Decompression, Posterolateral, and Interbody Fusion for High-Grade Spondylolisthesis
Comprehensive Introduction and Patho-Epidemiology
High-grade spondylolisthesis represents one of the most formidable and biomechanically complex spinal deformities encountered by the orthopedic spine surgeon. By definition, spondylolisthesis is the forward displacement or translation of one vertebral segment over the adjacent caudal segment. In the context of high-grade deformity, this anterior slippage constitutes 50% or more of the transverse width of the caudal vertebral body. Utilizing the universally recognized Meyerding classification system, this translates to a Grade III (51% to 75% slip), Grade IV (76% to 100% slip), or Grade V slip, the latter of which is strictly termed spondyloptosis, wherein the cranial vertebral body has completely fallen off the anterior sacral promontory.
The Wiltse-Newman classification system categorizes spondylolisthesis into five distinct etiologic types: dysplastic (congenital), isthmic, degenerative, traumatic, and pathologic. Ordinarily, the dysplastic and isthmic types are the primary drivers of high-grade slips, particularly in the pediatric and adolescent populations. In these younger cohorts, high-grade slips most commonly occur in the presence of a spondylolytic defect or a nonunion of the pars interarticularis (isthmic). Alternatively, they may arise from inherent congenital spinal anomalies, such as deficient, dysplastic, or maloriented lumbar and lumbosacral facets that fail to provide adequate posterior restraint against anterior shear forces.


The pathogenesis of this condition is inextricably linked to the biomechanics of the upright human posture. Spondylolisthesis is fundamentally a disorder of bipedalism; it increases the shear forces acting upon the lower segments of the spine and is virtually never observed in nonambulatory individuals. The lumbar spine is subjected to massive compressive loads and anterior shear vectors. The "bony hook"—a critical stabilizing complex consisting of the pedicle, the pars interarticularis, and the inferior articular facets—normally provides robust stability by resisting these shear forces and preventing forward sliding over the inferior endplates. When this hook is structurally compromised, either via dysplastic incompetence or isthmic fracture, the spine begins to translate anteriorly.
The natural history of high-grade spondylolisthesis underscores the necessity for vigilant clinical evaluation and, frequently, surgical intervention. Landmark long-term data, such as the 24-year follow-up study by Harris and Weinstein, demonstrated that among patients with high-grade slips treated nonoperatively or with simple in situ fusion, only 36% remained asymptomatic, while 55% suffered from chronic back pain and 45% developed progressive neurologic symptoms. Conversely, Beutler et al., in a 45-year longitudinal study of patients with spondylolysis, revealed that while unilateral pars defects rarely progress to listhesis, bilateral defects with low-grade slips tend to stabilize over time. However, high-grade dysplastic slips exhibit a marked propensity for relentless progression, driven by the structural inability of the dysplastic elements to resist the immense lumbosacral shear loads, thereby mandating definitive surgical stabilization.
Detailed Surgical Anatomy and Biomechanics
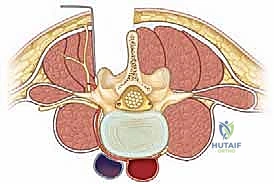
A profound understanding of the osseous and neurovascular anatomy of the lumbosacral junction is paramount for the safe execution of decompression and fusion procedures. The vertebral bodies of the lumbar spine progressively increase in size and cortical density as one moves caudally. This evolutionary adaptation is directly related to the escalating demands of stress, axial loading, and weight-bearing placed on the lumbosacral junction. The lumbar vertebrae are characteristically wider in their transverse diameter than in the anterior-posterior plane. The spinal canal and corresponding foramina assume a trefoil-like morphology, which tightly accommodates the traversing and exiting neural elements. The spinous processes are large and oblong, while the transverse processes project directly laterally, serving as critical levers for paraspinal musculature and primary decortication sites for posterolateral fusion beds.

The facet joints of the upper lumbar spine are oriented primarily in the sagittal plane, facilitating flexion and extension while restricting axial rotation. However, at the lumbosacral junction, the facet orientation abruptly transitions. The L5-S1 facet joints are flatter and more coronally oriented, a critical biomechanical design intended to resist the massive anterior shearing forces generated by the lumbar lordosis intersecting with the sacral slope. In dysplastic spondylolisthesis, these facets are often sagittally oriented, hypoplastic, or entirely absent, eradicating this essential shear-resistance mechanism. Furthermore, the pedicles—cylindrical cortical bridges connecting the anterior and posterior columns—exhibit distinct morphometric changes. From L1 to L5, the transverse diameter of the pedicles gradually increases, and their transverse angulation becomes progressively more medial, whereas their sagittal trajectory remains relatively neutral.
The neurovascular topography of the lumbosacral region demands meticulous surgical respect. The segmental vasculature, arising directly from the aorta, courses dorsally around the lateral waist of each vertebral body. Near the pedicles, these vessels bifurcate; one branch supplies the spinal canal, and the other perfuses the paraspinal musculature. These vessels run intimately between the transverse processes, making them highly susceptible to iatrogenic injury during aggressive lateral exposures or transverse process decortication. Neurologically, the spinal cord terminates at the conus medullaris (typically L1-L2), giving rise to the cauda equina. The dural sac lies medial to the pedicles, with the corresponding nerve roots exiting segmentally below the pedicle of the correspondingly numbered vertebra. The L5 nerve root is particularly vulnerable in high-grade slips; it courses extraforaminally over the sacral ala and can be severely stretched over the posterior superior margin of the S1 body as the L5 vertebra translates anteriorly and kyphoses into the pelvis.


Spinopelvic biomechanics represent the cornerstone of modern deformity correction. Pelvic incidence (PI) is a fixed, position-independent anatomic parameter defined as the angle subtended by a line perpendicular to the sacral endplate at its midpoint and a line connecting this point to the bicoxofemoral axis. The mean PI is approximately 47 degrees in children and 57 degrees in adults. An elevated PI dictates a higher sacral slope and a requisite increase in lumbar lordosis to maintain sagittal balance, thereby exponentially increasing the anterior shear forces at the lumbosacral junction. Patients with high-grade spondylolisthesis almost universally exhibit abnormally high PI. When the spine becomes unbalanced, the compensatory mechanisms fail, leading to a high slip angle (lumbosacral kyphosis). A slip angle greater than 50 degrees is highly predictive of slip progression, gross instability, and an unacceptable rate of pseudarthrosis if fused in situ without deformity correction.
Exhaustive Indications and Contraindications
The clinical presentation of high-grade spondylolisthesis is highly variable but often profoundly debilitating. In symptomatic patients, the most ubiquitous clinical manifestation is mechanical low back pain, frequently accompanied by radicular pain radiating through the L5 or S1 dermatomes. The onset of pain is typically chronic and insidious, heavily exacerbated by activity and upright posture, though acute episodic exacerbations are common. In patients with radicular symptoms, unilateral involvement is more frequently observed than bilateral, often due to asymmetric foraminal stenosis or unilateral tension on the L5 nerve root.
Physical examination reveals classic hallmark signs of lumbosacral deformity. A flattening of the normal lumbar lordosis is commonly seen, alongside a palpable "step-off" at the lumbosacral junction. As the slip progresses and lumbosacral kyphosis worsens, patients develop a compensatory abnormal gait, classically described as the Phalen-Dickson gait. This is characterized by a hip-flexed, knee-flexed posture with a vertical pelvis and a shortened stride, an involuntary mechanism to maintain global sagittal balance over the femoral heads. Severe hamstring tightness is nearly ubiquitous in high-grade slips, quantified clinically by measuring the popliteal angle. This tightness is not a primary muscle contracture but rather a physiologic reflex to stabilize the pelvis and counteract the anterior translation of the center of gravity.

Surgical intervention is definitively indicated for all high-grade slips (Meyerding III, IV, and V), even in the absence of overt neurologic deficits, due to the unacceptably high risk of relentless progression and the catastrophic potential for cauda equina syndrome. Refractory axial back pain, progressive radiculopathy, worsening sagittal imbalance, and deteriorating gait mechanics serve as absolute indications for operative stabilization. Straight leg raise (SLR) testing must be carefully interpreted; radicular pain elicited before 70 degrees strongly suggests acute L5 or S1 nerve root compression, whereas pain beyond 70 degrees or isolated to the posterior thigh is indicative of the aforementioned hamstring spasticity. A thorough rectal examination is mandatory to rule out insidious bowel or bladder dysfunction, which would escalate the surgical urgency.
Contraindications to surgical intervention are relatively few but must be strictly respected to avoid catastrophic perioperative morbidity. Active systemic infection, uncorrectable coagulopathy, and severe medical comorbidities precluding general anesthesia are absolute contraindications. Severe osteoporosis, while not an absolute contraindication, presents a massive challenge for instrumentation purchase and may necessitate the use of cement-augmented fenestrated screws, multiple points of fixation extending into the ilium, or an initial period of anabolic bone-building medical therapy prior to elective reconstruction.
| Clinical Parameter | Indications for Surgery | Contraindications for Surgery |
|---|---|---|
| Neurologic Status | Progressive motor deficit, Cauda Equina Syndrome, intractable radiculopathy. | Asymptomatic low-grade slip (relative), active central nervous system infection. |
| Biomechanical Stability | Meyerding Grade III, IV, V; Slip angle > 50 degrees; documented radiographic progression. | Severe, untreated osteoporosis precluding hardware purchase (relative). |
| Clinical Symptoms | Refractory mechanical back pain, Phalen-Dickson gait, severe hamstring spasticity. | Medical comorbidities precluding general anesthesia (ASA IV/V). |
| Deformity/Alignment | High pelvic incidence with unbalanced sagittal profile requiring reduction. | Active surgical site infection or untreated systemic bacteremia. |
Pre-Operative Planning, Templating, and Patient Positioning
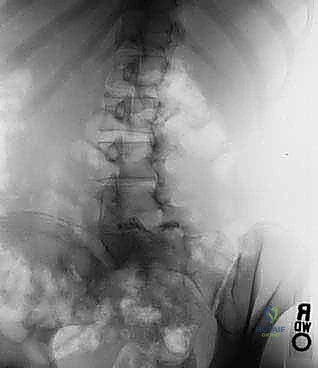
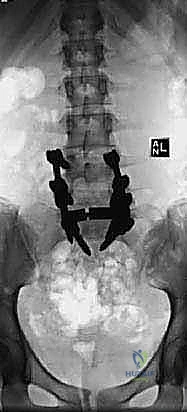
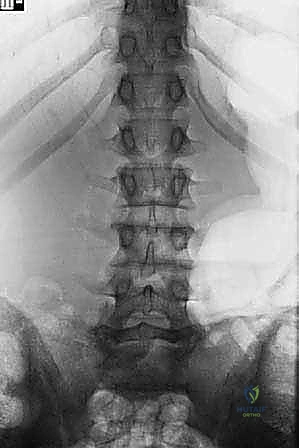
The foundation of a successful surgical outcome in high-grade spondylolisthesis is forged during the meticulous preoperative planning phase. Initial imaging must include standing, long-cassette posteroanterior (PA) and lateral radiographs of the entire spine, encompassing the cervical spine down to the femoral heads. This allows for the precise calculation of global sagittal alignment and critical spinopelvic parameters, including Pelvic Incidence (PI), Pelvic Tilt (PT), Sacral Slope (SS), and Lumbar Lordosis (LL). Oblique radiographs are historically useful for visualizing the pars interarticularis, though modern cross-sectional imaging has largely superseded their utility. The surgeon must scrutinize the radiographs for concomitant structural anomalies, such as spina bifida occulta, transitional lumbosacral anatomy, or compensatory coronal plane scoliosis.


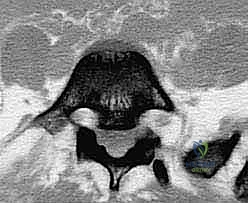
Advanced cross-sectional imaging is non-negotiable. High-resolution computed tomography (CT) scans with multi-planar sagittal and coronal reconstructions are invaluable for defining the exact bony morphology. The CT scan accurately delineates the size and trajectory of the dysplastic pedicles, the presence of the "sacral dome" (remodeling of the S1 superior endplate), and the available bone stock for interbody and trans-sacral fixation. Magnetic Resonance Imaging (MRI) is strictly indicated to evaluate the neural elements. It provides exquisite visualization of the L5 nerve roots as they exit the foramina and drape over the sacral ala, as well as the degree of central canal stenosis and cauda equina compression at the level of the pseudodisc.


Patient positioning in the operating theater requires obsessive attention to detail, as the procedure is lengthy and the risk of positioning-related neuropraxia or pressure necrosis is significant. The patient is typically positioned prone on a specialized radiolucent operative frame, such as a Jackson table. Two primary variations are utilized based on the surgical goals. The knee-chest position, where both hips and knees are heavily flexed, can help open the posterior elements for decompression but may exacerbate lumbosacral kyphosis. Alternatively, positioning the patient on a four-poster frame with the lower extremities extended parallel to the trunk helps maximize lumbar lordosis and can assist in the indirect reduction of the slip.

During positioning, the face must be meticulously supported using a specialized foam prone-view mask, ensuring absolutely no pressure is applied to the orbits to prevent catastrophic ischemic optic neuropathy. The cervical spine is maintained in a neutral alignment. The upper extremities are positioned in a strict 90-90 configuration (90 degrees of shoulder abduction and 90 degrees of elbow flexion) and generously padded to protect the ulnar nerve at the cubital tunnel and the brachial plexus from traction injuries. Continuous intraoperative neuromonitoring (SSEP, MEP, and spontaneous EMG) is established prior to positioning and monitored continuously throughout the case, particularly during the reduction maneuvers of the L5 vertebra, to provide real-time feedback on the functional integrity of the L5 and S1 nerve roots.
Step-by-Step Surgical Approach and Fixation Technique
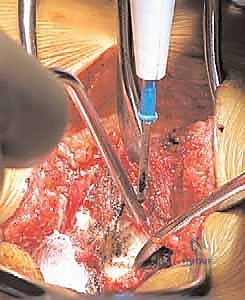
The surgical management of high-grade spondylolisthesis is governed by the paramount principle: "first, do no harm." The primary objectives are decompression of the neural elements, stabilization of the unstable segment, and restoration of a biomechanically favorable spinopelvic alignment. The procedure commences with a standard posterior midline longitudinal incision, typically extending from the spinous process of L3 down to the mid-sacrum (S2 or S3). The paraspinal musculature is elevated subperiosteally off the spinous processes, laminae, and facet joints, extending laterally to expose the tips of the transverse processes of L4 and L5, and the sacral ala. Meticulous hemostasis is maintained using bipolar electrocautery and hemostatic agents, as the epidural venous plexus in these patients is often massively engorged due to chronic structural distortion.

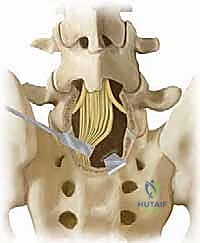

Following exposure, a wide, meticulous neural decompression is performed. In the presence of an intact but dysplastic neural arch, or a loose Gill body (the unattached posterior elements of L5 in isthmic slips), a complete laminectomy of L5 is executed. The fibrocartilaginous tissue at the pars defect is radically excised. The L5 nerve roots must be identified and decompressed from their origin at the thecal sac out into the far lateral extraforaminal zone. In high-grade slips, the L5 root is frequently tethered by a dense band of corporotransverse ligament and stretched taut over the prominent posterior-superior corner of the S1 vertebral body. Complete mobilization of these roots is an absolute prerequisite before any reduction maneuver is attempted, to mitigate the high risk of iatrogenic stretch neuropraxia.

Instrumentation typically involves the placement of robust pedicle screws into L4, L5, and S1, often supplemented with iliac or S2-alar-iliac (S2AI) screws to provide a massive distal biomechanical anchor. The decision to reduce the high-grade slip versus fusing in situ remains one of the most hotly debated topics in spine surgery. Proponents of reduction argue that restoring the slip angle and translating the L5 body posteriorly normalizes the spinopelvic parameters (specifically correcting the lumbosacral kyphosis), thereby decreasing shear forces on the hardware and improving global sagittal balance. Reduction is achieved using specialized reduction towers attached to the L5 screws, slowly cantilevering the L5 body posteriorly while distracting against the sacrum. This maneuver must be performed under continuous neuromonitoring, as the L5 root is at extreme risk of traction injury during posterior translation.


To achieve circumferential arthrodesis and long-term stability, an interbody fusion is virtually mandatory in high-grade slips. A classic and highly effective technique for severe slips (Grade IV and V) is the Bohlman technique, which utilizes a trans-sacral fibular dowel graft. This procedure is performed strictly under biplanar fluoroscopic guidance. Following posterior decompression, a guide pin is advanced from the posterior aspect of the S1 body, traversing the S1-L5 disc space, and terminating in the anterior superior quadrant of the L5 vertebral body. A cannulated drill bit (typically 1/2-inch) is used to over-drill the guide pin to a depth of approximately 5 cm, creating a trans-vertebral tunnel. A structural mid-diaphyseal fibular allograft or autograft is then impacted into this tunnel, effectively pegging the L5 body to the sacrum and providing massive resistance to anterior shear. Modern iterations of this concept utilize titanium or PEEK trans-sacral cages. Alternatively, a formal Transforaminal Lumbar Interbody Fusion (TLIF) or Anterior Lumbar Interbody Fusion (ALIF) can be performed to release the anterior longitudinal ligament, facilitate reduction, and provide a massive surface area for interbody arthrodesis.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique and advanced intraoperative technology, the surgical treatment of high-grade spondylolisthesis carries a formidable complication profile. The most feared and widely reported complication is iatrogenic neurologic deficit, specifically an L5 nerve root palsy. The incidence of L5 neuropraxia following reduction of a high-grade slip can range from 10% to over 30% in some series. This injury is rarely due to direct surgical transection; rather, it is a traction injury. As the L5 vertebral body is pulled posteriorly and cranially during reduction, the L5 nerve root, which is already stretched over the sacral ala, is subjected to acute tension. If neuromonitoring alerts (a significant drop in MEPs or sustained EMG firing) occur during reduction, the surgeon must immediately halt the maneuver, partially release the reduction, and re-evaluate the foraminal decompression.


Pseudarthrosis, or nonunion, is another major complication, historically occurring in up to 20-30% of cases treated with uninstrumented in situ fusion. The massive shear forces at the lumbosacral junction create a hostile biomechanical environment for bone healing. The use of rigid pedicle screw instrumentation combined with interbody structural support (TLIF, ALIF, or Bohlman trans-sacral dowel) has drastically reduced the pseudarthrosis rate to less than 5-10%. However, if a nonunion occurs, it inevitably leads to hardware failure, including pedicle screw fracture or rod breakage. Salvage management of a symptomatic pseudarthrosis requires revision surgery, removal of broken hardware, extension of the fusion construct (often into the pelvis), and aggressive re-grafting using rhBMP-2 (recombinant human bone morphogenetic protein-2) and copious autograft.


Surgical site infection (SSI) and wound dehiscence are significant risks, particularly given the extensive subperiosteal dissection, prolonged operative times, and the relatively poor soft tissue envelope over the lumbosacral junction in kyphotic patients. Deep infections require aggressive and often multiple surgical debridements, continuous negative pressure wound therapy (VAC), and prolonged culture-directed intravenous antibiotics. Hardware is generally retained unless it is grossly loose or the infection is caused by a highly virulent, biofilm-producing organism that is refractory to suppressive therapy. Dural tears, while less common than in revision degenerative surgery, can occur during the excision of the dense fibrocartilaginous pseudocapsule at the pars defect. These must be primarily repaired with non-absorbable suture and sealed with a dural substitute and fibrin glue to prevent postoperative cerebrospinal fluid (CSF) fistulas.
| Complication | Estimated Incidence | Prevention and Salvage Management |
|---|---|---|
| L5 Neuropraxia | 10% - 30% (with reduction |
Clinical & Radiographic Imaging Archive