Optimal Femoral Approaches: Mastering the Lateral Intermuscular Septum
Key Takeaway
Your ultimate guide to Optimal Femoral Approaches: Mastering the Lateral Intermuscular Septum starts here. Surgical approaches to the femur, including lateral, posterolateral, anterolateral, and anteromedial, are designed to access the bone. While some, like the lateral approach, involve splitting muscles such as the vastus lateralis, others utilize internervous planes to minimize trauma. Key anatomical structures, including the lateral intermuscular septum, guide these approaches for safe and effective femoral surgery.
Comprehensive Introduction and Patho-Epidemiology

Operations on the femur constitute a foundational pillar of orthopedic traumatology and reconstructive surgery. The bimodal epidemiological distribution of femoral fractures—characterized by high-energy mechanisms in the young, polytraumatized demographic and low-energy fragility fractures in the geriatric population—demands a versatile and masterful command of femoral surgical approaches. Historically, the lateral approach to the proximal femur was the undisputed gold standard, serving as the primary corridor for the treatment of an ever-growing incidence of intertrochanteric hip fractures. Before the widespread advent and refinement of proximal femoral intramedullary nailing systems, this approach was arguably the most frequently executed surgical exposure in all of orthopedic surgery, relying heavily on the robust vascularity and forgiving nature of the vastus lateralis muscle.
The evolution of orthopedic surgery has increasingly favored biology-preserving techniques, shifting the paradigm from extensile, periosteum-stripping exposures to minimally invasive plate osteosynthesis (MIPO) and closed intramedullary nailing. Despite this evolution, the fundamental principles of open femoral approaches remain indispensable. The four basic approaches to the femoral shaft—namely the lateral, posterolateral, anterolateral, and anteromedial—all require navigation through or around elements of the quadriceps muscle complex. While only the posterolateral approach exploits a true internervous plane, all of these approaches are considered relatively safe. This safety profile is predicated on the proximal arborization of the femoral nerve, which supplies the quadriceps femoris, allowing the more distal muscular elements to be split or mobilized without risking profound denervation.
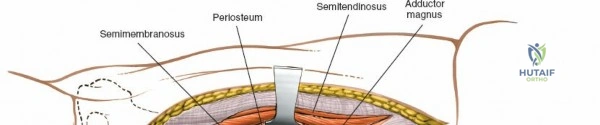
Mastery of the lateral intermuscular septum is particularly critical for surgeons tackling complex diaphyseal and distal femoral pathology. This fascial condensation not only serves as a reliable anatomical landmark but also acts as a crucial barrier protecting the posterior neurovascular structures. The posterolateral approach, which meticulously follows this septum, avoids splitting the vastus lateralis muscle belly directly, thereby preserving the dynamic function of the extensor mechanism. However, because the vastus lateralis originates in part from the lateral intermuscular septum itself, surgical mobilization still necessitates the detachment of these muscular origins, making the dissection demanding but highly rewarding for extensive distal exposures.
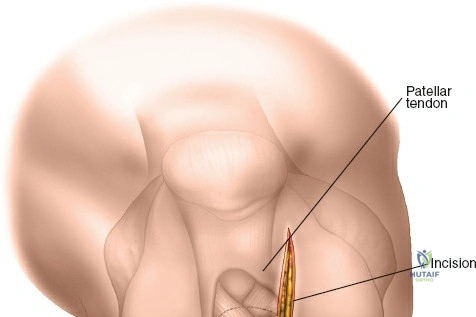
Modern femoral surgery requires a nuanced understanding of when to employ extensile open techniques versus minimally invasive windows. The minimally invasive approach to the distal femur, for instance, ingeniously utilizes two distinct windows: a distal window derived from the lateral parapatellar approach to the knee, and a proximal window derived from the classic lateral approach to the femoral shaft. As with all minimally invasive techniques, the reliance on intraoperative fluoroscopic imaging is absolute. Whether executing a closed intramedullary nailing via a minimally invasive proximal approach or performing a complex open reduction and internal fixation (ORIF) of a periprosthetic fracture, the surgeon's intimate knowledge of the thigh's cross-sectional anatomy and intermuscular septa dictates the success of the procedure and the rapidity of patient recovery.
Detailed Surgical Anatomy and Biomechanics
The femur is the longest, heaviest, and strongest bone in the human body, designed to withstand immense biomechanical forces. Structurally, the femoral shaft exhibits an anterior bow, which is critical for accommodating the massive extensor musculature and distributing axial loads. Biomechanically, the femur is subjected to eccentric loading during the normal gait cycle, resulting in high tensile forces along its lateral cortex and high compressive forces along its medial cortex. This fundamental biomechanical principle dictates the placement of load-bearing implants; tension-band constructs (such as laterally applied plates) must be robust enough to resist these tensile forces, while intramedullary devices are positioned closer to the mechanical axis to share the load more symmetrically.
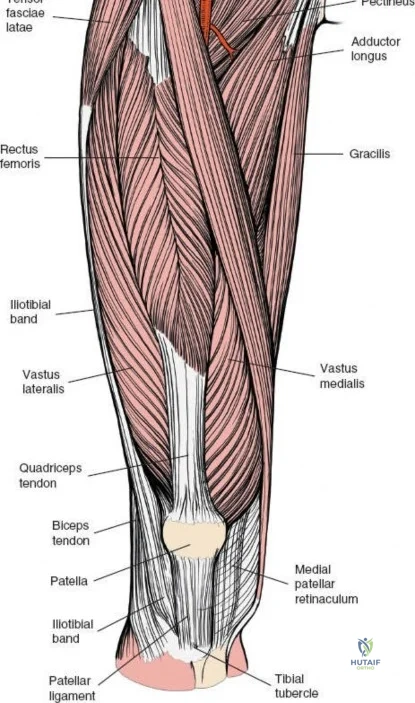
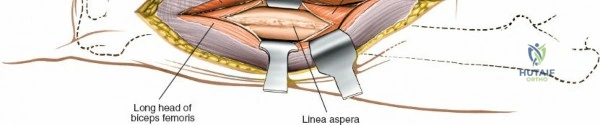
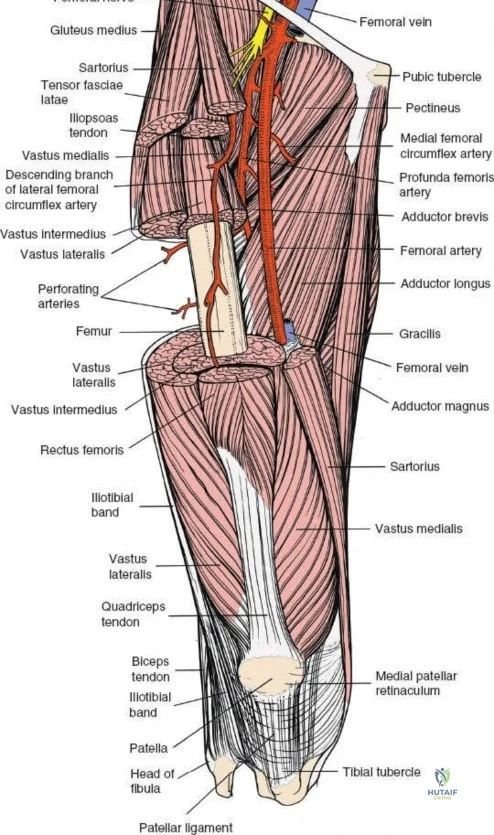
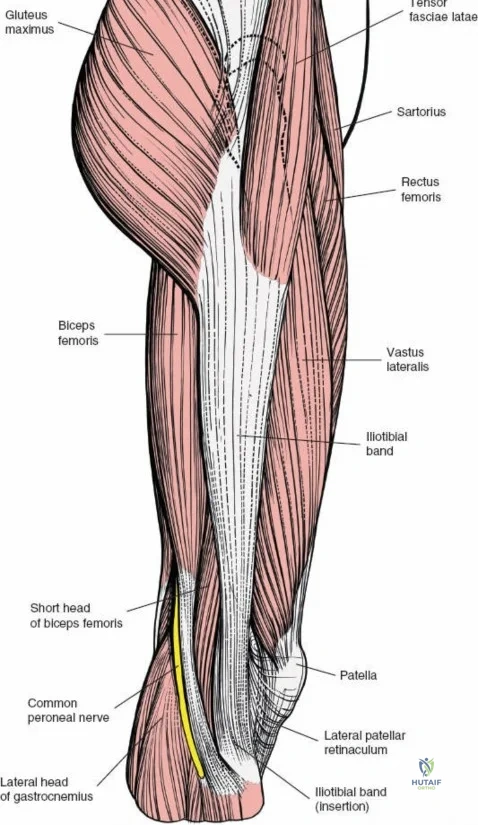
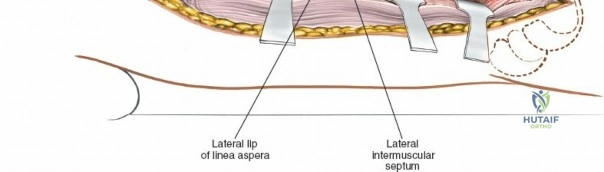
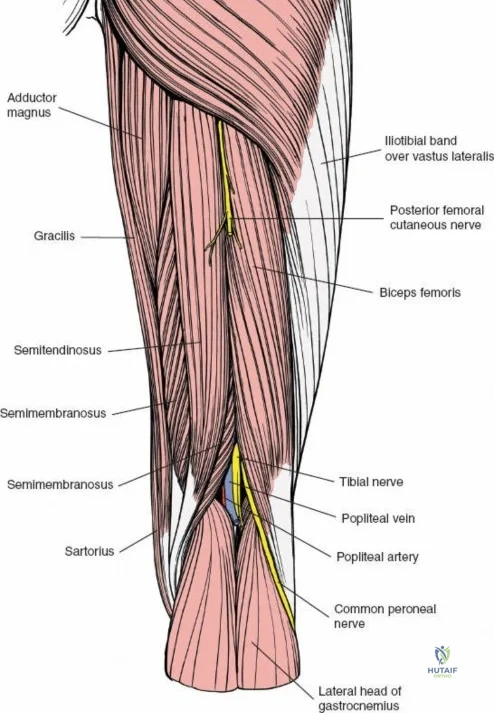
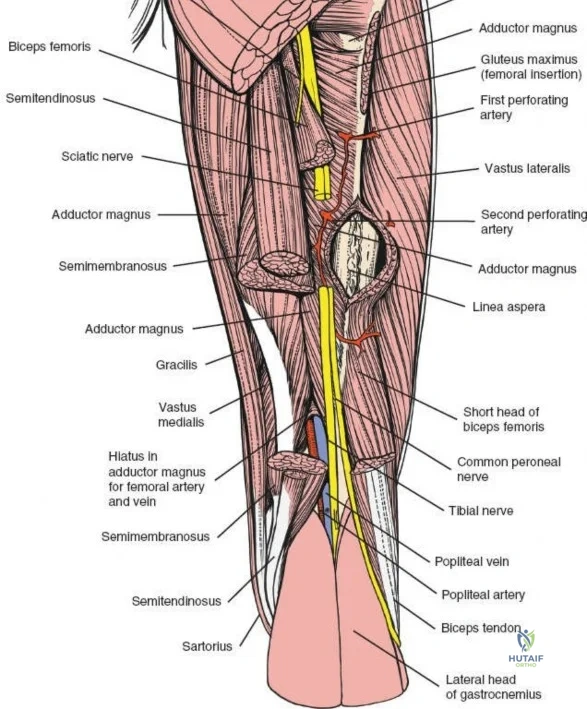
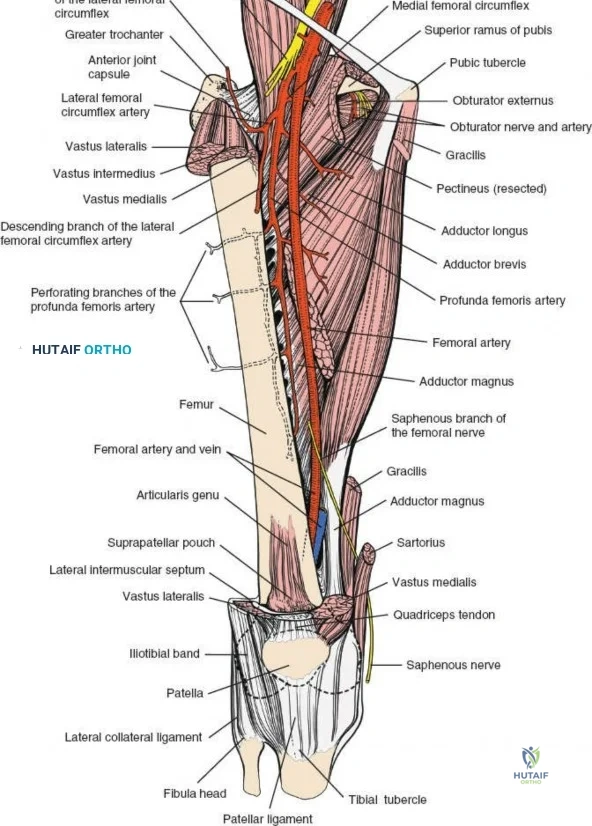
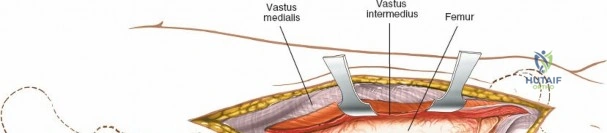
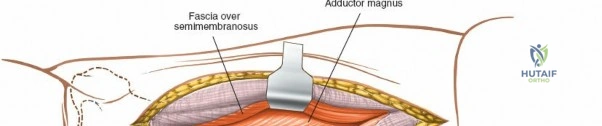
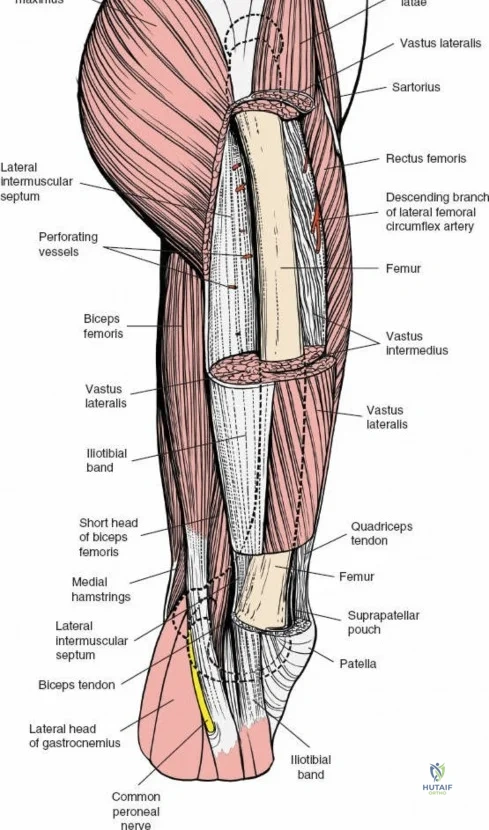
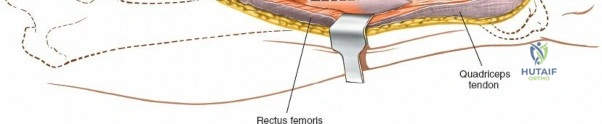
The musculature of the thigh is compartmentalized by thick fascial septa derived from the fascia lata. The anterior compartment contains the quadriceps femoris (rectus femoris, vastus lateralis, vastus medialis, and vastus intermedius) and the sartorius, all primarily innervated by the femoral nerve. The medial compartment houses the adductor group, innervated by the obturator nerve. The posterior compartment contains the hamstrings, innervated by the sciatic nerve. The lateral intermuscular septum is the thickest and most surgically relevant of these dividers, separating the vastus lateralis anteriorly from the short head of the biceps femoris posteriorly. It attaches firmly to the linea aspera, the prominent longitudinal ridge on the posterior aspect of the femur, which serves as the primary site of muscular origin and insertion.
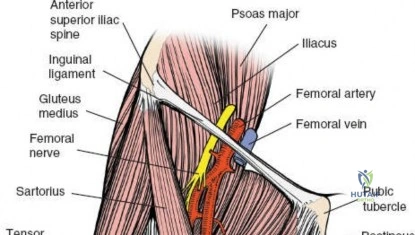
Vascular anatomy within the thigh is notoriously unforgiving and requires meticulous surgical respect. The key vascular structures spiral down the thigh, passing in an anterior to posterior direction. The superficial femoral artery travels within the subsartorial (Hunter’s) canal and transitions into the popliteal artery as it passes through the adductor hiatus. However, it is the profunda femoris artery—the deep artery of the thigh—that poses the greatest challenge during lateral and posterolateral approaches. The profunda femoris gives rise to multiple perforating branches (typically three to four) that pierce the adductor magnus and the lateral intermuscular septum to supply the posterior and lateral musculature. These perforating arteries traverse the vastus lateralis muscle and are intimately applied to the linea aspera.
During the lateral approach, which involves splitting the vastus lateralis, these perforating vessels are inevitably encountered. Because they are tethered by the fascial septa and the muscle itself, they are highly susceptible to avulsion during blunt dissection. If severed, these vessels rapidly retract into the muscle belly or behind the intermuscular septum, leading to profound, difficult-to-control hemorrhage. Consequently, precise identification, isolation, and prophylactic coagulation or ligation of these perforators are mandatory steps. The posterolateral approach, while avoiding a direct muscle split, requires elevating the vastus lateralis off the lateral intermuscular septum, exposing these perforators directly at their point of septal penetration, demanding equal vigilance and meticulous hemostatic technique.
Exhaustive Indications and Contraindications

The selection of a specific femoral approach is dictated by the fracture morphology, the presence of concomitant injuries, the planned fixation construct, and the patient's soft tissue envelope. The classic lateral approach remains the workhorse for the proximal third of the femur. Its primary indication is the open reduction and internal fixation of intertrochanteric and subtrochanteric fractures, particularly when utilizing dynamic hip screws or proximal femoral locking plates. It is also the standard approach for the insertion of internal fixation in the treatment of slipped capital femoral epiphysis (SCFE) and basicervical femoral neck fractures. Furthermore, the lateral approach is highly versatile; it can be utilized for subtrochanteric or intertrochanteric osteotomies, extra-articular arthrodesis of the hip joint, and the biopsy or wide excision of bone tumors located in the proximal or mid-diaphysis.
The posterolateral approach, by contrast, is uniquely suited for pathology involving the middle and distal thirds of the femoral shaft. Because it exploits the plane along the lateral intermuscular septum, it allows for extensive exposure of the linea aspera and the posterior cortex. This makes it ideal for the open reduction and plating of complex, comminuted supracondylar fractures where posterior cortical continuity must be visually restored. It is also the preferred approach for treating atrophic or hypertrophic nonunions of the femoral shaft, as it provides excellent access for decortication and the application of autologous bone graft without severely compromising the anterior muscular envelope. Additionally, if facilities for closed intramedullary nailing are unavailable, the posterolateral approach provides excellent access for open intramedullary nail placement.

Contraindications to these approaches are generally relative and heavily dependent on the local soft tissue status. Severe soft tissue compromise, such as deep abrasions, degloving injuries (Morel-Lavallée lesions), or active superficial infections over the lateral thigh, strictly precludes the use of a direct lateral or posterolateral incision due to the unacceptably high risk of deep postoperative infection. In cases where the patient has undergone previous surgeries utilizing posterior or medial flaps, the vascular supply to the remaining skin bridges must be carefully evaluated to prevent full-thickness skin necrosis. The posterior approach to the femur is rarely used for fracture fixation and is explicitly reserved for the exploration of the sciatic nerve or for patients who cannot undergo more anterior approaches due to severe anterior skin problems.
| Indication/Contraindication Parameter | Lateral Approach | Posterolateral Approach | Minimally Invasive (MIPO) |
|---|---|---|---|
| Primary Indications | Intertrochanteric fractures, subtrochanteric fractures, proximal osteotomies, tumor biopsies. | Distal third shaft fractures, supracondylar fractures, diaphyseal nonunions, open IM nailing. | Distal femur articular/extra-articular fractures, periprosthetic fractures. |
| Optimal Fixation Implants | Dynamic Hip Screws (DHS), Proximal Femoral Locking Plates, Cephalomedullary Nails (entry). | Broad Dynamic Compression Plates (DCP), Distal Femoral Locking Plates, Open IM Nails. | Distal Femoral Locking Plates (LISS), Retrograde IM Nails. |
| Absolute Contraindications | Active lateral soft tissue infection, unhealed lateral burns/grafts. | Active lateral/posterior infection, severe peripheral vascular disease with posterior flap risk. | Inability to obtain adequate closed reduction, lack of fluoroscopy. |
| Relative Contraindications | Severe medial comminution requiring direct medial buttress plating (requires medial approach). | Extensive proximal shaft involvement (requires excessive vastus lateralis retraction). | Highly comminuted articular fractures requiring direct visualization of the joint block. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the cornerstone of successful femoral surgery. High-quality, orthogonal radiographs of the entire femur, including the hip and knee joints, are mandatory to rule out ipsilateral segmental fractures or femoral neck fractures, which occur in up to 10% of high-energy femoral shaft fractures. For complex distal femoral fractures or those with suspected intra-articular extension, a fine-cut computed tomography (CT) scan with 2D and 3D reconstructions is essential for understanding the fracture morphology and planning the sequence of reduction. Digital templating using calibrated radiographs allows the surgeon to accurately determine the required plate length, screw trajectory, and the optimal entry point for intramedullary nails. This significantly reduces intraoperative decision-making time and ensures that the appropriate hardware inventory is available.
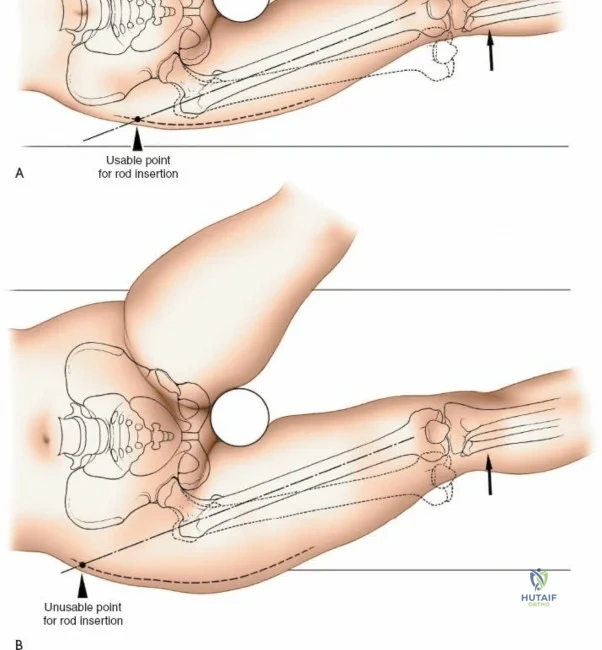
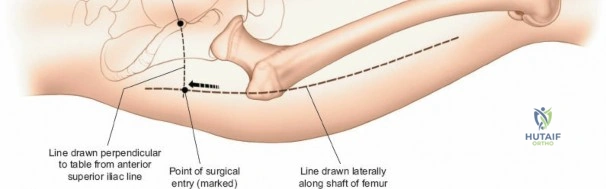
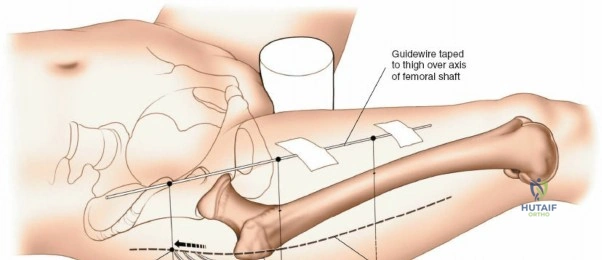
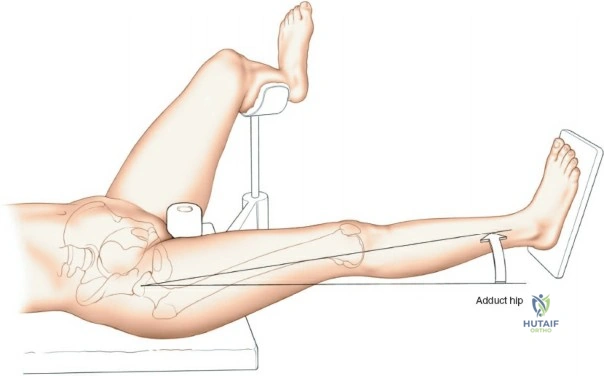
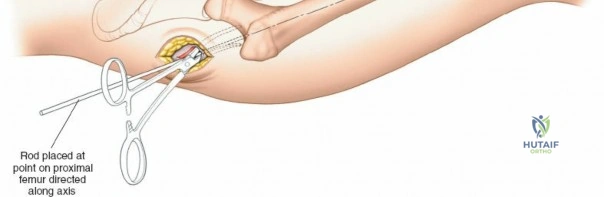
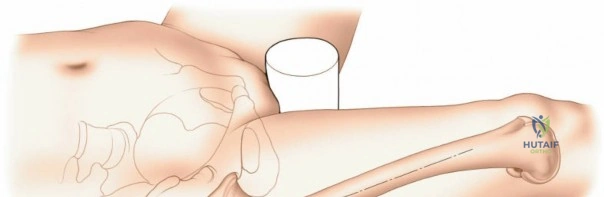
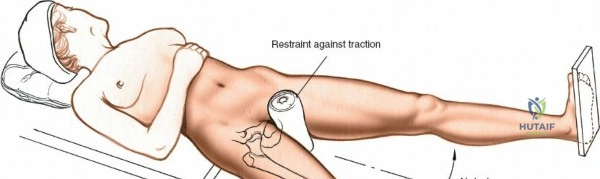
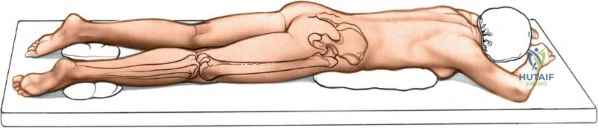
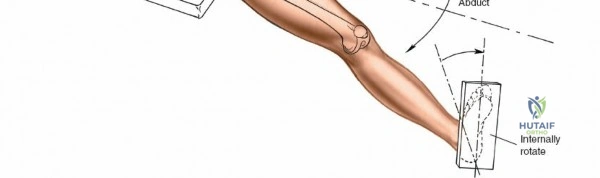
Patient positioning is a critical step that dictates the ease of the surgical approach and the quality of intraoperative imaging. For the lateral approach to the proximal femur, particularly for trochanteric fractures, the patient is typically placed supine on an orthopedic fracture table. This specialized table allows for skeletal traction and precise manipulation of the extremity. The affected leg is internally rotated approximately 15 degrees to overcome the natural anteversion of the femoral neck, bringing the lateral surface of the greater trochanter and proximal shaft into a true lateral position relative to the floor. This internal rotation is crucial for accurate fracture reduction in extracapsular hip fractures and ensures that the femoral neck is parallel to the floor, which greatly facilitates the correct positioning of the femoral neck guidewire under fluoroscopy.
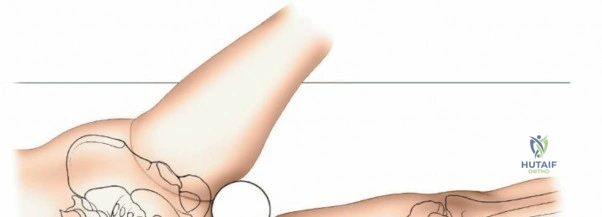
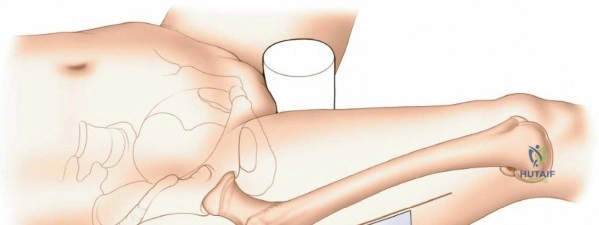
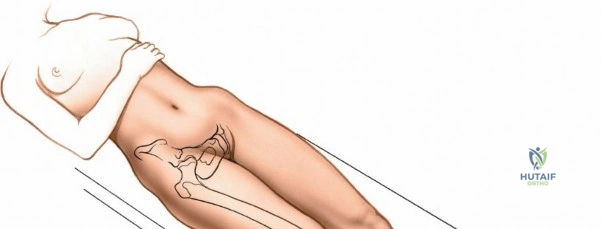
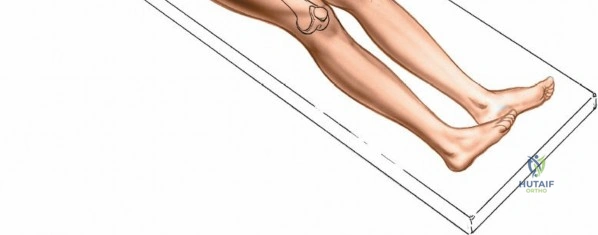
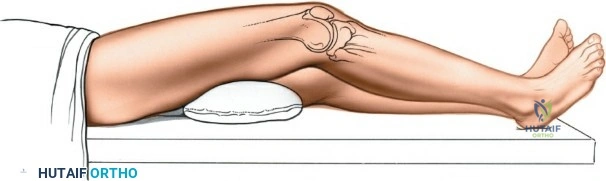
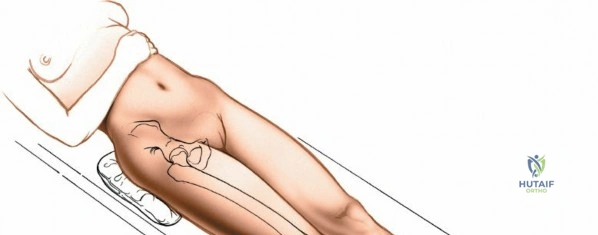
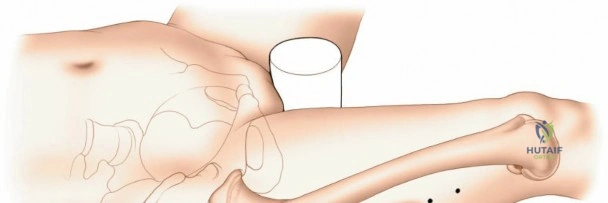
Conversely, for surgery on the diaphyseal shaft of the femur, especially when utilizing the posterolateral approach, a lateral decubitus or "floppy lateral" position is frequently employed. The patient is placed on their side with the affected limb uppermost. It is imperative to meticulously pad the bony prominences of the dependent limb (such as the fibular head and lateral malleolus) to avoid iatrogenic pressure necrosis or peroneal nerve palsy. An axillary roll is placed to protect the dependent brachial plexus. Pillows or a sterile foam ramp are placed between the two limbs to pad the medial surface of the operative knee and medial malleolus. Alternatively, the patient can be placed supine with a large sandbag or bump placed beneath the ipsilateral buttock. This elevates the hip and internally rotates the leg, bringing the posterolateral surface of the thigh clear of the operating table and allowing gravity to assist in retracting the posterior musculature.
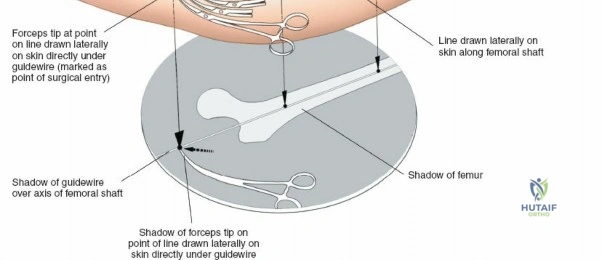
Fluoroscopy setup must be integrated into the positioning plan before the patient is prepped and draped. The C-arm image intensifier should be positioned such that it can easily swing between anteroposterior (AP) and lateral views without compromising the sterile surgical field or colliding with the operating table. For proximal femoral procedures on a fracture table, the C-arm is usually positioned between the patient's legs, allowing for unobstructed imaging of the femoral neck and head. For distal or diaphyseal procedures, the C-arm typically enters from the contralateral side of the table. The surgeon must verify that adequate, high-quality images of the entire planned surgical field can be obtained prior to making the incision, as intraoperative adjustments to positioning are cumbersome and increase the risk of breaking sterility.
Step-by-Step Surgical Approach and Fixation Technique

The Lateral Approach to the Proximal Femur
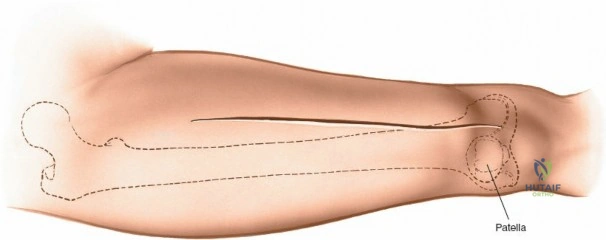
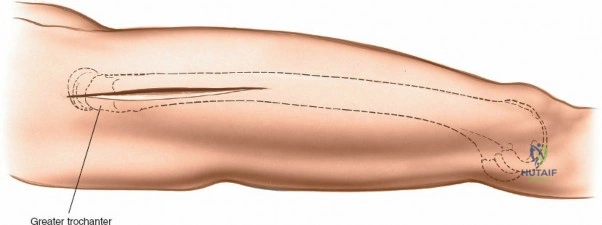
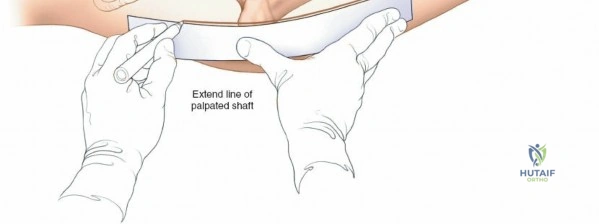
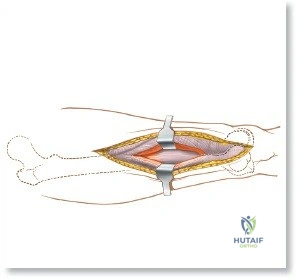
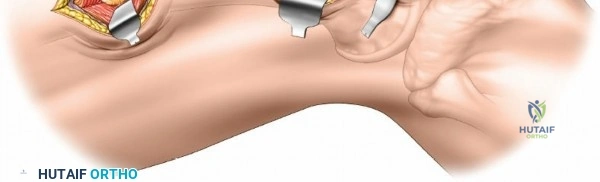
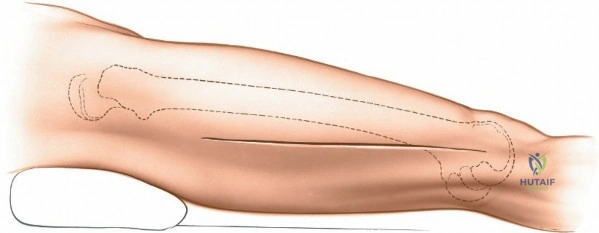
The lateral approach is initiated by identifying the critical bony landmarks. The posterior edge of the greater trochanter is relatively uncovered by muscle and serves as the primary proximal landmark. The surgeon palpates this edge, moving the fingers anteriorly and proximally to identify the tip of the trochanter. Extending distally, the shaft of the femur is palpable as a firm line of resistance on the lateral side of the thigh. A longitudinal skin incision is made, beginning over the middle of the greater trochanter and extending distally down the lateral aspect of the thigh. The exact length and position of the incision are tailored to the specific requirements of the planned fixation. Utilizing preoperative and intraoperative radiographic control to accurately site the incision significantly reduces unnecessary soft tissue dissection and minimizes morbidity.
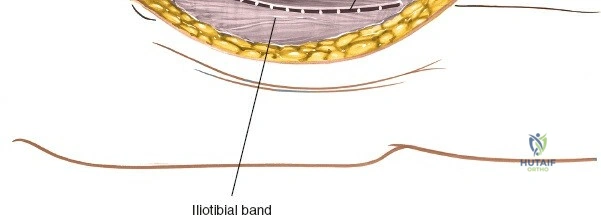
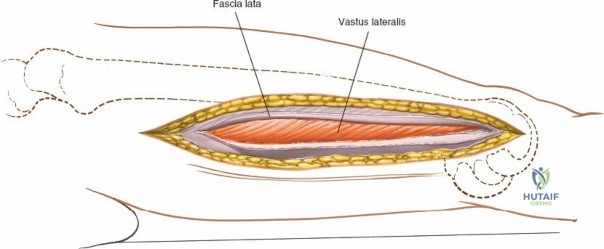
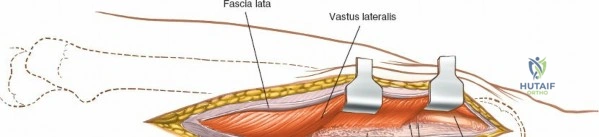
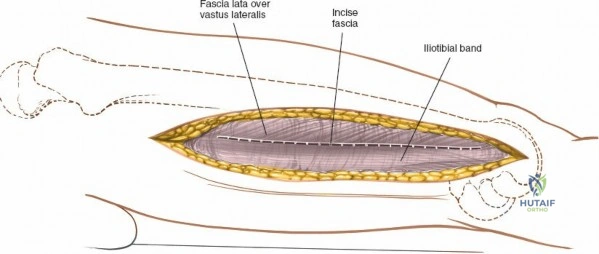
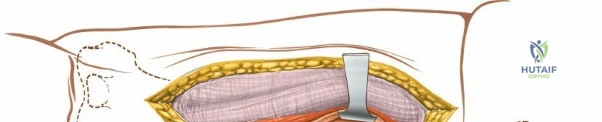
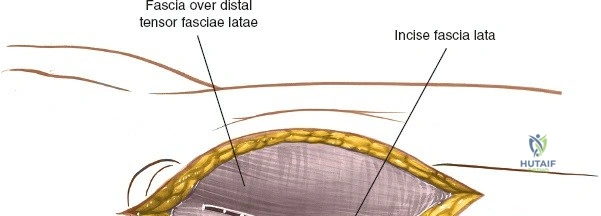
Following the skin incision, the subcutaneous tissues are divided in line with the incision to expose the glistening white fascia lata. The fascia lata is incised longitudinally. At the proximal extent of the wound, the distal tendinous fibers of the tensor fasciae latae muscle may be encountered. In approximately one-third of patients, these fibers extend distally beyond the greater trochanter and must be split in line with their fibers to fully expose the underlying vastus lateralis muscle. Once the fascia lata is open, it is retracted anteriorly and posteriorly, revealing the vastus lateralis enveloped in its thin epimysium. There is no true internervous plane here; the approach relies on splitting the vastus lateralis, which is safe because the femoral nerve innervates the muscle well proximal to the surgical field.
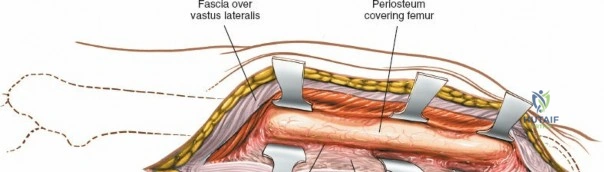
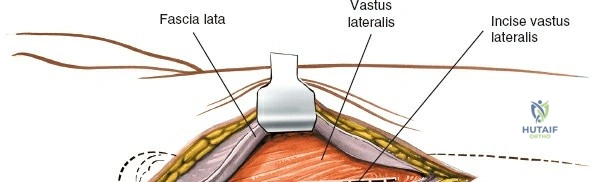
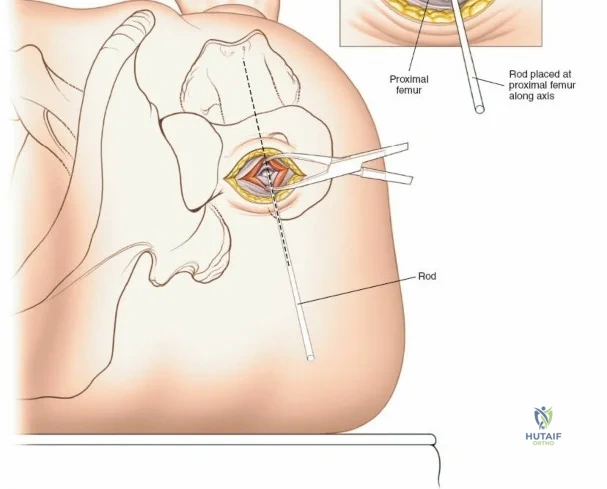
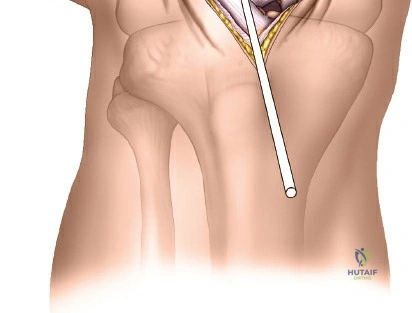
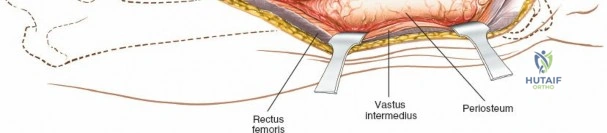
Deep dissection begins by carefully incising the fascial covering of the vastus lateralis. A Hohmann or Bennett retractor is inserted through the muscle fibers, running the blunt tip over the anterior aspect of the femoral shaft to hook over the anterior cortex. A second retractor is inserted through the same gap, manipulated underneath the femur to hook the posterior cortex. By pulling these two retractors apart, the vastus lateralis is split longitudinally in the line of its fibers. This splitting must be performed via blunt dissection rather than sharp scalpel cuts. As the muscle fibers separate, numerous perforating branches of the profunda femoris artery will be encountered traversing the muscle belly. These vessels must be meticulously identified, isolated, and coagulated or ligated before they are avulsed. Sharp dissection straight down to the bone is strongly discouraged, as severed vessels will rapidly retract into the muscle mass, making hemostasis exceedingly difficult and leading to significant postoperative hematoma.
The Posterolateral Approach to the Femoral Shaft
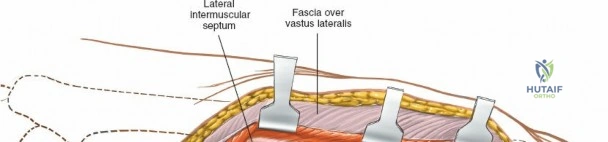
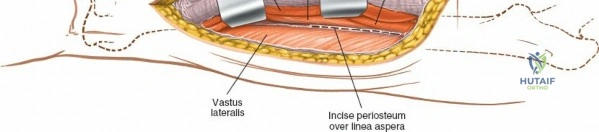
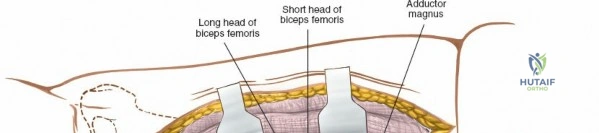
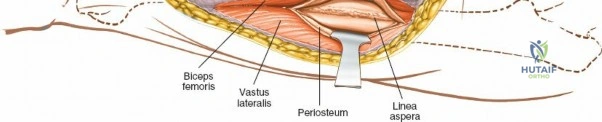
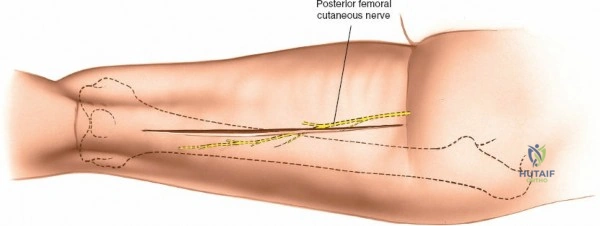
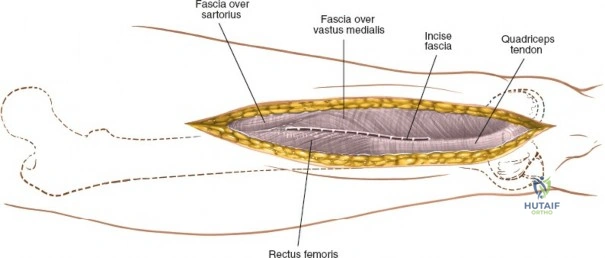
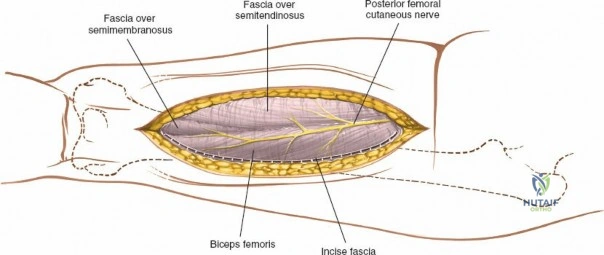
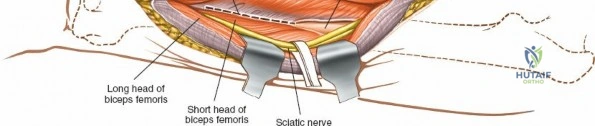
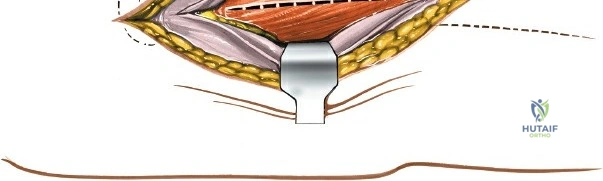
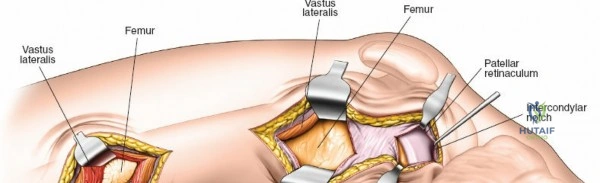
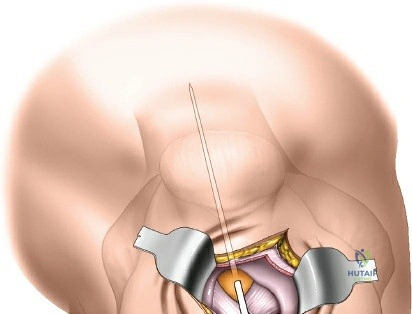
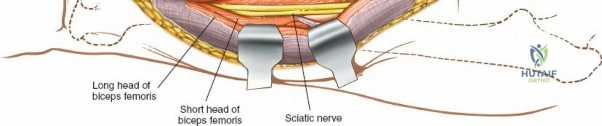
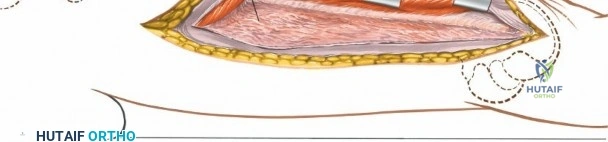
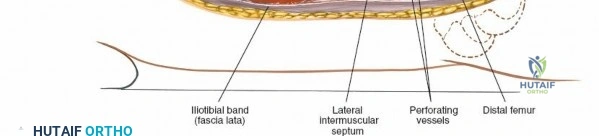
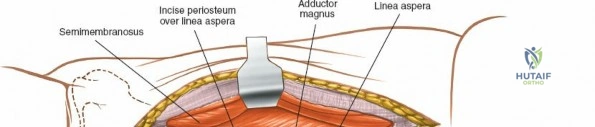
The posterolateral approach is designed to expose the entire length of the femur without splitting the vastus lateralis muscle belly, utilizing the plane of the lateral intermuscular septum. The patient is positioned appropriately (supine with a bump or lateral decubitus), and a longitudinal incision is made along the posterolateral aspect of the thigh, aligned with the palpable lateral intermuscular septum. The fascia lata is incised in line with the skin incision. Deep to the fascia lata, the vastus lateralis is visualized anteriorly, and the short head of the biceps femoris is visualized posteriorly. The critical step is identifying the lateral intermuscular septum, which appears as a thick, white fascial band separating these two muscle groups.


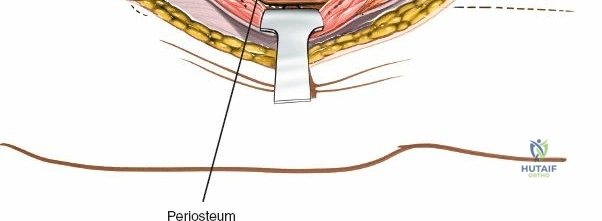
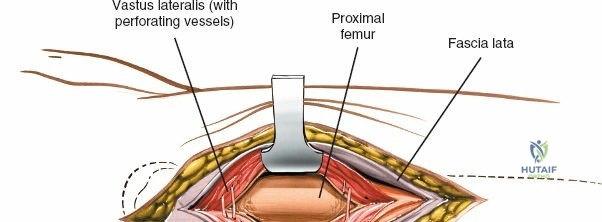
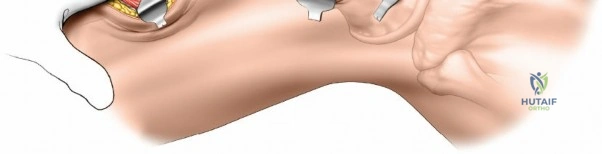
Deep dissection involves elevating the vastus lateralis anteriorly off the lateral intermuscular septum. This is a deliberate, subperiosteal dissection. The surgeon starts distally, where the septum is most prominent, and works proximally. As the vastus lateralis is retracted anteriorly, the surgeon must be acutely aware of the perforating branches of the profunda femoris artery. These vessels pierce the lateral intermuscular septum close to its attachment to the linea aspera. They must be systematically identified, clamped, and securely ligated or coagulated with bipolar electrocautery right at the septal border. Failure to secure these perforators at the septum will result in catastrophic bleeding that retracts posteriorly into the thigh. Once the vastus lateralis is fully mobilized and retracted anteriorly with deep Hohmann retractors, the entire posterolateral surface of the femur and the linea aspera are brilliantly exposed for fracture reduction and plate application.
Minimally Invasive and Extensile Adaptations
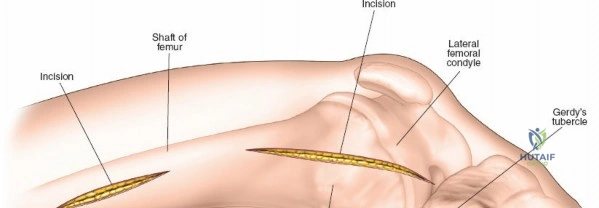
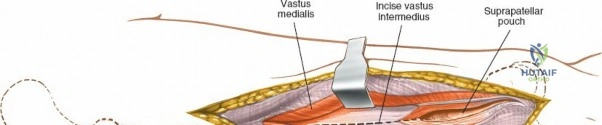
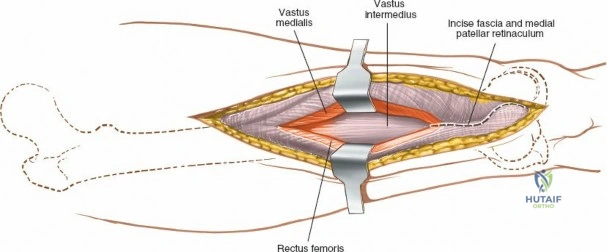
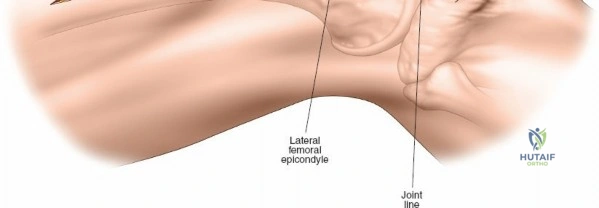
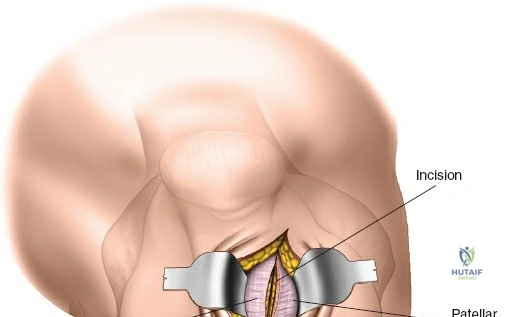
Modern orthopedic trauma heavily utilizes minimally invasive approaches, particularly for the distal femur. The MIPO approach to the distal femur utilizes two distinct windows. The distal window is derived from a lateral parapatellar approach, allowing visualization of the lateral femoral condyle and the knee joint for articular reduction. The proximal window is a small 3-5 cm incision derived from the standard lateral approach to the femoral shaft. A submuscular, extraperiosteal tunnel is created between these two windows using a blunt elevator. A pre-contoured distal femoral locking plate is then slid submuscularly from distal to proximal. This technique preserves the fracture hematoma and the periosteal blood supply, drastically improving union rates. However, it requires absolute reliance on intraoperative fluoroscopy to ensure correct plate positioning, restoration of limb alignment, and avoidance of neurovascular injury during percutaneous screw insertion.
When necessary, the standard lateral approach is highly extensile. It is most frequently used for exposing the proximal third of the bone for internal fixation of a hip fracture, but the incision can be seamlessly extended distally all the way to the lateral epicondyle of the knee joint. This allows for full, unhindered exposure of the entire lateral aspect of the femoral shaft, which is occasionally required for the reduction and fixation of highly comminuted, segmental femoral fractures that cannot be managed with closed intramedullary nailing. During closure of any lateral approach, it is imperative to meticulously repair the fascia lata. Failure to achieve a robust fascial closure can result in painful muscle herniation of the vastus lateralis through the fascial defect, leading to chronic lateral thigh pain and functional impairment.
Complications, Incidence Rates, and Salvage Management
Complications associated with femoral approaches and subsequent fixation are multifaceted, ranging from acute intraoperative events to chronic mechanical failures. The most immediate and potentially life-threatening complication is massive hemorrhage. As previously emphasized, the perforating branches of the profunda femoris artery are the primary culprits. If a perforator is avulsed and retracts into the deep posterior compartment, blind clamping is strictly contraindicated due to the proximity of the sciatic nerve. Salvage management requires immediate packing of the wound with laparotomy sponges, application of direct pressure, and, if bleeding is uncontrollable, extension of the exposure to directly visualize the retracted vessel. In extreme cases, temporary closure and emergent transfer to interventional radiology for selective angiographic embolization may be life-saving.
Infection and wound healing complications remain a significant concern, particularly in extensile open approaches. The incidence of deep surgical site infection (SSI) following open plating of the femur ranges from 2% to 5%, but this rate increases exponentially in patients with comorbidities such as morbid obesity, poorly controlled diabetes mellitus, and active tobacco use. Meticulous soft tissue handling, frequent irrigation, and minimization of periosteal stripping are paramount. If a deep SSI occurs, salvage management mandates aggressive surgical debridement, hardware retention (if the construct is stable), and the application of targeted intravenous antibiotic therapy. In cases of severe soft tissue defects, the use of negative pressure wound therapy (NPWT) and eventual coverage with rotational or free muscle flaps may be required.
Mechanical complications, including aseptic nonunion and hardware failure, are deeply tied to the biomechanical principles of the femur. Varus collapse is a common mode of failure in proximal femoral fractures treated with lateral plating, often resulting from inadequate restoration of the medial calcar buttress or the use of a plate that is too short to withstand the lateral tensile forces. Diaphyseal nonunions occur in approximately 1-10% of cases, heavily dependent on the degree of initial trauma and the preservation of biology. Salvage management for nonunion typically involves revision surgery. Hypertrophic nonunions, indicating adequate biology but inadequate stability, are treated with hardware revision to a more rigid construct (e.g., exchanging a plate for a larger reamed intramedullary nail). Atrophic nonunions require biological augmentation, frequently necessitating decortication via a posterolateral approach and the application of autologous iliac crest bone graft (ICBG) or bone morphogenetic proteins (BMP).
| Complication | Estimated Incidence | Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Hemorrhage (Profunda Perforators) | 1 - 3% | Blunt avulsion, poor visualization, sharp deep dissection. | Immediate packing, extension of exposure, selective angiographic embolization. |
| Deep Surgical Site Infection (SSI) | 2 - 5% (Open) | Obesity, Diabetes, Smoking, prolonged operative time. | Serial I&D, hardware retention if stable, targeted IV antibiotics, NPWT. |
| Aseptic Nonunion | 1 - 10% | Severe comminution, periosteal stripping, smoking. | Revision fixation (nail exchange or plate revision), autologous bone grafting. |
| Hardware Failure (Varus Collapse) | 2 - 8% | Medial cortical comminution, osteopenia, premature weight-bearing. | Revision to cephalomedullary nail or medial buttress plating, correction of |
Clinical & Radiographic Imaging Archive