Advanced Bilateral Simultaneous THA: Uncemented Monobloc Case Title

Key Takeaway
Discover the latest medical recommendations for Advanced Bilateral Simultaneous THA: Uncemented Monobloc Case Title. A **case title bilateral** hip arthroplasty addresses severe conditions like advanced bilateral osteoarthritis, osteonecrosis, or rheumatoid arthritis. This often involves simultaneous total hip arthroplasty using components such as monobloc acetabular all poly or cemented implants. The goal is to restore function, alleviate pain from joint obliteration, and facilitate early rehabilitation and long-term prosthesis survival.
Patient Presentation and History
A 62-year-old male presented with a 5-year history of progressively worsening bilateral hip pain, more pronounced on the left, severely limiting his activities of daily living. The pain was described as deep, aching, and localized to the groin and buttock, radiating to the anterior thigh. It was exacerbated by weight-bearing activities, prolonged standing, and initiation of movement after rest. Night pain and difficulty sleeping were reported, indicating advanced joint degeneration. He ambulated with a significant antalgic gait and required a single-point cane for distances greater than 50 meters. He denied any preceding trauma, inflammatory episodes, or neurological deficits.
Conservative management over the preceding 36 months had failed. This included extensive physical therapy focusing on abductor strengthening, continuous use of non-steroidal anti-inflammatory drugs (NSAIDs), activity modification, and two sequential intra-articular corticosteroid injections bilaterally, which provided only transient relief lasting less than three weeks per injection. His preoperative Harris Hip Score (HHS) was calculated at 42 for the left hip and 48 for the right hip, indicative of severe functional impairment.
Demographics and Comorbidities
- Age: 62 years
- Sex: Male
- Occupation: Retired accountant
- BMI: 28 kg/m²
- Controlled hypertension (managed with lisinopril 10mg daily)
- Type 2 Diabetes Mellitus (HbA1c 6.8%, managed with metformin 1000mg BID)
- Hyperlipidemia (managed with atorvastatin 40mg daily)
- No history of previous hip surgery, deep vein thrombosis (DVT), pulmonary embolism (PE), or cardiac events.
- ASA physical status classification: II
Etiology of Hip Pathology
His history and initial workup were consistent with primary osteoarthritis, advanced bilaterally. There was no clear history suggestive of developmental dysplasia of the hip (DDH), Legg-Calve-Perthes disease, or slipped capital femoral epiphysis (SCFE) in childhood, nor significant trauma leading to post-traumatic arthritis. While avascular necrosis (AVN) was considered in the differential, clinical and radiological features did not strongly support it as the primary etiology. The progressive nature of his symptoms, coupled with characteristic radiographic findings, pointed towards idiopathic degenerative arthritis.
Clinical Examination Findings
General Inspection and Gait Analysis
The patient appeared comfortable at rest but exhibited a pronounced antalgic gait with a shortened stance phase on both lower limbs, significantly more pronounced on the left. A bilateral abductor lurch (Trendelenburg gait) was noted during ambulation, compensating for gluteus medius insufficiency secondary to chronic pain and altered joint mechanics. No significant structural limb length discrepancy was grossly apparent upon block testing, though a functional discrepancy was noted due to pelvic obliquity and fixed flexion contractures. Mild bilateral quadriceps and gluteal atrophy was observed. No skin changes, scars, or overt deformities around the hips were present.
Palpation and Neurovascular Status
Tenderness was elicited over the anterior groin capsule and greater trochanteric regions bilaterally, consistent with capsular distension, osteophytic impingement, and secondary trochanteric bursitis. No palpable masses, gross crepitus, or localized warmth were noted.
Peripheral pulses (femoral, popliteal, dorsalis pedis, posterior tibial) were 2+ and symmetrical bilaterally. Capillary refill was less than 2 seconds. The neurovascular status was unremarkable, effectively ruling out vascular claudication as a primary source of lower extremity pain.
Range of Motion Assessment
All measurements were taken with the patient supine using a goniometer. The Thomas test was utilized to accurately quantify the fixed flexion deformities.
Right Hip
* Flexion: 90° (painful at end range)
* Extension: 0°
* Abduction: 20° (painful)
* Adduction: 10°
* Internal Rotation: 5° (severely painful, indicating anterior capsular contracture)
* External Rotation: 15°
* Fixed flexion deformity: 10°
Left Hip
* Flexion: 80° (painful at end range)
* Extension: 0°
* Abduction: 15° (severely painful)
* Adduction: 5°
* Internal Rotation: 0° (excruciatingly painful)
* External Rotation: 10°
* Fixed flexion deformity: 15°
Neurological Assessment
Motor strength was graded 5/5 in all major muscle groups of both lower extremities, including hip flexors (L2-L3), extensors (S1), abductors (L5), adductors (L2-L4), knee flexors (S1), knee extensors (L3-L4), ankle dorsiflexors (L4-L5), and plantarflexors (S1). No focal neurological weakness was detected. Sensory examination revealed intact light touch and pinprick sensation across all L1-S1 dermatomes bilaterally. Patellar and Achilles deep tendon reflexes were 2+ and symmetrical. The absence of radicular symptoms, negative straight leg raise, and normal neurological exam significantly lowered the probability of concurrent lumbar spinal stenosis or radiculopathy.
Imaging and Diagnostics
Standard preoperative radiographs included an anteroposterior (AP) pelvis centered over the symphysis pubis with 15 degrees of internal rotation of the lower extremities to profile the femoral necks, alongside true lateral and Dunn lateral views of both hips.
Radiographic Findings

The AP Pelvis radiograph demonstrated severe, bilateral tricompartmental joint space narrowing. The left hip exhibited complete obliteration of the superior and axial joint spaces with bone-on-bone articulation. Subchondral sclerosis was prominent bilaterally, accompanied by marginal osteophyte formation at the femoral head-neck junction and the acetabular rim. Large subchondral cysts (geodes) were visible in the superior weight-bearing dome of the left acetabulum.
The lateral view of the left hip confirmed the loss of sphericity of the femoral head, extensive anterior and posterior osteophytosis, and severe joint space collapse.

The lateral view of the right hip demonstrated similar but slightly less advanced degenerative changes, with marked loss of anterior joint space and reactive subchondral bone formation.
Preoperative Templating
Digital templating was performed to determine the optimal component size, restore the center of rotation, equalize leg lengths, and optimize femoral offset.

Templating established the following parameters:
* Center of Rotation: The anatomical center of rotation was identified bilaterally. The templated acetabular components were positioned to restore this center, ensuring medialization to the true floor of the acetabulum (teardrop) without violating the Kohler line.
* Acetabular Sizing: Templating suggested a 54 mm multi-hole hemispherical titanium shell for the left and a 52 mm or 54 mm shell for the right, aiming for an inclination of 40 degrees and anteversion of 20 degrees.
* Femoral Sizing and Offset: A standard offset, uncemented monobloc titanium stem was templated. The monobloc design requires precise templating of the femoral canal to ensure rigid diaphyseal/metaphyseal fit while simultaneously achieving the correct neck length and offset, as there is no modular neck option. The templated cut was planned 15 mm above the lesser trochanter bilaterally to restore appropriate leg length and abductor tension.
* Bone Quality: According to the Dorr classification, the proximal femur exhibited Type B bone quality (cortices thick but with some widening of the medullary canal), which is highly amenable to uncemented, press-fit diaphyseal/metaphyseal fixation.
Differential Diagnosis
The diagnosis of primary osteoarthritis was clear based on clinical and radiographic parameters. However, a comprehensive differential diagnosis was considered to rule out secondary causes of joint destruction that might alter the surgical approach or postoperative medical management.
| Pathology | Clinical Presentation | Radiographic Hallmarks | Distinguishing Features in this Case |
|---|---|---|---|
| Primary Osteoarthritis | Chronic, progressive groin/buttock pain. Morning stiffness < 30 mins. Worse with weight-bearing. | Asymmetric joint space narrowing (superior migration), subchondral sclerosis, osteophytes, cysts. | Patient matches classic demographic, bilateral presentation, and characteristic radiographic findings. |
| Avascular Necrosis | Often sudden onset of pain. History of corticosteroid use, alcohol abuse, or trauma. | Crescent sign, subchondral collapse, preservation of joint space until late stages. | Lack of risk factors. Radiographs show global joint space loss and osteophytosis rather than isolated focal head collapse. |
| Inflammatory Arthropathy | Prolonged morning stiffness (>1 hour). Systemic symptoms. Bilateral symmetric involvement. | Symmetric joint space loss (axial migration), periarticular osteopenia, erosions, lack of osteophytes. | Absence of systemic symptoms, normal inflammatory markers (ESR/CRP), and presence of robust osteophyte formation. |
| Lumbar Radiculopathy | Pain radiating below the knee. Exacerbated by lumbar extension. Possible motor/sensory deficits. | Degenerative disc disease, facet arthropathy, neuroforaminal narrowing on MRI. | Normal neurological exam. Pain localized to groin. Negative straight leg raise. Severe ROM restriction in the hip. |
Surgical Decision Making and Classification
Indication for Operative Intervention
The patient presented with end-stage bilateral hip osteoarthritis, categorized as Tönnis Grade 3 bilaterally (large cysts, severe narrowing or obliteration of the joint space, severe deformity of the head). Given the failure of exhaustive non-operative modalities, the severe impairment of activities of daily living, and the profound impact on his quality of life, surgical intervention was definitively indicated.
Rationale for Bilateral Simultaneous THA
The decision to proceed with a simultaneous bilateral Total Hip Arthroplasty versus a staged procedure was carefully evaluated. The criteria for simultaneous bilateral THA generally include ASA classification I or II, age under 75, BMI under 30, and the absence of severe cardiopulmonary disease.
This patient met all criteria for a simultaneous approach. The advantages of a simultaneous procedure include a single anesthetic event, a single hospital stay, reduced overall rehabilitation time, and the immediate correction of bilateral fixed flexion deformities and functional limb length discrepancies, which greatly facilitates symmetric gait retraining. The primary risks—increased perioperative blood loss, higher risk of venous thromboembolism, and potential for fat embolism syndrome—were mitigated through an optimized Enhanced Recovery After Surgery (ERAS) protocol, meticulous surgical technique, and rigorous medical management.
Implant Selection Uncemented Monobloc System
An uncemented, porous-coated titanium acetabular shell with a highly cross-linked polyethylene liner and a ceramic femoral head was selected.
For the femur, an uncemented monobloc titanium stem was chosen. The rationale for a monobloc stem includes:
1. Elimination of Modularity: Monobloc stems eliminate the modular neck junction, completely eradicating the risk of trunnionosis, mechanically assisted crevice corrosion (MACC), and modular neck fracture.
2. Excellent Survivorship: Long-term registry data demonstrates exceptional survivorship for fully porous-coated or proximally coated monobloc stems in Dorr Type A and B bone.
3. Biomechanical Stability: The metaphyseal filling design provides immediate rigid primary stability, while the titanium plasma spray or hydroxyapatite coating facilitates rapid osseointegration (secondary stability).
The primary challenge of a monobloc stem is the inability to independently adjust version, offset, and leg length after the stem is seated. This necessitates meticulous preoperative templating and precise intraoperative execution of the femoral neck cut and broaching sequence.
Surgical Technique and Intervention
Preoperative Preparation and Anesthesia
The patient was optimized via our institutional ERAS pathway. Pre-emptive multimodal analgesia (acetaminophen 1000mg, celecoxib 200mg, and gabapentin 300mg) was administered. Intravenous tranexamic acid (TXA) 1 gram was given prior to incision, with a second 1 gram dose planned at wound closure. Prophylactic intravenous cefazolin (2 grams) was administered within 60 minutes of incision.
Spinal anesthesia was utilized, providing excellent regional blockade, vasodilation (reducing intraoperative blood loss), and reduced risk of postoperative deep vein thrombosis compared to general anesthesia.
Left Total Hip Arthroplasty
The patient was placed in the right lateral decubitus position on a standard operating table, utilizing rigid pelvic positioners at the ASIS and sacrum to ensure absolute stability. The left lower extremity was prepped and draped in standard sterile fashion.

A standard posterolateral approach (Moore/Southern) was utilized. A 12 cm curvilinear incision was centered over the posterior aspect of the greater trochanter. The subcutaneous tissues were divided, and the iliotibial band and gluteus maximus fascia were incised in line with the skin incision. The gluteus maximus fibers were bluntly split, exposing the short external rotators.
The piriformis tendon, superior gemellus, obturator internus, and inferior gemellus were identified, tagged with non-absorbable suture, and tenotomized near their insertion on the greater trochanter. The capsule was exposed, and a T-shaped capsulotomy was performed. The hip was dislocated posteriorly with gentle internal rotation and flexion.
The templated femoral neck cut was executed using an oscillating saw, 15 mm proximal to the lesser trochanter, ensuring the correct angle to match the monobloc stem geometry. The femoral head was removed and passed off the field.

Attention was directed to the acetabulum. The labrum and peripheral osteophytes were excised to define the true acetabular rim. The transverse acetabular ligament was identified as a landmark for version and inferior positioning. Sequential reaming was performed, starting at 46 mm and progressing to 53 mm, achieving a bleeding subchondral bone bed with excellent concentric fit. A 54 mm uncemented, highly porous titanium hemispherical shell was impacted into position, achieving excellent rigid primary stability at 40 degrees of inclination and 20 degrees of anteversion. Two 6.5 mm titanium cancellous screws were placed in the posterosuperior quadrant for supplemental fixation. A highly cross-linked polyethylene liner (36 mm inner diameter) was seated.

The femur was then elevated and prepared. The femoral canal was opened with a box osteotome, and sequential broaching was performed. Because a monobloc stem was selected, careful attention was paid to the rotational alignment (anteversion) of the broach, aiming for 10-15 degrees of native anteversion. Broaching continued until rigid rotational and axial stability was achieved with the final broach. A trial neck and 36 mm head were placed, and the hip was reduced.
Trialing demonstrated equal leg lengths (referenced from the lesser trochanter to the center of rotation), excellent soft tissue tension, and no impingement in combined flexion/internal rotation or extension/external rotation.
The hip was redislocated. The final uncemented monobloc titanium stem was impacted into the prepared canal. A 36 mm ceramic head (+0 offset) was impacted onto the clean, dry trunnion. The hip was reduced, and final stability was confirmed.
The capsule was meticulously repaired, followed by a transosseous repair of the short external rotators and piriformis tendon to the greater trochanter to minimize dislocation risk. The fascial layer, subcutaneous tissues, and skin were closed in layers. A sterile occlusive dressing was applied.
Right Total Hip Arthroplasty
Following closure of the left hip, the surgical drapes were removed. The patient was carefully rolled into the left lateral decubitus position. The surgical team re-scrubbed, and a completely new set of sterile instruments, drapes, and gowns were utilized to prevent cross-contamination.
The right hip arthroplasty proceeded in an identical fashion to the left. The templated neck cut was performed. The acetabulum was sequentially reamed and a 54 mm uncemented porous shell was placed with two supplemental screws, followed by a highly cross-linked polyethylene liner.
The right femur was broached, and an identical uncemented monobloc stem was impacted. A 36 mm ceramic head was seated. Trialing confirmed absolute equality in leg lengths and symmetric bilateral soft tissue tension. The wound was closed in a standard layered fashion. Total operative time for both procedures was 145 minutes. Estimated blood loss was 450 mL total.
Post Operative Protocol and Rehabilitation
Immediate Postoperative Phase (Days 0 to 2)
The patient was transferred to the Post-Anesthesia Care Unit (PACU) and subsequently to the orthopedic ward.
* Weight Bearing: Weight-bearing as tolerated (WBAT) bilaterally with the assistance of a front-wheeled walker.
* Mobilization: Physical therapy was initiated on postoperative Day 0. The patient successfully stood and ambulated 15 feet within 6 hours of surgery.
* Precautions: Standard posterior hip precautions were instituted (no hip flexion past 90 degrees, no adduction across the midline, no internal rotation) for 6 weeks.
* VTE Prophylaxis: Given the bilateral nature of the procedure, DVT prophylaxis consisted of Aspirin 81mg BID for 4 weeks, combined with sequential compression devices (SCDs) while in bed.
* Pain Management: The multimodal pain regimen was continued, utilizing scheduled acetaminophen, NSAIDs, and PRN short-acting oral opioids (oxycodone) for breakthrough pain.
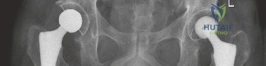
Radiographic Confirmation
Postoperative AP pelvis radiographs demonstrated bilateral uncemented THA with excellent component positioning. The acetabular shells were appropriately medialized with ideal inclination. The monobloc femoral stems were in neutral alignment, filling the metaphysis adequately without varus or valgus tilt. Leg lengths and global femoral offsets were symmetrically restored.

The lateral radiograph of the left hip confirmed appropriate anteversion of the acetabular component and central placement of the femoral stem within the medullary canal.

The lateral radiograph of the right hip similarly demonstrated excellent component alignment and seating of the uncemented monobloc stem.
Intermediate to Long-Term Rehabilitation (Weeks 2 to 12)
The patient was discharged to home on postoperative Day 2.
* Weeks 2-4: Transitioned from a front-wheeled walker to a single cane. Focus on abductor strengthening, gait normalization, and resolving the preoperative Trendelenburg habit.
* Weeks 6-8: Posterior hip precautions were lifted. The patient achieved independent, unassisted ambulation with a symmetric, non-antalgic gait.
* Months 3-6: Progressive return to low-impact recreational activities (stationary cycling, swimming, golf).
At the 6-month follow-up, the patient reported zero pain bilaterally. His Harris Hip Score improved from 42/48 preoperatively to 98 bilaterally. Radiographs showed stable components with signs of robust osseointegration and no radiolucent lines.
Clinical Pearls and Pitfalls
Pearls
- Simultaneous Bilateral Efficiency: Simultaneous bilateral THA is safe and highly effective in appropriately selected patients. Utilizing two distinct instrument trays and re-draping between sides minimizes infection risk and maintains workflow efficiency.
- Monobloc Stem Biomechanics: The use of a monobloc stem eliminates the modular junction, preventing trunnion-related complications. It is an excellent choice for patients with Dorr A or B bone where metaphyseal press-fit is reliable.
- Symmetric Restoration: Bilateral simultaneous surgery allows the surgeon to perfectly match leg lengths and offsets in a single setting, utilizing the first side as a definitive reference for the second side, avoiding the common patient complaint of perceived leg length discrepancy often seen in staged procedures.
- Blood Conservation: The routine use of intravenous Tranexamic Acid (TXA) is critical in simultaneous bilateral procedures to minimize blood loss and transfusion requirements.
Pitfalls
- Monobloc Inflexibility: The primary pitfall of the monobloc stem is the lack of modularity. If the femoral neck cut is made too low or too high, or if the stem is broached in excessive retroversion, the surgeon cannot simply change the modular neck to compensate. Meticulous preoperative templating and precise intraoperative execution of the neck cut are mandatory.
- Fat Embolism Risk: Bilateral sequential reaming and broaching of the femoral canals increase the intramedullary pressure, elevating the risk of fat emboli syndrome. Adequate venting of the femoral canal during broaching and careful monitoring by the anesthesia team during implant impaction are essential.
- Patient Selection: Failing to strictly adhere to patient selection criteria for simultaneous bilateral THA (e.g., operating on patients with severe cardiopulmonary disease or ASA > III) dramatically increases the risk of perioperative morbidity and mortality. Thorough preoperative medical optimization is non-negotiable.
