Diaphyseal Forearm Fractures: OR/IF Masterclass

Key Takeaway
Welcome, fellows, to an immersive surgical masterclass on open reduction and internal fixation of diaphyseal forearm fractures. We'll meticulously cover comprehensive surgical anatomy, precise preoperative planning, and granular intraoperative execution using the Henry and subcutaneous approaches. Expect detailed discussions on neurovascular protection, fracture reduction techniques, hardware application, and critical pearls to optimize patient outcomes and manage potential complications.
Comprehensive Introduction and Patho-Epidemiology
Fellows, welcome to the operating theater. Today, we are undertaking a foundational yet extraordinarily complex procedure: Open Reduction and Internal Fixation (OR/IF) of Diaphyseal Forearm Fractures. This intervention is not merely an exercise in carpentry or aligning cortical bone; it is a critical restoration of the intricate biomechanics of a highly specialized limb. The human forearm is designed to facilitate a near 180-degree arc of pronosupination, considerable elbow flexion-extension, and multidirectional wrist circumduction. A successful surgical outcome hinges entirely on precise anatomical reduction and rigid, stable fixation, which together minimize postoperative complications and maximize long-term functional recovery.
Forearm diaphyseal fractures exhibit a classic bimodal epidemiological distribution. We frequently encounter these injuries in young, active males secondary to high-energy mechanisms such as motor vehicle collisions, falls from significant heights, or sports-related trauma. Conversely, there is a distinct peak in the elderly population, predominantly females, where low-energy falls from a standing height lead to fractures in osteoporotic bone. Understanding the energy of the injury is paramount, as high-energy trauma alerts the orthopedic surgeon to the high probability of extensive soft tissue stripping, severe periosteal disruption, and an elevated risk of acute compartment syndrome.
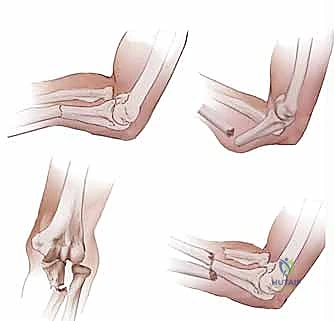
The concept of the forearm as a complex, articulated joint ring cannot be overstated. The radius and ulna are intimately bound by the proximal radioulnar joint (PRUJ), the distal radioulnar joint (DRUJ), and the stout interosseous membrane complex. Because of this rigid, ring-like anatomical relationship, a displaced fracture of one bone frequently results in either a fracture of the paired bone or a dislocation of one of the adjacent radioulnar joints—classically recognized as Monteggia or Galeazzi fracture-dislocations. Treating a diaphyseal fracture of the forearm requires the exact same meticulous attention to anatomical restoration as one would apply to an intra-articular fracture of a major weight-bearing joint.
Failure to respect these biomechanical imperatives leads to predictable and devastating clinical failures. Even minor degrees of angular deformity, rotational malalignment, or narrowing of the interosseous space will dramatically restrict the patient's arc of pronation and supination. Furthermore, inadequate fixation constructs in the face of high-energy comminution will inevitably succumb to the tremendous torsional forces experienced by the forearm during activities of daily living, leading to hardware failure, delayed union, or frank nonunion.
Detailed Surgical Anatomy and Biomechanics
Understanding the intricate and unforgiving anatomy of the forearm is absolutely non-negotiable for the operating surgeon. This anatomical knowledge dictates our surgical approaches, safeguards vital neurovascular structures, and guides our ultimate reduction maneuvers. The forearm's ability to pronate and supinate is a complex, synchronized dance between the radius and ulna, hinged proximally at the PRUJ and distally at the DRUJ.
Osteology and the Crucial Forearm Bows
The biomechanical relationship between the radius and ulna dictates that the radius rotates around a longitudinal axis passing from the center of the radial head proximally to the fovea of the ulnar head distally. The ulna itself is not entirely static; it moves in a subtle varus-valgus arc of approximately 9 degrees during pronosupination, allowing the ulnar head to move clear of the rotating distal radius. At the DRUJ, the primary motion is rotational, but at the physiological extremes, the radius translates dorsally in pronation and palmarly in supination.
The concept of the radial bow is arguably the most critical element of forearm osteology. The radius possesses two distinct bows: a smaller proximal bow with its apex at the biceps tuberosity, and a larger, more critical distal bow with its apex at the insertion of the pronator teres. Restoration of this distal radial bow is paramount for preserving pronation biomechanics. The ulna features a converse anatomical arrangement, possessing a longer, shallower proximal bow dictated by the anconeus insertion, and a very subtle distal bow near the pronator quadratus insertion.
The ligamentous connections between these two bones form the foundation of longitudinal and transverse stability. The annular ligament stabilizes the PRUJ, while the Triangular Fibrocartilage Complex (TFCC) stabilizes the DRUJ. Between them lies the interosseous membrane (IOM), which spans the middle 75% of the diaphysis. The central band of the IOM is a stout ligamentous structure critical for load sharing—transferring axial loads from the distal radius to the proximal ulna—and providing longitudinal stability. Disruption of these structures, particularly in Essex-Lopresti variants, severely complicates diaphyseal fracture management.
Muscular Intervals and Surgical Planes
The musculature of the forearm is a dense, complex arrangement of longitudinal, oblique, and transversely oriented musculotendinous units organized into distinct superficial and deep layers. Our surgical approaches are specifically designed to exploit true internervous planes, thereby minimizing denervation and muscle necrosis. The superficial longitudinal muscles include the brachioradialis (BR), which forms the lateral border of the "mobile wad," and the flexor carpi radialis (FCR) and flexor carpi ulnaris (FCU) anteriorly.
Deeper to these lie the oblique and transverse muscles, which present significant hurdles during surgical exposure. The supinator muscle, with its humeral and ulnar heads, wraps around the proximal radius. The pronator teres originates from the medial epicondyle and arches obliquely to insert at the apex of the radial bow. Distally, the pronator quadratus lies in the floor of the anterior compartment, spanning both bones. Navigating these muscles requires a profound understanding of their nerve supply to safely retract or reflect them during plating.
The classic Volar Henry approach to the radius exploits the internervous plane between the brachioradialis (innervated by the radial nerve) and the flexor carpi radialis (innervated by the median nerve). Conversely, the dorsal Thompson approach utilizes the plane between the extensor carpi radialis brevis (radial nerve) and the extensor digitorum communis (posterior interosseous nerve). Mastery of these planes allows the surgeon to expose the entire length of the radius without compromising motor function.
Neurovascular Structures and Danger Zones
The forearm is traversed by three major nerves—the median, ulnar, and radial nerves—along with the radial and ulnar arteries. Protection of these structures is the primary concern during any diaphyseal exposure. The radial nerve bifurcates at the elbow; its sensory branch continues deep to the BR, closely associated with the radial artery, making it vulnerable during anterior approaches.
The Posterior Interosseous Nerve (PIN) is the most frequently injured structure in proximal radius surgery. It branches from the radial nerve, passes between the two heads of the supinator muscle, and enters the dorsal compartment to innervate the extensor musculature. When utilizing a dorsal or lateral approach to the proximal radius, identifying and protecting the PIN is a mandatory, high-stakes step. Supinating the forearm dynamically shifts the PIN laterally, moving it away from the surgical field during anterior exposures.

The median nerve courses deep to the pronator teres and the fibrous arch of the flexor digitorum superficialis (FDS), while the ulnar nerve runs deep to the FCU. The radial artery, a key landmark in the Henry approach, lies just deep to the fascia along the medial border of the BR. The "leash of Henry," a network of recurrent radial artery branches, must be meticulously identified and ligated to mobilize the proximal radial artery and safely expose the proximal radius.
Exhaustive Indications and Contraindications
The decision to proceed with operative intervention for diaphyseal forearm fractures in adults is generally straightforward, as conservative management of displaced fractures yields universally poor functional results. However, nuanced clinical judgment is required to navigate complex fracture patterns, severe soft tissue injuries, and patient-specific comorbidities.
Surgical stabilization is the gold standard for virtually all displaced adult both-bone forearm fractures. The inherent instability of these fractures, combined with the deforming forces of the robust forearm musculature, makes maintenance of reduction via closed casting nearly impossible. Furthermore, any fracture involving a disruption of the radioulnar joints—specifically Galeazzi (distal radius fracture with DRUJ dislocation) and Monteggia (proximal ulna fracture with PRUJ dislocation) fracture-dislocations—mandates immediate open reduction and rigid internal fixation to restore joint congruity and prevent chronic instability.
| Parameter | Absolute Indications for OR/IF | Relative Indications / Considerations | Contraindications for Immediate OR/IF |
|---|---|---|---|
| Fracture Pattern | Displaced both-bone fractures; Galeazzi fractures; Monteggia fractures. | Isolated, minimally displaced ulna fractures failing conservative care. | Undisplaced, stable isolated fractures (e.g., non-displaced nightstick). |
| Soft Tissue | Open fractures (requires urgent debridement + fixation); Acute compartment syndrome. | Severe soft tissue swelling without compartment syndrome (may delay). | Active, untreated deep infection at the surgical site. |
| Vascular/Neuro | Associated arterial injury requiring repair; Progressive neurological deficit. | Static, non-progressive nerve palsy associated with closed injury. | Medically unstable polytrauma patient (damage control orthopedics preferred). |
| Patient Factors | Polytrauma requiring early mobilization; Floating elbow injuries. | Non-compliant patient; Severe osteoporosis (requires specialized implants). | Terminal illness with extremely limited life expectancy and minimal pain. |
Contraindications to immediate definitive internal fixation are relatively few but critically important. The most pressing is the medically unstable polytrauma patient "in extremis," where prolonged surgical times for definitive plating are life-threatening. In such damage-control scenarios, rapid application of a spanning external fixator is the procedure of choice. Similarly, grossly contaminated open fractures with extensive soft tissue loss may require initial external fixation and serial debridements before definitive internal plating can be safely performed.
Relative indications often revolve around isolated ulnar shaft fractures (the classic "nightstick" fracture). While undisplaced fractures can be managed with functional bracing, those with greater than 50% displacement, more than 10 degrees of angulation, or involving the proximal third of the ulna are at a high risk for nonunion and should be strongly considered for primary operative fixation.
Pre-Operative Planning, Templating, and Patient Positioning
Before a surgical blade ever touches the patient's skin, a phase of meticulous, exhaustive preoperative planning must be undertaken. For diaphyseal forearm fractures, where the tolerance for malalignment is virtually zero, the stakes are exceptionally high. Any residual angulation, rotational deformity, or failure to restore the interosseous space will severely compromise the patient's functional outcome.
Clinical Assessment and Imaging
The initial assessment begins with a thorough history to ascertain the mechanism of injury, which informs the surgeon regarding the energy imparted to the limb. A high-energy crush injury or motor vehicle accident raises the index of suspicion for severe soft tissue compromise and impending compartment syndrome. The physical examination must rigorously evaluate the skin for traumatic arthrotomies or open wounds, which dictate the timing and urgency of the procedure.
High-quality orthogonal radiographs are the cornerstone of preoperative planning. True anteroposterior (AP) and lateral views of the entire forearm, explicitly including both the elbow and wrist joints, are mandatory to rule out associated Monteggia or Galeazzi variants. In cases of severe comminution or when articular extension is suspected, a fine-cut computed tomography (CT) scan with 3D reconstructions is invaluable for understanding the fracture morphology and planning screw trajectories.

The Art of Preoperative Templating
Templating is not a mere academic exercise; it is a critical step in ensuring the restoration of the radial bow. As established by the landmark work of Schemitsch and Richards, the restoration of the maximum radial bow is the single most important variable in recovering full pronosupination. The normal radial bow measures 15.3 ± 0.3 mm and is located at approximately 60% of the total length of the radius, measured from the bicipital tuberosity to the sigmoid notch.
Using digital templating software or traditional acetate overlays on contralateral intact forearm films, the surgeon must calculate the required plate length and the specific contour needed to recreate this bow. Modern pre-contoured locking compression plates (LCPs) provide an excellent starting point, but intraoperative fine-tuning with plate benders is frequently required. Failure to template often leads to the selection of an inappropriately straight plate, which will flatten the radial bow and tether the interosseous membrane, permanently restricting rotation.

Patient Positioning and Operating Room Setup
Proper positioning is essential for seamless intraoperative workflow and unobstructed fluoroscopic imaging. The patient is placed supine on the operating table. The affected arm is meticulously prepped and draped free from the axilla to the fingertips, allowing the surgeon full access to the forearm, elbow, and wrist, and permitting unhindered pronation and supination during the procedure.
A sterile pneumatic tourniquet is applied high on the brachium to provide a bloodless surgical field, though it should be deflated periodically during prolonged cases to minimize ischemic damage to the musculature. The arm is placed on a radiolucent hand table. The C-arm fluoroscopy unit is positioned either parallel or perpendicular to the table, depending on surgeon preference, but it must be able to obtain true AP and lateral views of the entire forearm without requiring awkward manipulation of the fractured limb.
Step-by-Step Surgical Approach and Fixation Technique
The intraoperative execution of forearm plating requires a methodical, step-by-step approach. In both-bone fractures, it is generally recommended to tackle the less comminuted bone first—most frequently the ulna. Fixing the simpler fracture restores the longitudinal length of the forearm, providing a stable anatomical framework that significantly facilitates the reduction of the more complex, paired bone.
The Subcutaneous Approach to the Ulna
The ulna is uniquely accessible due to its subcutaneous position along the posterior border of the forearm. This allows for a direct approach that minimizes soft tissue dissection and avoids major neurovascular structures, provided the surgeon stays true to the anatomical planes.
The patient's arm is positioned across the chest or on the hand table with the elbow flexed and the forearm fully pronated. A straight longitudinal incision is made directly over the palpable subcutaneous border of the ulna, centered over the fracture site. The length of the incision must be generous enough to allow the application of a plate that provides at least three, and ideally four, holes of fixation (six to eight cortices) on each side of the fracture.



Subcutaneous dissection is carried down to the deep fascia. The internervous plane lies between the extensor carpi ulnaris (ECU), innervated by the posterior interosseous nerve, and the flexor carpi ulnaris (FCU), innervated by the ulnar nerve. The deep fascia is incised longitudinally directly over the ulnar crest.


Subperiosteal elevation is then performed to expose the fracture ends. It is critical to elevate the periosteum only as much as necessary to apply the plate; aggressive circumferential stripping will devascularize the bone fragments and drastically increase the risk of delayed union or nonunion. The fracture is debrided of hematoma and interposed soft tissue, preparing it for reduction.



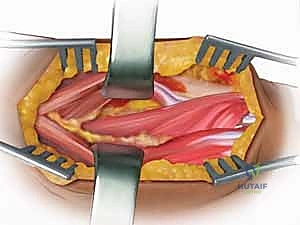
The Volar Henry Approach to the Radius
The volar approach, popularized by A.K. Henry, is highly versatile and allows safe exposure of the entire length of the radius. It exploits the internervous plane between the brachioradialis (radial nerve) and the flexor carpi radialis (median nerve).
The arm is supinated, and a longitudinal incision is made along the course of the FCR tendon, curving slightly laterally at the elbow crease if proximal extension is required. After incising the superficial fascia, the BR is retracted laterally and the FCR medially. The radial artery is identified beneath the BR and must be carefully mobilized and retracted medially with its associated venae comitantes.


To expose the proximal third of the radius, the "leash of Henry"—a series of recurrent radial artery branches—must be identified, ligated, and divided. This allows the radial artery to be safely retracted. The supinator muscle is then identified. To protect the PIN, the forearm is fully supinated, moving the nerve laterally. The supinator is incised along its ulnar insertion and reflected laterally, exposing the proximal radius.


For midshaft exposures, the pronator teres is identified. If it impedes plate placement, it can be elevated from its radial insertion, taking care to repair it during closure. Distally, the pronator quadratus and flexor pollicis longus are elevated subperiosteally to expose the volar surface of the distal radius.
The Dorsal Thompson Approach to the Proximal Radius
The dorsal approach is particularly useful for fractures of the proximal and middle thirds of the radius, especially when a dorsal plate application is desired. It utilizes the internervous plane between the extensor carpi radialis brevis (ECRB, radial nerve) and the extensor digitorum communis (EDC, posterior interosseous nerve).
With the forearm pronated, a straight incision is made from the lateral epicondyle toward the Lister's tubercle. The fascia is incised, and the interval between the ECRB and EDC is developed. The deep dissection reveals the supinator muscle overlying the proximal radius and the abductor pollicis longus (APL) and extensor pollicis brevis (EPB) outcropping muscles more distally.


The critical step in the Thompson approach is the identification and protection of the PIN. The nerve can be found exiting the supinator distally. The supinator is carefully elevated off the radius, ensuring the nerve remains protected within the muscle substance. Retractors must be placed with extreme caution to avoid traction neuropraxia.
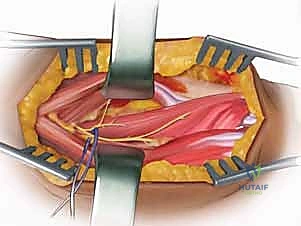
Reduction Techniques and Internal Fixation Principles
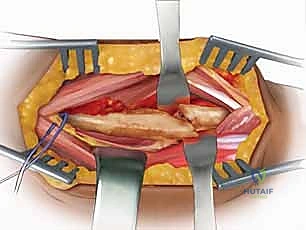
Once the fractures are exposed, anatomical reduction is achieved using reduction forceps, taking care not to crush the cortical bone. For oblique or spiral fractures, interfragmentary lag screws are utilized to achieve absolute stability and primary bone healing. The lag screw is placed perpendicular to the fracture plane, overdrilling the near cortex to create compression.


Definitive fixation is achieved with 3.5 mm dynamic compression plates (DCP), limited contact dynamic compression plates (LC-DCP), or locking compression plates (LCP). The plate must be perfectly contoured to match the radial bow. A minimum of three bicortical screws (six cortices) is required on each side of the fracture, though four screws (eight cortices) are highly preferred for diaphyseal stability. In cases of severe comminution where anatomical reduction is impossible, the plate is used in a bridge plating fashion to maintain length, alignment, and rotation while preserving the fracture hematoma.


