Cubital Tunnel Release: An Intraoperative Masterclass in Ulnar Nerve Decompression
Key Takeaway
Welcome, fellows, to an immersive masterclass on cubital tunnel syndrome surgical treatment. We'll meticulously cover the anatomy of the ulnar nerve at the elbow, precise preoperative planning, and the step-by-step execution of both in situ release and medial epicondylectomy. Learn critical pearls, pitfalls, and post-operative protocols to optimize patient outcomes for this common compression neuropathy.
Comprehensive Introduction and Patho-Epidemiology
Welcome, fellows, to the operating theater. Today, we are addressing a common yet critical condition: cubital tunnel syndrome. This is a compression neuropathy of the ulnar nerve, occurring at or around the elbow, a region we surgeons refer to as the cubis, derived from Latin. It stands as the second most prevalent compression neuropathy of the upper limb requiring surgical intervention, surpassed only by carpal tunnel syndrome. Our objective is to meticulously decompress the ulnar nerve, restoring its axonal transport mechanisms, alleviating the patient's debilitating symptoms, and preventing irreversible motor endplate degradation.
The pathophysiology of cubital tunnel syndrome is multifactorial, encompassing mechanical compression, dynamic traction, and localized ischemia. Unlike the median nerve at the wrist, which is primarily subject to static pressure within a confined space, the ulnar nerve at the elbow is subjected to significant excursion and tension during normal physiologic range of motion. Prolonged or repetitive elbow flexion increases intraneural pressure, leading to venous congestion, breakdown of the blood-nerve barrier, and subsequent endoneurial edema. This cascade initially manifests as reversible neuropraxia, but if left untreated, progresses to irreversible axonotmesis, Wallerian degeneration, and intraneural fibrosis.
Epidemiologically, cubital tunnel syndrome affects a broad demographic, though it frequently presents in patients whose occupations or recreational activities demand repetitive elbow flexion or valgus stress. Throwing athletes, manual laborers, and individuals who sleep with their elbows acutely flexed are at particularly high risk. Furthermore, systemic conditions such as diabetes mellitus, thyroid dysfunction, and alcoholism can lower the threshold for nerve injury, making the nerve more susceptible to the double-crush phenomenon. Understanding these underlying systemic and biomechanical factors is essential for accurate prognostication and comprehensive patient management.
Historically, the surgical management of cubital tunnel syndrome was heavily biased toward routine anterior transposition of the ulnar nerve. However, contemporary orthopedic literature and advanced neurodynamic studies have catalyzed a paradigm shift. We now recognize that a meticulously executed in situ decompression is often sufficient for primary, uncomplicated cases, minimizing the disruption of the nerve's intrinsic segmental blood supply. Transposition techniques and medial epicondylectomies are now more judiciously applied, tailored to specific anatomical aberrancies, severe traction neuropathies, or revision scenarios. Today’s masterclass will navigate these nuanced decision-making algorithms.
Detailed Surgical Anatomy and Biomechanics
Let us begin with a thorough review of the anatomy, which is paramount for a successful outcome and for avoiding devastating iatrogenic complications. The ulnar nerve is a terminal branch of the medial cord of the brachial plexus, receiving its primary contributions from the C8 and T1 nerve roots. As it descends through the medial compartment of the arm, it lies anterior to the medial intermuscular septum before piercing it—typically at the arcade of Struthers—to enter the posterior compartment.
Neurovascular Relationships and Cutaneous Nerves
It is crucial to appreciate the surrounding cutaneous structures before making the skin incision. The medial antebrachial cutaneous nerve (MABC) and the medial brachial cutaneous nerve (MBCN) both originate directly from the medial cord, not as branches of the ulnar nerve itself. However, they frequently arborize directly within our surgical field. Expect to find the branches of the MABC often deeper than anticipated, nestled along the fascia of the triceps, brachialis, and flexor carpi ulnaris (FCU). Meticulous subcutaneous dissection is required to identify and preserve these sensory nerves. Laceration or entrapment of the MABC in scar tissue is the leading cause of painful postoperative neuromas, a complication that can overshadow a perfectly executed ulnar nerve decompression.
The Cubital Tunnel and Sites of Compression
The ulnar nerve traverses the cubital tunnel, a complex fibro-osseous tunnel at the medial aspect of the elbow. Understanding its boundaries is fundamental: the medial epicondyle forms the anterior-medial wall; the olecranon forms the posterior-lateral wall; the medial collateral ligament (MCL) of the elbow—specifically the anterior and posterior bundles—forms the floor. The roof is formed by the fibrous retinaculum, classically known as the arcuate ligament of Osborne, which spans from the medial epicondyle to the olecranon.
Any of several potential sites of compression around the elbow can lead to cubital tunnel syndrome. Our surgical approach must systematically interrogate all these possibilities:
* Arcade of Struthers: Present in roughly 70% of the population, located approximately 8 cm proximal to the medial epicondyle. It consists of a fascial thickening running from the medial head of the triceps to the intermuscular septum.
* Medial Intermuscular Septum: The ulnar nerve may "scissor" over this septum as it transitions from the anterior to the posterior compartment. In cases of anterior transposition, if this septum is not adequately excised, it creates a rigid fulcrum, becoming a new, iatrogenic point of compression.
* Arcuate Ligament of Osborne: This fibrous band forming the roof of the cubital tunnel is the most frequent site of primary stenosis.
* Heads of the Flexor Carpi Ulnaris (FCU): Distally, the nerve passes between the humeral and ulnar heads of the FCU. We must release the deep aponeurotic fascia well into the muscle belly to ensure complete distal decompression.
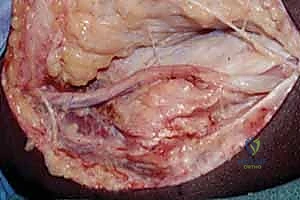
* Anomalous Anconeus Epitrochlearis Muscle: This is a rare, anomalous thin muscle extending from the medial olecranon to the medial epicondyle, effectively replacing Osborne's ligament with dynamic muscle tissue.
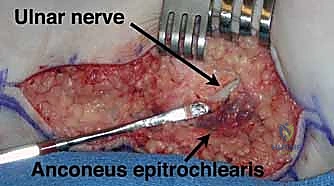
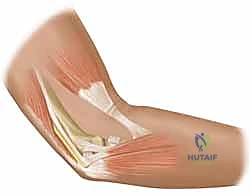
FIG 2 • An anomalous anconeus epitrochlearis encountered overlying the cubital tunnel. Anterior is at top and posterior at bottom; the forearm is to the left.
Ulnar Nerve Branches and Biomechanical Considerations
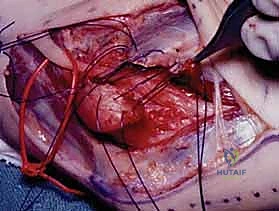
As we dissect, we must respect the critical branches of the ulnar nerve. The articular sensory branch to the elbow joint is typically the first branch encountered proximally within the tunnel. Distally, the motor branches to the flexor carpi ulnaris (FCU) and the ulnar half of the flexor digitorum profundus (FDP) emerge. The FCU branches are usually found proximally as the muscle belly appears, often tethering the nerve. Extreme caution is warranted here; aggressive mobilization without dissecting these motor fascicles free can result in catastrophic avulsion and iatrogenic motor deficit.
Biomechanically, the ulnar nerve is highly vulnerable. The nerve is superficial at the elbow, making it susceptible to both minor repetitive contusions and high-energy trauma. Furthermore, dynamic compression is significant. Elbow flexion demonstrably increases extraneural pressure by tightening Osborne's ligament and the FCU aponeurosis, while simultaneously decreasing the cross-sectional volume of the cubital tunnel by up to 55%. Additionally, an inherently shallow bony groove can predispose the nerve to subluxation or "perching" on the apex of the medial epicondyle during flexion, leading to repetitive friction microtrauma.

FIG 3 • A. “Perched” ulnar nerve. The nerve subluxates anteriorly, sitting on top of the medial epicondyle with the elbow in flexion.
Exhaustive Indications and Contraindications
The decision to proceed with surgical intervention for cubital tunnel syndrome must be evidence-based, relying on a synthesis of clinical severity, duration of symptoms, and the failure of exhaustive non-operative modalities. Non-operative management—comprising nighttime extension splinting (keeping the elbow at 30-45 degrees of flexion), activity modification, and localized elbow padding—should be trialed for a minimum of 3 to 6 months in patients with mild, purely sensory symptoms. Surgery is indicated when these conservative measures fail to halt disease progression or alleviate unacceptable symptoms.
Absolute indications for surgical decompression center around the presence of motor compromise or irreversible sensory degradation. Patients presenting with measurable weakness in the ulnar-innervated intrinsic musculature of the hand, profound atrophy, or persistent two-point discrimination deficits require prompt surgical intervention to prevent permanent disability. Advanced disease often manifests as clawing of the ring and small fingers (due to loss of intrinsic flexion at the MCP joints and unopposed extrinsic extension), a sign that dictates immediate surgical scheduling, though patients must be counseled that intrinsic recovery may be incomplete.

FIG 3 • B. Wasting of first dorsal interosseous nerve. (A: Copyright Amy Ladd, MD.)
Contraindications to isolated cubital tunnel release are critical to identify to avoid "failed" surgeries. A primary contraindication is the presence of a more proximal cervical radiculopathy (C8-T1) or a distal entrapment at Guyon's canal that fully explains the patient's symptoms. While a "double crush" scenario may exist, addressing the elbow alone in the face of severe cervical stenosis will yield suboptimal results. Additionally, patients with severe, end-stage systemic polyneuropathy (e.g., advanced diabetic neuropathy) without focal electrodiagnostic evidence of entrapment at the elbow are poor surgical candidates.
Indications and Contraindications Summary
| Category | Specific Clinical Scenarios | Rationale / Considerations |
|---|---|---|
| Absolute Indications | Progressive motor weakness (interossei, adductor pollicis) | Indicates severe axonal loss; requires urgent decompression to salvage motor endplates. |
| Intrinsic muscle atrophy / Wasting | Late-stage sign; surgery halts progression, though full reversal of atrophy is unlikely. | |
| Failure of 3-6 months of conservative care | Persistent pain/numbness impacting quality of life despite splinting and NSAIDs. | |
| Relative Indications | Recurrent symptoms in throwing athletes | May require anterior transposition due to dynamic valgus overload and MCL pathology. |
| Ulnar nerve subluxation / "Snapping" triceps | Friction neuritis necessitates stabilization (transposition or epicondylectomy). | |
| Contraindications | Asymptomatic incidental findings on EMG | Surgery should treat the patient, not the electrical study. |
| Isolated cervical radiculopathy (C8-T1) | Symptoms mimic cubital tunnel; requires cervical spine MRI and potential spine intervention. | |
| Severe systemic polyneuropathy | Diffuse nerve damage will not benefit from focal surgical release. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the cornerstone of a successful operation. Before we even consider the knife, we must meticulously review the patient's history, physical examination, and objective diagnostic data to formulate a precise surgical blueprint.
Clinical Evaluation and Physical Examination
Key subjective findings include numbness and tingling in the small and ulnar half of the ring fingers, often accompanied by burning pain radiating from the medial epicondyle down the ulnar forearm. These symptoms are characteristically exacerbated at night or during activities requiring prolonged elbow flexion, such as talking on a cellular phone. Patients with progressive disease will report insidious hand weakness, manifesting as clumsiness, difficulty opening jars, or dropping objects.
Our physical examination must be systematic and rigorous. Sensory evaluation utilizing Semmes-Weinstein monofilaments provides objective, reproducible threshold measurements. It is vital to evaluate the dorsal ulnar cutaneous nerve territory (the ulnar dorsum of the hand); normal sensation here in the presence of volar ulnar numbness strongly suggests a distal entrapment at Guyon's canal rather than the cubital tunnel. Motor examination focuses on the intrinsic muscles: look for wasting of the first dorsal interosseous and hypothenar eminence.
Specific provocative tests are indispensable. Tinel's test—percussing over the cubital tunnel—is sensitive but lacks specificity. The Elbow Flexion Test, performed by holding the elbow in maximal flexion with wrist extension for 60 seconds, is highly sensitive for reproducing paresthesias. We also utilize the Crossed Finger Test to demonstrate weakness of the dorsal and palmar interossei, Froment's Sign to indicate compensatory interphalangeal hyperflexion due to adductor pollicis weakness, and Wartenberg's Sign, an abducted posture of the small finger resulting from weak palmar interossei and an unopposed extensor digiti minimi. Finally, palpate the nerve through a full arc of motion to assess for dynamic subluxation over the medial epicondyle.
Diagnostic Studies and Imaging
Plain radiographs of the elbow are mandatory. We utilize standard AP and lateral views, but an axial view of the cubital tunnel is particularly helpful. This view allows us to evaluate the bony architecture of the groove, identifying post-traumatic deformities (cubitus valgus/varus), malunions, degenerative osteophytes, or heterotopic ossification that may be directly impinging on the nerve.
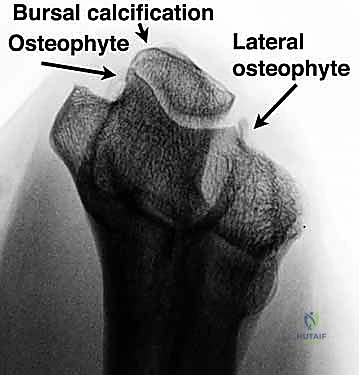
FIG 4 • Axial view of the elbow demonstrates a hooked osteophyte within the cubital tunnel, as well as calcification in the bursa and osteophyte. (Copyright Amy Ladd, MD.)
Electrodiagnostic studies (Nerve Conduction Studies and Electromyography) are the gold standard for confirming the diagnosis and localizing the exact site of compression. While they may be falsely negative in early, mild cases, they are critical for surgical planning. Diagnostic criteria include a motor conduction velocity across the elbow of less than 50 m/sec, or a focal drop in velocity of greater than 10 m/sec compared to the forearm segment. The presence of fibrillation potentials or positive sharp waves on EMG indicates active axonal denervation, portending a poorer prognosis for complete recovery and underscoring the urgency of decompression. High-resolution ultrasound and MRI are increasingly utilized as ancillary studies to define soft tissue aberrancies, nerve cross-sectional area, or intraneural neuromas.

Patient Positioning and Operating Room Setup
The patient is positioned supine on the operating table. The arm is externally rotated and abducted, supported comfortably on a radiolucent arm table. We utilize folded sterile towels to stabilize and elevate the elbow, ensuring it is slightly flexed (approximately 45 to 60 degrees) and the forearm is supinated. This specific posture opens the medial joint space and provides optimal, unhindered exposure of the medial epicondyle and the entire course of the cubital tunnel.
A standard pneumatic tourniquet is applied high in the axilla over soft padding to prevent skin maceration or secondary nerve injury. If a sterile tourniquet is preferred to allow for more proximal extension of the incision, the entire forequarter must be meticulously prepped and draped. In obese patients, a proximally placed tourniquet can be challenging to secure due to distal gapping; take the extra time to ensure a snug, effective fit, or utilize a conical tourniquet. Adequate hemostasis is absolutely critical for visualizing the delicate vasa nervorum and the microscopic branches of the MABC. The tourniquet is inflated to 250 mmHg only after thorough exsanguination of the arm with an Esmarch bandage.
Step-by-Step Surgical Approach and Fixation Technique
Our choice of surgical technique is highly individualized. Today, we will focus on the foundational techniques: the in situ release and the in situ release with medial epicondylectomy. These are the primary workhorses for the vast majority of patients. Anterior transposition is reserved for specific indications, such as a severely subluxating nerve, a biologically poor nerve bed (e.g., severe osteoarthritis with osteophytes), or revision surgery.
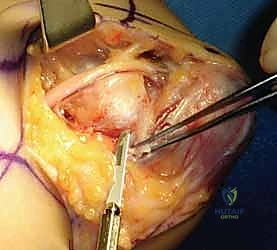
The Incision and Superficial Dissection
We begin with a curvilinear incision, approximately 8 to 10 cm in length, centered just posterior to the medial epicondyle. The incision should not be placed directly over the prominence of the epicondyle to avoid a painful, tethered scar.

We incise the skin and immediately transition to blunt dissection using tenotomy scissors. The subcutaneous fat is carefully spread to identify the branches of the medial antebrachial cutaneous nerve (MABC). These branches typically run transversely across the operative field, from anterior to posterior.

Once identified, the MABC branches are gently mobilized and protected with vessel loops. Never use monopolar electrocautery in the superficial subcutaneous tissues here; utilize bipolar cautery exclusively to maintain a dry field without risking thermal injury to these delicate sensory fascicles.
In Situ Decompression
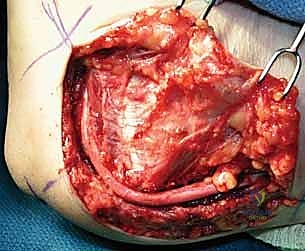
With the MABC protected, we incise the deep fascia overlying the ulnar nerve proximal to the cubital tunnel. The nerve is identified by its characteristic yellowish hue and longitudinal vascular striations. We trace the nerve distally, identifying the roof of the cubital tunnel—the arcuate ligament of Osborne.

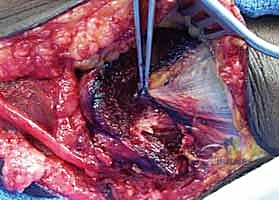
Using a combination of dissecting scissors and a scalpel, Osborne's ligament is sharply divided. The release must continue distally between the humeral and ulnar heads of the flexor carpi ulnaris (FCU). It is imperative to release the deep aponeurotic fascia of the FCU for at least 5 cm distal to the epicondyle. During this distal dissection, carefully identify and preserve the motor branches to the FCU, which exit the nerve laterally and plunge directly into the muscle belly.
Next, our attention turns proximally. The ulnar nerve is traced proximally into the arm for at least 8 to 10 cm. The medial intermuscular septum is identified. If the septum is thick or if the nerve appears to drape tightly over it, a 2 to 3 cm segment of the septum must be excised to prevent proximal tethering. We also digitally explore the medial triceps for the presence of the Arcade of Struthers; if a fascial band is palpated compressing the nerve, it is sharply released.
Medial Epicondylectomy Technique
If the nerve is found to subluxate anteriorly over the epicondyle during dynamic intraoperative testing (flexing and extending the elbow), or if there is significant bony deformity, a medial epicondylectomy may be indicated to allow the nerve to glide anteriorly without tension.

To perform the epicondylectomy, we make a longitudinal incision through the common flexor-pronator origin, directly over the apex of the medial epicondyle. Using a periosteal elevator, we reflect the flexor-pronator mass anteriorly and the capsular tissues posteriorly, exposing the bony prominence.
Using a sharp, curved osteotome or an oscillating saw, we perform an oblique osteotomy. The critical technical pearl here is to remove only the anterior-medial prominence of the epicondyle. We must meticulously preserve the sublime tubercle and the attachment of the anterior bundle of the medial collateral ligament (MCL) to prevent catastrophic iatrogenic valgus instability of the elbow. After the osteotomy, the raw cancellous bone surface is smoothed with a rasp, and bone wax is applied to minimize postoperative hematoma. The flexor-pronator fascia is then securely repaired over the raw bone using heavy absorbable sutures.
Following either an in situ release or an epicondylectomy, the tourniquet is deflated. Meticulous hemostasis is achieved using bipolar cautery. The wound is copiously irrigated. The subcutaneous tissues are closed with interrupted inverted absorbable sutures, and the skin is reapproximated with a running subcuticular closure or interrupted nylon sutures, depending on surgeon preference and skin tension.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, complications can and do occur. The "failed cubital tunnel" is a notoriously difficult clinical entity to manage, often requiring complex revision surgery with unpredictable outcomes. Therefore, primary prevention through anatomical mastery is our greatest weapon.
The most frequent and arguably most debilitating complication is injury to the medial antebrachial cutaneous nerve (MABC). Laceration, aggressive traction, or entrapment of the MABC in the surgical scar leads to the formation of a painful neuroma. Patients present with exquisite point tenderness, hyperalgesia, and a positive Tinel's sign over the incision, often overshadowing any improvement in their ulnar nerve symptoms.

Another significant complication is iatrogenic ulnar nerve instability. If an in situ release is performed too aggressively, completely detaching the nerve from its bed without addressing a pre-existing tendency to subluxate, the nerve may snap back and forth over the medial epicondyle postoperatively. This friction neuritis causes severe pain and requires revision surgery, typically an anterior submuscular transposition.
Incomplete decompression is the primary cause of persistent or recurrent symptoms. Failure to release the deep aponeurosis of the FCU distally, or failure to excise a restrictive medial intermuscular septum proximally, leaves the nerve subjected to ongoing ischemia. Hematoma formation, due to inadequate hemostasis after tourniquet deflation, can lead to extensive perineural fibrosis and scarring, effectively re-compressing the nerve.
Complications and Salvage Strategies
| Complication | Estimated Incidence | Prevention Strategy | Salvage / Management |
|---|---|---|---|
| MABC Neuroma | 5% - 10% | Bipolar cautery only; meticulous subcutaneous dissection; transverse incision variants. | Neuroma excision and proximal burying into the triceps muscle belly. |
| Incomplete Decompression | 3% - 8% | Mandatory exploration 10cm proximally (Struthers/Septum) and 5cm distally (FCU fascia). | Revision decompression; extensive neurolysis; consider transposition. |
| **Iatrogenic |
