Corrective Osteotomy for Forearm Diaphyseal Malunions: An Intraoperative Masterclass

Key Takeaway
This masterclass details corrective osteotomy for forearm malunions, crucial for restoring function. We cover comprehensive anatomy, meticulous preoperative planning, and granular, step-by-step intraoperative execution of volar, dorsal, and ulnar approaches. Fellows will learn precise instrument use, critical neurovascular protection, and strategies for optimal reduction and plating, ensuring restoration of the radial bow and forearm kinematics.
Comprehensive Introduction and Patho-Epidemiology
Welcome, colleagues and fellows, to the operating theater and this advanced masterclass. Today, we are undertaking a rigorous examination of a highly complex, yet profoundly rewarding orthopedic procedure: the corrective osteotomy for diaphyseal malunions of the radius and ulna. This surgical intervention transcends the mere realignment of osseous structures; it is fundamentally an exercise in the meticulous restoration of the intricate biomechanics of the forearm. The forearm must be conceptualized as a critical, dynamic "ring" structure, one that is absolutely essential for the spatial positioning of the hand and the execution of daily functional activities. A malunion, defined as a fracture that has consolidated in a biomechanically suboptimal position, initiates a devastating cascade of kinematic derangements that ultimately compromise the entire upper extremity kinetic chain.
The clinical impact of a radial or ulnar shaft malunion is profound and multifaceted. Patients typically present with a constellation of symptoms including debilitating, mechanically-induced pain, a significant and restrictive loss of range of motion, diminished grip strength, and progressive instability at both the radiocarpal and elbow articulations. Radiographically, we frequently observe a combination of malrotation, angular deformity that pathologically narrows the vital interosseous space, axial shortening, and a critical loss of the normal radial bow. These geometric alterations have been unequivocally proven to severely compromise functional outcomes. While the proximal radioulnar joint (PRUJ) can develop secondary osteoarthritis in longstanding, neglected cases, it is the distal radioulnar joint (DRUJ) that is most frequently and acutely compromised by these diaphyseal deformities, leading to subluxation, ulnocarpal impaction, and chronic pain.
The pathogenesis of both-bone forearm fractures typically involves high-energy indirect trauma, such as a fall on an outstretched hand generating complex axial and torsional loads, or direct, blunt-force blows. To understand the functional deficits, one must remember that the radius dynamically pronates and supinates around a relatively static ulna. Any alteration in the natural curvature, longitudinal length, or rotational alignment of the radius profoundly impacts this complex motion arc. For instance, a torsional deformity exceeding 30 degrees in the radius invariably leads to a mathematically predictable and clinically significant loss of forearm rotation. Furthermore, even subtle changes in the length-tension relationship of the interosseous membrane, induced by osseous shortening or angulation, can significantly restrict rotational excursion. Clinically, it is universally accepted that patients require a minimum functional arc of 50 degrees of supination and 50 degrees of pronation to perform essential activities of daily living. Malunions exhibiting greater than 15 degrees of angular malalignment, or a significant loss of the apex of the radial bow, will invariably lead to a clinically unacceptable loss of motion and strength if left unaddressed by surgical intervention.
Detailed Surgical Anatomy and Biomechanics
A profound, three-dimensional understanding of forearm anatomy is the absolute prerequisite for successful corrective osteotomy. The forearm is a marvel of biomechanical engineering, relying on the precise interplay of osseous geometry, ligamentous restraints, and muscular dynamic forces. Conceptually, the forearm functions as a closed kinematic ring, interconnected at three crucial anatomical junctures: the PRUJ, the DRUJ, and the interosseous membrane (IOM). Force transmission across the forearm predominantly occurs through the central band of the IOM, which effectively transfers axial loads from the radius distally to the ulna proximally. Disruption or slackening of this membrane due to malunion severely alters load mechanics, predisposing the wrist and elbow to premature degenerative changes.
The Radioulnar Articulations and the Interosseous Membrane
The PRUJ comprises the radial head, the radial notch of the proximal ulna, the annular ligament, and the quadrate ligament. Its stability is the cornerstone of proximal forearm rotation and longitudinal stability. Conversely, the DRUJ is a highly complex, diarthrodial articulation consisting of the sigmoid notch of the distal radius, the ulnar head, the robust dorsal and volar radioulnar ligaments, the extensor carpi ulnaris (ECU) subsheath, and the triangular fibrocartilage complex (TFCC). The DRUJ is exquisitely sensitive to alterations in radial length and alignment; even a few millimeters of radial shortening can significantly increase load transmission across the ulnocarpal joint and lead to DRUJ subluxation. The IOM, particularly its central band, is oriented obliquely from the proximal radius to the distal ulna. Restoring the tension of the IOM is a secondary, yet critical, benefit of restoring precise osseous length and alignment during corrective osteotomy.
Osteology and Neurovascular Relations of the Radius
The radial shaft is fundamentally triangular in cross-section in its proximal and middle thirds, with its sharpest apex oriented medially to serve as the attachment site for the IOM. It presents three distinct surfaces: anterior, lateral, and posterior. Critically, the radius possesses a gentle, volar-concave and ulnar-concave bow. This radial bow is not merely an aesthetic or incidental feature; its exact magnitude and location are the fundamental drivers of forearm kinematics. Schemitsch and Richards devised a critical formula demonstrating that the maximum radial bow typically occurs at approximately 60% of the length of the radius from the bicipital tuberosity, with an average magnitude of 15 millimeters.
Navigating the neurovascular relations of the radius requires meticulous surgical technique. The Superficial Radial Nerve (SRN) lies on the undersurface of the brachioradialis (BR) muscle and is at high risk during distal volar approaches (Henry approach), particularly during aggressive radial retraction. The Posterior Interosseous Nerve (PIN), a critical motor branch of the radial nerve, dictates the safety of dorsal approaches to the proximal radius (Thompson approach). It pierces the supinator muscle at the arcade of Frohse, supplying its motor branches within the muscle belly before exiting distally. Identifying, mobilizing, and protecting this nerve is non-negotiable during proximal dissection. Furthermore, the radial artery, located volar to the radius in the interval between the flexor carpi radialis (FCR) and the BR, must be carefully protected; its recurrent branches often require meticulous ligation to mobilize the proximal radius safely.
Osteology and Neurovascular Relations of the Ulna
The ulna is a structurally essential long bone, serving as the fixed axis around which the radius rotates. It is triangular in cross-section in its proximal two-thirds, transitioning to a more cylindrical and circular shape distally. It features anterior, posterior, and medial surfaces. The proximal half of the ulnar shaft exhibits a slight volar concavity, whereas the distal half is relatively straight. Its prominent subcutaneous border along the posterior aspect makes it readily palpable and provides a safe, straightforward landmark for surgical access via an internervous plane.

While the ulnar shaft itself has fewer immediate neurovascular structures directly applied to its periosteum compared to the radius, regional anatomy remains critical. The ulnar nerve lies medially in the proximal forearm and must be respected, especially when extending approaches proximally toward the olecranon or distally toward the wrist. The ulnar artery lies deep to the flexor carpi ulnaris (FCU) muscle belly and is generally well-protected during standard direct posterior or posteromedial approaches to the ulnar diaphysis. However, aberrant vascular anatomy or severe post-traumatic scarring can alter these relationships, demanding constant intraoperative vigilance.
Exhaustive Indications and Contraindications
The decision to proceed with a corrective osteotomy of the forearm is highly nuanced and must be tailored to the individual patient's functional demands, symptomatology, and the precise geometric nature of the deformity. We do not operate simply to normalize radiographs; we operate to restore function and alleviate debilitating symptoms. A meticulous assessment of the indications and absolute contraindications is the first step in ensuring a successful outcome and avoiding catastrophic complications in an already compromised extremity.
The primary indication for corrective osteotomy is a clinically significant loss of forearm rotation that directly impairs the patient's ability to perform activities of daily living or occupational tasks. Generally, a rotational arc of less than 100 degrees (combined pronation and supination) is considered functionally restrictive and warrants surgical consideration. Furthermore, DRUJ instability or incongruity resulting directly from the diaphyseal malunion—often manifesting as ulnar-sided wrist pain, a positive piano key sign, or ECU tendon subluxation—is a strong indication for diaphyseal correction before considering joint-sacrificing salvage procedures. Painful nonunions that coexist with malalignment also necessitate a combined approach of osteotomy, rigid fixation, and biological augmentation.
Conversely, absolute contraindications must be strictly observed. Active infection at the site of the previous fracture or proposed surgical incision precludes any elective osteotomy until the infection is definitively eradicated. Severe osteopenia or osteoporosis that would prevent adequate screw purchase and rigid plate fixation is a relative to absolute contraindication, as failure of osteosynthesis is highly probable. Furthermore, patients with advanced, irreversible osteoarthritis of the DRUJ or PRUJ may not benefit from an isolated diaphyseal corrective osteotomy; in these scenarios, the surgeon must consider concomitant or alternative salvage procedures, such as a Darrach procedure, a Sauvé-Kapandji procedure, or total joint arthroplasty, depending on the patient's age and functional demands.
| Category | Specific Factors | Clinical Rationale |
|---|---|---|
| Absolute Indications | Functional rotational arc < 100° | Severe impairment of ADLs and occupational capacity. |
| Symptomatic DRUJ instability | Prevents progressive ulnocarpal impaction and secondary osteoarthritis. | |
| Painful combined malunion/nonunion | Requires mechanical realignment and biological stimulation for union. | |
| Relative Indications | Unacceptable cosmesis | Patient-specific; usually combined with mild functional deficits. |
| Impending PRUJ arthrosis | Prophylactic realignment to normalize joint contact forces. | |
| Absolute Contraindications | Active local or systemic infection | High risk of hardware seeding and catastrophic osteomyelitis. |
| Severe, untreated osteoporosis | Inability to achieve rigid internal fixation; high risk of hardware pullout. | |
| Lack of viable soft tissue coverage | High risk of wound breakdown, hardware exposure, and subsequent infection. | |
| Relative Contraindications | Advanced, irreversible DRUJ/PRUJ arthritis | Diaphyseal correction alone will not relieve joint-specific arthritic pain. |
| Non-compliant patient | Post-operative rehabilitation is crucial; poor compliance risks failure. |
Pre-Operative Planning, Templating, and Patient Positioning
Fellows, I cannot overstate this: the operation is won or lost in the preoperative planning phase. Meticulous, obsessive preoperative templating is absolutely non-negotiable for a corrective osteotomy. We are not merely reducing a fresh fracture; we are deliberately creating a new fracture to correct a complex, three-dimensional deformity. This requires a comprehensive radiographic analysis, utilizing high-quality orthogonal views of both the affected and the normal, contralateral forearm. The contralateral films serve as the patient's own perfect anatomical template, allowing us to accurately determine the normal length, radial bow magnitude, and apex location.

Modern preoperative planning relies heavily on advanced imaging. While plain radiographs are foundational, a continuous thin-slice CT scan of both forearms is now considered the standard of care. The CT scan is indispensable for accurately assessing and quantifying rotational deformities, which are notoriously difficult to judge on plain films. Furthermore, the CT data can be utilized to generate three-dimensional reconstructions. In highly complex, multiplanar deformities, we increasingly utilize this 3D data to perform virtual surgical planning (VSP) and to print patient-specific, customized cutting guides. These guides allow for precise execution of the planned osteotomy angles and locations intraoperatively, significantly reducing surgical time and improving the accuracy of the correction.

When utilizing traditional AO templating techniques, the process is methodical. First, the malunion is meticulously sketched from the preoperative radiographs, noting all angular and rotational deviations. Second, the individual bone fragments proximal and distal to the deformity are isolated conceptually. Third, the precise osteotomy sites are marked on both the AP and lateral templates. The surgeon must decide on the geometry of the cut: a simple transverse cut for pure rotational correction, an oblique cut to allow for lengthening and rotation, or an opening/closing wedge osteotomy for severe angular corrections. Finally, the bone is conceptually realigned on the template. If significant shortening is present, the resulting gap on the template dictates the exact dimensions of the required structural corticocancellous bone graft, typically harvested from the iliac crest.

Patient positioning must be optimized for both surgical access and intraoperative fluoroscopy. The patient is placed supine on the operating table with the affected extremity extended onto a radiolucent hand table. A sterile tourniquet is applied high on the brachium. It is critical to ensure that the C-arm can easily swing in to obtain true AP and lateral views of the entire forearm, wrist, and elbow without obstruction. The contralateral iliac crest is prepped and draped simultaneously if a structural bone graft is anticipated. Proper positioning not only facilitates the surgical approach but also ensures that the surgeon can accurately assess the restoration of alignment and rotation dynamically throughout the procedure.
Step-by-Step Surgical Approach and Fixation Technique
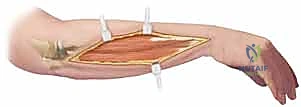
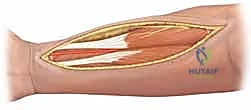
The surgical execution of a corrective osteotomy demands precision, respect for soft tissues, and rigid adherence to the principles of stable internal fixation. The choice of surgical approach is dictated by the location of the deformity and the planned osteotomy. For the radius, the volar Henry approach provides excellent exposure to the middle and distal thirds, while the dorsal Thompson approach is preferred for the proximal third to safely manage the PIN. The ulna is almost universally approached via a direct incision over its subcutaneous border, utilizing the internervous plane between the extensor carpi ulnaris and the flexor carpi ulnaris.

A fundamental principle in dual-bone malunions is the "More Deformed Bone First" rule. We typically address the bone with the most severe angular or rotational deformity initially. If both bones are equally deformed, it is highly advantageous to osteotomize, anatomically reduce, and provisionally plate the ulna first. The ulna, being relatively straight, is easier to align and provides a stable, rigid "working length" and a fixed axis around which the more complex, bowed radius can subsequently be corrected.
Once the bone is exposed, the osteotomy is executed exactly as templated. If custom 3D-printed cutting guides are used, they are securely pinned to the bone, and the cuts are made with an oscillating saw under copious saline irrigation to prevent thermal necrosis. If performing a freehand osteotomy based on 2D templating, K-wires can be placed proximal and distal to the planned cut to serve as rotational and angular references. Following the osteotomy, the bone ends are mobilized. This often requires careful subperiosteal release of contracted soft tissues and the interosseous membrane to allow for full correction of shortening and rotation.

Rigid internal fixation is paramount. We utilize 3.5mm dynamic compression plates (DCP) or locking compression plates (LCP), ensuring a minimum of six cortices of purchase both proximal and distal to the osteotomy site. The plate is typically applied to the tension band surface of the bone (dorsal for the radius, posterior for the ulna).

If an opening wedge osteotomy or an intercalary lengthening is performed, the resulting defect must be meticulously filled with a structural corticocancellous autograft from the iliac crest. The graft provides both mechanical support and osteoinductive/osteoconductive properties to ensure rapid consolidation.
Before final tightening of the screws, the forearm must be taken through a full, dynamic range of pronation and supination to confirm that the functional arc has been restored and that there is no impingement between the radius and ulna.

Intraoperative assessment of the DRUJ and PRUJ is the final critical step. After diaphyseal stabilization, the stability of the DRUJ must be tested via the piano key test and direct translation.

If the DRUJ remains unstable despite perfect diaphyseal realignment, concurrent soft tissue reconstruction (e.g., TFCC repair or Adams-Berger reconstruction) or temporary transarticular K-wire pinning in the position of maximum stability (usually supination) may be required.

Meticulous hemostasis is achieved, and the wounds are closed in layers over a suction drain to prevent hematoma formation, which can predispose to infection or ischemic contracture.

Complications, Incidence Rates, and Salvage Management
Despite meticulous planning and flawless execution, corrective osteotomy of the forearm remains a procedure fraught with potential complications. The surgeon must be acutely aware of these risks, actively work to mitigate them intraoperatively, and possess the knowledge to manage them effectively should they arise. Thorough preoperative patient counseling regarding these potential adverse events is an essential component of the informed consent process.
Neurovascular injury is a devastating complication. The Superficial Radial Nerve and the Posterior Interosseous Nerve are at the highest risk during radial exposures. The incidence of transient neurapraxia can be up to 5-10%, usually resolving with observation. However, complete transection requires immediate microsurgical repair. Vascular injury, particularly to the radial artery, is less common (<2%) but can compromise the viability of the hand if collateral circulation is insufficient. Infection rates following elective osteotomy are generally low (1-3%) but can be catastrophic, often necessitating hardware removal, aggressive debridement, and prolonged intravenous antibiotic therapy, which severely compromises the ultimate functional outcome.
Nonunion or delayed union at the osteotomy site occurs in approximately 2-10% of cases. This risk is significantly elevated in patients who smoke, those with poor nutritional status, or instances where structural bone grafting was inadequate, or fixation was insufficiently rigid. Management of a symptomatic nonunion typically requires re-operation, exchange of hardware to a more robust construct, decortication, and application of fresh autologous bone graft or orthobiologics. Radioulnar synostosis—the formation of a pathological bony bridge between the radius and ulna—is a devastating complication (incidence <5%) that completely obliterates forearm rotation. Its management is highly complex, usually requiring delayed excision of the synostosis (at least 6 months post-operatively when the bone has matured), interposition of inert material (e.g., silastic or fat), and prophylactic radiation or indomethacin therapy to prevent recurrence.
| Complication | Estimated Incidence | Prevention Strategy | Salvage / Management Strategy |
|---|---|---|---|
| Transient Neurapraxia (PIN/SRN) | 5 - 10% | Meticulous dissection; avoid aggressive retraction; identify and protect nerves. | Observation; gabapentinoids; physical therapy. Usually resolves in 3-6 months. |
| Nonunion / Delayed Union | 2 - 10% | Rigid 3.5mm plate fixation; generous use of iliac crest autograft for gaps; smoking cessation. | Revision open reduction internal fixation (ORIF); hardware exchange; repeat bone grafting; bone stimulator. |
| Radioulnar Synostosis | < 5% | Avoid operating through a single incision for both bones; meticulously control bone dust; achieve hemostasis. | Delayed excision (>6 months); soft tissue interposition (fat/muscle); post-op radiation or NSAIDs. |
| Persistent DRUJ Instability | 5 - 15% | Ensure perfect restoration of radial length and bow; intraoperative DRUJ stress testing. | TFCC repair; Adams-Berger reconstruction; or salvage (Darrach/Sauvé-Kapandji) if arthritic. |
| Deep Surgical Site Infection | 1 - 3% | Strict sterile technique; prophylactic antibiotics; meticulous soft tissue handling; drain usage. | Aggressive I&D; hardware retention if stable, removal if loose; targeted IV antibiotics. |

Phased Post-Operative Rehabilitation Protocols
The surgical procedure itself is merely the first half of the patient's journey; a rigorous, phased, and highly supervised post-operative rehabilitation protocol is equally critical to achieving an optimal functional outcome. The rehabilitation plan must be carefully communicated to both the patient and the occupational therapist, as premature stress can lead to hardware failure or nonunion, while over-protection will result in irreversible stiffness and contracture.
Phase I: Immediate Post-Operative Phase (0-2 Weeks)
The primary goals during this initial phase are the protection of the osteosynthesis, strict edema control, and pain management. The patient is typically placed in a bulky, well-padded long-arm posterior splint or a Muenster-style splint with the forearm in neutral rotation to minimize stress on the DRUJ and the osteotomy sites. Elevation of the extremity above the level of the heart is mandatory to control swelling. Active range of motion (AROM) of the digits and the shoulder is initiated immediately on post-operative day one to prevent tendon adhesions and shoulder stiffness.

Phase II: Early Mobilization Phase (2-6 Weeks)
At the two-week mark, sutures are removed, and the surgical incisions are inspected. If clinical and radiographic signs indicate stable fixation, the patient is transitioned to a custom-molded, removable thermoplastic splint. The critical transition here is the initiation of supervised, gentle Active Range of Motion (AROM) and Active-Assisted Range of Motion (AAROM) of the elbow, wrist, and forearm. Pronation and supination are introduced gradually, often starting within a pain-free arc. Passive stretching and forceful manipulation are strictly contraindicated during this phase to protect the healing osteotomy and the delicate soft tissue reconstructions at the DRUJ.
Phase III: Strengthening and Functional Restoration (6-12 Weeks)
By six weeks, early radiographic evidence of bridging callus at the osteotomy site should be visible. At this juncture, the removable splint is progressively weaned during the day and used primarily for protection in crowds or during sleep. Passive Range of Motion (PROM) exercises are cautiously introduced to address any residual capsular contractures. Progressive resistive exercises (PREs) are initiated to rebuild grip strength and forearm muscle endurance. The occupational therapist focuses on integrating the restored motion into functional, task-specific activities of daily living.

Phase IV: Return to High-Demand Activities (>12 Weeks)
Return to heavy manual labor, contact sports, or high-demand activities is generally restricted until there is unequivocal clinical and radiographic evidence of complete osseous union, which typically occurs between 12 and 16 weeks post-operatively. Patients must demonstrate near-normal grip strength (at least 80% of the contralateral side) and a functional, pain-free arc of motion before being cleared for unrestricted activity. Long-term follow-up at 6 months and 1 year is essential to ensure maintenance of correction and to monitor for any late complications such as hardware irritation or delayed DRUJ arthrosis.
Summary of Landmark Literature and Clinical Guidelines
The evolution of corrective osteotomy for forearm malunions has been heavily influenced by several landmark biomechanical and clinical studies. A profound understanding of this literature is essential for any orthopedic surgeon undertaking these complex reconstructions. The foundational biomechanical principles we rely on today were established through rigorous scientific inquiry.
The most critical paper in this domain is undoubtedly the 1992 study by Schemitsch and Richards, published in the Journal of Bone and Joint Surgery. This landmark biomechanical study definitively quantified the normal anatomy of the radial bow and established its direct correlation with functional outcomes. They demonstrated that restoring the maximum radial bow to within 1.5 mm of its normal magnitude, and locating its apex to within 4.3% of the contralateral forearm's apex location, allowed patients to regain over 80% of their normal rotational motion. This paper shifted the paradigm from simple linear realignment to precise, three-dimensional geometric restoration.
Clinically, the work of Trousdale et al. at the Mayo Clinic provided critical insights into the outcomes and complication profiles of forearm osteotomies. Their retrospective reviews highlighted that while functional improvement is reliably achievable, the complication rates—particularly nonunion and nerve injury—are non-trivial, underscoring the need for meticulous technique and rigid fixation. More recently, the advent of 3D computer-assisted planning has been validated by numerous authors, including Oka et al., who demonstrated that patient-specific surgical guides significantly improve the accuracy of rotational and angular correction compared to traditional 2D templating methods. Current clinical guidelines strongly advocate for the use of advanced 3D imaging and templating for all complex, multiplanar diaphyseal malunions to optimize functional recovery and minimize intraoperative guesswork.
