Intraarticular Malunions of the Distal Radius: Comprehensive Surgical Management
Key Takeaway
Intraarticular malunions of the distal radius with an articular step-off exceeding 2 mm significantly increase the risk of posttraumatic arthritis and functional impairment. Management requires meticulous preoperative computed tomography and timely intervention. Surgical options range from joint-preserving intraarticular osteotomies in young, active patients with simple fracture patterns, to salvage procedures like arthrodesis or carpectomy for advanced degeneration. Early correction optimizes radiocarpal biomechanics and preserves long-term wrist function.
INTRODUCTION TO INTRAARTICULAR MALUNIONS
Intraarticular malunions of the distal radius represent one of the most formidable challenges in reconstructive hand and wrist surgery. They frequently lead to profound functional disability, characterized by chronic pain, restricted range of motion, diminished grip strength, and progressive joint degeneration. The fundamental principle governing the radiocarpal joint dictates that intraarticular incongruity of 2 mm or more is directly associated with poor clinical outcomes and a high likelihood of posttraumatic arthritis (PTA).
While it is universally acknowledged that the optimal strategy is to prevent malunions through aggressive, anatomically precise initial management of intraarticular distal radial fractures, surgeons must be equipped to manage these complex deformities when primary treatment fails or is delayed. Surgical treatment of intraarticular distal radial malunions can be broadly categorized into two distinct pathways:
1. Joint-Preserving Procedures: Primarily intraarticular osteotomies aimed at restoring articular congruity and preventing posttraumatic arthritis.
2. Salvage Procedures: Interventions designed to alleviate pain once irreversible cartilage damage has occurred, including limited carpal arthrodesis, total wrist arthrodesis, proximal row carpectomy (PRC), wrist denervation, and total wrist arthroplasty.
BIOMECHANICS AND PATHOANATOMY
Understanding the biomechanical consequences of an intraarticular malunion is critical for preoperative planning. The normal radiocarpal joint transmits approximately 80% of the axial load through the distal radius and 20% through the triangular fibrocartilage complex (TFCC) and distal ulna.
When an articular step-off or gap exceeds 2 mm, the contact area of the radiocarpal joint decreases dramatically. This reduction in surface area leads to a focal concentration of contact stresses on the articular cartilage. Over time, these elevated peak pressures overwhelm the chondrocytes' ability to maintain the extracellular matrix, initiating a cascade of cartilage degradation, subchondral sclerosis, and eventual osteoarthritis. Furthermore, volar or dorsal subluxation of the carpus—often seen in malunited Barton fractures—alters the kinematic center of rotation, leading to rapid, catastrophic joint wear and severe instability.
Clinical Pearl: An articular step-off is generally less tolerated than an articular gap. A step-off creates a rigid mechanical block to carpal translation and acts as a "plow" against the opposing scaphoid or lunate cartilage during wrist motion.
INDICATIONS AND CONTRAINDICATIONS FOR INTRAARTICULAR OSTEOTOMY
Intraarticular osteotomies are technically demanding procedures that require meticulous patient selection. The primary goal is to recreate the original fracture lines, mobilize the malunited fragments, and restore a congruent articular surface.
Indications
Intraarticular osteotomies are indicated in patients who meet the following criteria:
* Patient Profile: Young, active individuals with high functional demands.
* Articular Deformity: More than 2 mm of articular step-off or gap.
* Joint Status: No clinical or radiographic evidence of established posttraumatic arthritis.
* Instability: Volar or dorsal subluxation of the radiocarpal joint secondary to loss of the volar or dorsal lip (e.g., malunited Barton fractures).
* Fracture Pattern: Simple intraarticular fracture patterns are most amenable to correction. Ideal candidates include those with malunited radial styloid fractures (Chauffeur's fractures), volar/dorsal Barton fractures, and isolated dorsal die-punch fractures.
Contraindications
Attempting an intraarticular osteotomy in the wrong patient can lead to disastrous outcomes. Absolute and relative contraindications include:
* Advanced Osteoarthritis: If the cartilage is already denuded, restoring bony anatomy will not relieve pain.
* Massive Articular Comminution: "Exploded" joints with multiple small, avascular fragments cannot be reliably reconstructed.
* Poor Bone Quality: Severe osteopenia or osteoporosis precludes rigid internal fixation.
* Patient Factors: Low functional demands, medical comorbidities precluding prolonged surgery, or non-compliance with postoperative rehabilitation.
* Soft Tissue Compromise: Poor soft tissue coverage or active infection.
* Neuropathic Pain: Reflex sympathetic dystrophy (RSD) / Complex Regional Pain Syndrome (CRPS) is a strong contraindication, as surgical trauma often exacerbates the condition.
PREOPERATIVE EVALUATION AND PLANNING
A successful intraarticular osteotomy is won or lost in the preoperative planning phase. Standard posteroanterior (PA), lateral, and oblique radiographs provide a baseline assessment of radial height, inclination, volar tilt, and ulnar variance, but they are insufficient for mapping intraarticular deformities.
Advanced Imaging
- Computed Tomography (CT): A CT scan with 1-mm fine cuts in the sagittal, coronal, and axial planes is mandatory. It precisely characterizes the malunion, identifies the location of the step-off (e.g., scaphoid fossa vs. lunate fossa), and reveals the presence of subchondral cysts or early arthritic changes.
- Three-Dimensional (3D) Reconstruction: When available, 3D CT reconstructions and 3D-printed models are invaluable. They allow the surgeon to visualize the spatial orientation of the fragments and can be used to pre-contour plates or practice the osteotomy.
Wrist Arthroscopy
If the condition of the articular cartilage is uncertain based on imaging, diagnostic wrist arthroscopy should be performed either as a staged procedure or immediately prior to the osteotomy. Arthroscopy allows direct visualization of the chondral surfaces. If widespread grade III or IV chondromalacia is identified, the surgeon should abandon the osteotomy and proceed directly to a salvage procedure.
Surgical Warning: Never commit to an intraarticular osteotomy without discussing salvage options with the patient. Consent must always include the possibility of proceeding to a limited or total wrist fusion if the joint is found to be unsalvageable intraoperatively.
SURGICAL TIMING: THE GOLDEN WINDOW
The timing of surgical intervention is a critical determinant of success. Optimally, intraarticular osteotomies are performed within 6 weeks after the initial injury. During this "early reconstruction" phase, the fracture lines are still composed of immature woven bone and fibrous tissue, making them easily identifiable and amenable to mobilization with osteotomes.
If the osteotomy is delayed too long, the malunion consolidates with dense cortical bone. More importantly, with large articular step-offs or radiocarpal subluxation, irreversible posttraumatic arthritis may develop within the first year. Once this occurs, the wrist becomes unsalvageable from a joint-preservation standpoint, and the patient is relegated to salvage procedures.
SURGICAL TECHNIQUE: INTRAARTICULAR OSTEOTOMY
1. Positioning and Setup
The patient is placed supine with the operative arm extended on a radiolucent hand table. A well-padded proximal arm tourniquet is applied. Regional anesthesia (supraclavicular or axillary block) combined with general anesthesia or deep sedation is preferred. High-quality fluoroscopy must be positioned to allow seamless PA and lateral imaging without compromising the sterile field.
2. Surgical Approaches
The approach is dictated by the location of the malunited fragment.
- Volar Approach (Modified Henry): Ideal for volar Barton malunions and accessing the volar lunate facet.
- An incision is made over the flexor carpi radialis (FCR) tendon.
- The FCR sheath is incised, and the tendon is retracted ulnarly to protect the palmar cutaneous branch of the median nerve.
- The floor of the FCR sheath is incised to access the space of Parona.
- The flexor pollicis longus (FPL) is retracted ulnarly, and the pronator quadratus is elevated from its radial border to expose the volar distal radius.
- Dorsal Approach: Ideal for dorsal die-punch fragments and dorsal Barton malunions.
- A longitudinal dorsal incision is made centered over Lister's tubercle.
- The extensor retinaculum is incised over the third dorsal compartment, and the extensor pollicis longus (EPL) is transposed radially or ulnarly.
- The second and fourth compartments are elevated subperiosteally to expose the dorsal radiocarpal joint. A dorsal capsulotomy may be required to visualize the articular surface directly.
- Radial Approach: Utilized for isolated radial styloid malunions. Care must be taken to identify and protect the superficial branch of the radial nerve (SBRN).
3. Executing the Osteotomy
- Identification: Using fluoroscopy and preoperative CT mapping, the healed fracture line is identified.
- Osteotomy: Fine, sharp osteotomes (e.g., 4 mm or 6 mm) are carefully driven into the malunion site. The osteotome must follow the original fracture plane to avoid creating new, iatrogenic intraarticular fragments.
- Mobilization: Once the osteotomy is complete, the fragment is mobilized. Soft tissue attachments (such as the radiocarpal ligaments on the radial styloid or volar lip) must be meticulously preserved to maintain the blood supply to the fragment.
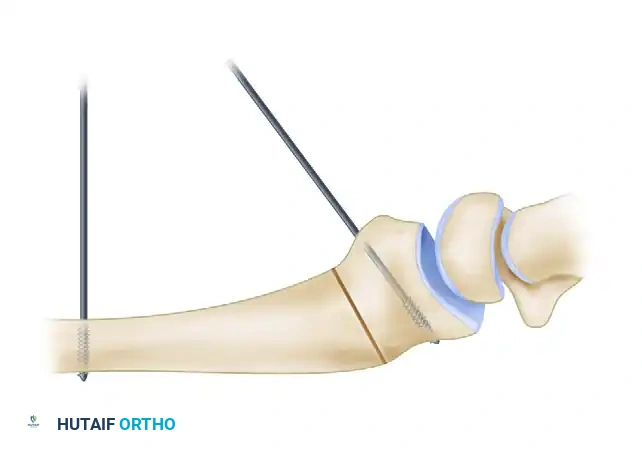
- Reduction: K-wires (1.1 mm or 1.6 mm) are inserted into the mobilized fragment to act as "joysticks." The fragment is manipulated into anatomical alignment, restoring articular congruity. Fluoroscopy and, if necessary, arthroscopy are used to confirm a step-off of less than 1 mm.
4. Bone Grafting
Mobilizing a malunited fragment invariably creates a metaphyseal void. This defect must be filled with structural bone graft to support the articular surface and prevent secondary subsidence.
* Cancellous or corticocancellous autograft from the iliac crest is the gold standard.
* Alternatively, structural allograft or synthetic bone substitutes (e.g., calcium phosphate cement) can be used, provided rigid internal fixation is achieved.
5. Internal Fixation
Rigid fixation is paramount. Depending on the fragment size and location:
* Volar Fragments: Supported with a volar locking plate. Small, distal fragments may require fragment-specific fixation using hook plates or wire forms.
* Dorsal Fragments: Stabilized with low-profile dorsal plates or buried K-wires.
* Radial Styloid: Often best fixed with headless compression screws or a radial column plate.
6. Addressing Concomitant Pathology
Intraarticular malunions frequently do not occur in isolation. Associated pathological conditions must be identified and treated concurrently:
* Extraarticular Malunion: Metaphyseal angulation or shortening must be corrected simultaneously to restore overall radial alignment.
* Distal Radioulnar Joint (DRUJ) Dysfunction: Radial shortening often leads to ulnar impaction syndrome or DRUJ incongruity. This may necessitate a concurrent ulnar shortening osteotomy or a matched distal ulna resection (Darrach or Sauvé-Kapandji procedure) if the DRUJ is arthritic.
* Scapholunate Ligament Injury: Chronic scapholunate dissociation should be addressed, potentially requiring capsulodesis or ligament reconstruction.
SALVAGE PROCEDURES
When an intraarticular osteotomy is contraindicated due to delayed presentation, advanced osteoarthritis, or massive comminution, salvage procedures are employed to provide a painless, stable wrist, albeit at the cost of motion.
- Limited Carpal Arthrodesis: Procedures such as radioscapholunate (RSL) fusion can be utilized if the midcarpal joint is preserved. This is often combined with distal scaphoid excision.
- Proximal Row Carpectomy (PRC): An option if the lunate fossa is severely damaged but the capitate head and lunate facet of the radius (or at least the radiolunate articulation) can be optimized. However, PRC is generally contraindicated if the radius articular surface is globally destroyed.
- Total Wrist Arthrodesis: The gold standard for pan-carpal arthritis or severe, unsalvageable intraarticular malunions. It provides reliable pain relief and a stable grip, though all radiocarpal and midcarpal motion is sacrificed.
- Wrist Denervation: A palliative option for low-demand patients seeking pain relief without sacrificing motion, involving the surgical transection of the anterior and posterior interosseous nerves.
- Total Wrist Arthroplasty: Reserved for low-demand, elderly patients with severe arthritis who require preservation of wrist motion for activities of daily living.
POSTOPERATIVE PROTOCOL AND REHABILITATION
Following an intraarticular osteotomy, the wrist is immobilized in a bulky plaster splint for 10 to 14 days to allow soft tissue healing and reduce edema.
- Phase 1 (0-2 weeks): Strict elevation, digital range of motion exercises to prevent tendon adhesions.
- Phase 2 (2-6 weeks): The splint is transitioned to a removable custom orthosis. Gentle, active range of motion (AROM) of the wrist and forearm is initiated. Passive stretching is strictly avoided to prevent displacement of the osteotomy.
- Phase 3 (6-12 weeks): Radiographs are obtained to confirm bony consolidation. Once bridging trabeculae are visible, passive range of motion (PROM) and progressive strengthening exercises are commenced.
- Phase 4 (>12 weeks): Return to heavy manual labor or sports is generally permitted once full radiographic union is achieved and grip strength reaches at least 80% of the contralateral side.
OUTCOMES AND EVIDENCE-BASED LITERATURE
Historically, there have been few reports in the literature concerning the results of intraarticular osteotomy for distal radial malunions, and long-term outcomes were considered uncertain. However, contemporary literature demonstrates that when performed in carefully selected patients, the results are highly encouraging.
Two- and three-year outcomes in small series report good or excellent results in the vast majority of patients.
* Ruch et al. demonstrated that early intraarticular osteotomy (performed before the onset of arthritic changes) significantly improved both grip strength and the functional range of motion of the wrist.
* Marx and Axelrod reported on a small cohort, noting excellent results in one patient and good results in three patients, with a 100% satisfaction rate regarding pain relief and functional restoration.
The most robust data comes from a multicenter study by Ring et al., who reported on 23 intraarticular distal radial malunions treated with corrective osteotomy. With an average follow-up of 38 months, the study highlighted the efficacy of the procedure. The primary indication in 14 of these patients was dorsal or volar subluxation of the radiocarpal joint, while 17 patients had at least 2 mm of articular step-off. The study concluded that anatomical restoration of the articular surface successfully halted the progression of posttraumatic arthritis and restored functional kinematics to the wrist, provided the intervention occurred before irreversible cartilage damage was established.
Clinical Pearl: The success of an intraarticular osteotomy is inversely proportional to the time elapsed since the injury. Surgeons must maintain a high index of suspicion for articular incongruity during the initial management of distal radius fractures and intervene decisively when conservative measures fail to maintain a congruent joint.
📚 Medical References
You Might Also Like