Structural Allograft Reconstruction for Large Talar Osteochondral Lesions: A Masterclass

Key Takeaway
Welcome to the OR, fellows. Today, we're tackling a structural allograft reconstruction for a large osteochondral lesion of the talus. This masterclass will cover meticulous preoperative planning, precise patient positioning, and a step-by-step intraoperative execution, emphasizing critical anatomical considerations and advanced surgical techniques. We'll delve into pearls, pitfalls, and comprehensive postoperative care, ensuring you master this complex procedure.
Comprehensive Introduction and Patho-Epidemiology
Osteochondral lesions of the talus (OLTs) represent a formidable challenge in orthopedic foot and ankle surgery, particularly when these defects are large, uncontained, or associated with massive subchondral cystic changes. While small, symptomatic lesions often respond favorably to arthroscopic marrow stimulation techniques such as microfracture, large-volume defects—typically defined as those exceeding 1.5 square centimeters in area or 3 cubic centimeters in volume—demonstrate unacceptably high failure rates with joint-sparing, reparative procedures. The fibrocartilage generated by marrow stimulation lacks the complex, organized extracellular matrix and robust biomechanical properties of native hyaline cartilage, leading to inevitable breakdown under the immense contact stresses of the ankle mortise.
When dealing with massive OLTs, particularly those involving the talar shoulder—the critical biomechanical transition zone where the superior talar dome articulates with the medial or lateral malleolus—structural allograft reconstruction emerges as the premier joint-preserving intervention. This masterclass focuses on the utilization of fresh osteochondral allografts (FOCA), a technique that allows for the transplantation of mature, metabolically active hyaline cartilage alongside a structurally intact subchondral bone plate. Unlike synthetic scaffolds or particulate juvenile cartilage, massive structural allografts provide immediate mechanical stability and true anatomical restoration of the articular contour, which is paramount in a highly congruent joint like the ankle.
The pathogenesis of these large-volume lesions is multifactorial, though the prevailing consensus points toward a combination of acute trauma, repetitive microtrauma, and idiopathic focal avascular necrosis. Traumatic shear forces during ankle inversion or eversion injuries can cause osteochondral fractures, disrupting the tenuous vascular supply to the subchondral bone. Over time, the necrotic bone fragment may resorb or detach, leading to a cascade of synovial fluid intrusion, elevated intraosseous pressure, and the formation of expansile subchondral cysts. If left untreated, the natural history of a large, uncontained OLT is a predictable progression toward altered joint kinematics, asymmetrical contact stresses, subchondral collapse, and end-stage tibiotalar osteoarthritis.
Our primary objective with structural allograft reconstruction is to fundamentally interrupt this degenerative cascade. By excising the necrotic, cystic bone and replacing it with a precisely contoured, viable osteochondral unit, we aim to restore the normal biomechanical environment of the ankle. This procedure is technically demanding, requiring meticulous preoperative templating, precise surgical execution, and a profound understanding of ankle anatomy and biomechanics. However, when performed correctly in properly selected patients, it offers a profound opportunity to salvage the joint, alleviate debilitating chronic pain, and significantly delay or entirely circumvent the need for joint-sacrificing procedures such as ankle arthrodesis or total ankle arthroplasty.
Detailed Surgical Anatomy and Biomechanics
Osseous Architecture and Articular Congruency
The talus is a uniquely complex osseous structure, distinguished by the fact that approximately 60% to 70% of its surface area is covered by articular cartilage. It acts as the central keystone of the ankle mortise, lacking any direct muscular or tendinous attachments, which renders its position and stability entirely dependent on the surrounding capsuloligamentous structures and the congruency of its articulations. The superior talar dome, or trochlea, is wider anteriorly than posteriorly, a geometric feature that imparts inherent stability to the ankle in dorsiflexion while allowing for subtle rotational laxity in plantarflexion. The medial and lateral articular facets of the talus interface with their respective malleoli, creating a highly constrained, mortise-and-tenon joint configuration.
Because of this profound congruency, the ankle joint is exquisitely sensitive to even microscopic alterations in anatomical alignment. Landmark biomechanical studies have demonstrated that a mere 1-millimeter lateral shift of the talus can reduce the tibiotalar contact area by up to 42%, exponentially increasing peak contact stresses. This biomechanical reality underscores the absolute necessity of precise allograft sizing and contouring. An allograft that is left "proud" (protruding above the native cartilage) will act as a focal stress riser, leading to accelerated wear of the opposing tibial plafond (a "kissing lesion") and premature graft failure. Conversely, a graft that is countersunk will fail to participate in load sharing, leading to surrounding native cartilage overload and progressive degeneration.
Vascular Supply and Watershed Zones
Understanding the tenuous and retrograde vascular supply of the talus is critical for both comprehending the etiology of OLTs and executing surgical approaches safely. The talus is perfused by an intricate extraosseous anastomotic ring formed by the three major arteries of the lower leg: the posterior tibial, anterior tibial (dorsalis pedis), and peroneal arteries. The posterior tibial artery provides the most significant contribution via the artery of the tarsal canal, which supplies the majority of the talar body. The artery of the sinus tarsi, formed by anastomoses between the perforating peroneal and dorsalis pedis arteries, supplies the anterolateral aspect of the talar body and head.
Crucially, the blood supply to the talar dome enters distally and courses proximally in a retrograde fashion. This vascular architecture creates distinct "watershed" zones within the subchondral bone, rendering the superior articular surface highly susceptible to avascular necrosis following trauma. During our surgical approach, particularly when performing a medial malleolar osteotomy, we must be exquisitely careful to preserve the deltoid ligament branches of the posterior tibial artery. Excessive stripping of the periosteum or capsular attachments can further devascularize the talus, compromising the integration of the allograft and increasing the risk of postoperative talar body collapse.
Soft Tissue Envelope and Neurovascular Relations
Navigating the medial soft tissue envelope requires a meticulous, layered dissection to avoid catastrophic iatrogenic injury. The great saphenous vein and the accompanying saphenous nerve course superficially over the medial malleolus. The saphenous nerve provides critical sensory innervation to the medial aspect of the foot and ankle; its transection or entrapment in scar tissue can result in debilitating neuromas and postoperative dysesthesias that often overshadow the success of the osseous reconstruction. Deep to the superficial fascia lies the flexor retinaculum, which roofs the tarsal tunnel.
Immediately posterior to the medial malleolus, within the primary retromalleolar groove, courses the posterior tibial tendon (PTT). The PTT is the primary dynamic stabilizer of the medial longitudinal arch and a critical structure that must be mobilized and protected during a medial malleolar osteotomy. Deep to the PTT lies the deltoid ligament complex, a robust stabilization system comprising superficial (tibionavicular, tibiocalcaneal, and superficial tibiotalar) and deep (anterior and posterior tibiotalar) components. The deep deltoid ligament is the primary restraint to lateral talar excursion and external rotation. While the medial malleolar osteotomy inevitably violates portions of the joint capsule, our osteotomy trajectory must be planned to preserve the deep deltoid attachments to the distal malleolar fragment, ensuring that the vascularity and stabilizing function of the ligament are maintained upon repair.
Exhaustive Indications and Contraindications
Patient selection is the absolute cornerstone of success in structural allograft reconstruction. This is a salvage procedure, and applying it to the wrong patient population will reliably yield catastrophic failures. The ideal candidate is a younger, active patient with a focal, massive osteochondral defect, normal lower extremity alignment, and a stable ankle mortise.
When considering indications, we look for large-volume lesions (>1.5 cm²) or deep cystic lesions (>3cc) where the subchondral bone plate is structurally compromised. Patients who have failed prior marrow stimulation techniques (e.g., microfracture, drilling) are prime candidates, as the subchondral bone in these cases is often sclerotic and incapable of supporting further reparative attempts. Uncontained lesions involving the talar shoulder are also strong indications, as cylindrical osteochondral autograft transfer (OATS) procedures are geometrically ill-suited to reconstruct the complex, multi-planar curvature of the talar edge.
Contraindications must be strictly respected. "Kissing lesions"—where full-thickness cartilage loss is present on the opposing tibial plafond—are an absolute contraindication, as the implanted allograft will rapidly degrade against the bare tibial bone. Diffuse tibiotalar osteoarthritis, active intra-articular infection, and uncorrected severe malalignment (varus or valgus hindfoot) will uniformly lead to graft failure due to abnormal contact stresses. Furthermore, patient-specific factors such as active tobacco use, uncontrolled diabetes mellitus, and Charcot neuroarthropathy severely compromise bone healing and graft incorporation, rendering the procedure highly inadvisable.
| Parameter | Indications for Structural Allograft | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Lesion Size | Large area (>1.5 cm²) or deep volume (>3cc) | Small, contained lesions (<1.0 cm²) | Moderate lesions amenable to OATS |
| Lesion Morphology | Uncontained, talar shoulder involvement, massive subchondral cysts | Diffuse tibiotalar osteoarthritis | Multiple, disparate focal lesions |
| Prior Surgery | Failed prior microfracture or marrow stimulation | Active joint infection or osteomyelitis | Prior failed structural allograft |
| Joint Status | Intact opposing tibial plafond cartilage | "Kissing lesions" (tibial plafond damage) | Mild, asymptomatic osteophyte formation |
| Alignment | Neutral hindfoot and ankle alignment | Uncorrectable severe varus/valgus malalignment | Correctable malalignment (requires concurrent osteotomy) |
| Patient Factors | High functional demand, compliant with NWB rehab | Active smoker, Charcot arthropathy, severe neuropathy | BMI > 35, poorly controlled diabetes |
Pre-Operative Planning, Templating, and Patient Positioning
Advanced Imaging and 3D Templating
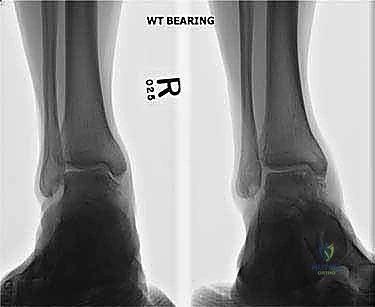
Standard weight-bearing orthogonal radiographs are merely the starting point; they are wholly insufficient for surgical planning in large OLTs. While they help rule out diffuse joint space narrowing and gross malalignment, they drastically underestimate defect size. Magnetic Resonance Imaging (MRI) is excellent for assessing the integrity of the surrounding cartilage and identifying subchondral edema, but the marrow edema footprint often exaggerates the true osseous void, leading to overestimation of the required graft size.
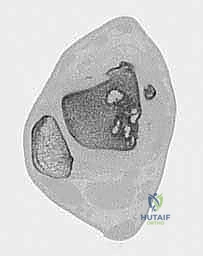
The undisputed gold standard for preoperative planning is a high-resolution, thin-slice Computed Tomography (CT) scan. CT provides precise, three-dimensional spatial resolution of the subchondral bone plate and the exact dimensions of the cystic void. We utilize advanced 3D reconstruction software to map the defect's length, width, and depth to the millimeter. This data is critical for communicating with the tissue bank. We perform virtual templating, superimposing geometric shapes (cylinders or blocks) over the defect to determine the optimal graft configuration and to ensure that the planned medial malleolar osteotomy will provide adequate surgical access to the entire lesion.
Allograft Procurement and Chondrocyte Viability
The logistics of procuring a fresh osteochondral allograft (FOCA) require rigorous coordination. We adhere strictly to the JUPITER (Justification for Use of Post-Traumatic Inflammatory Phase Treatments and Early Rehabilitation) guidelines and established tissue bank protocols. The term "fresh" is critical; unlike frozen or irradiated bone grafts, FOCAs are stored at 4°C in specialized nutrient media to maintain chondrocyte viability. Chondrocytes are the metabolic engines of the cartilage matrix, and their survival is paramount for the long-term durability of the graft.
The window for implantation is narrow, typically between 14 and 28 days post-procurement. Prior to 14 days, comprehensive viral and bacterial serologic testing (including HIV, Hepatitis B/C, and Syphilis) is pending. Beyond 28 days, chondrocyte senescence accelerates rapidly, and the cell viability drops below the threshold required for clinical success. We provide the tissue bank with the precise CT measurements and specify the laterality (left or right). The bank then matches a donor talus based on size, geometry, and radius of curvature. Upon arrival in the operating room, the allograft is meticulously inspected for any macroscopic cartilage fissures, softening, or signs of degradation before the patient is anesthetized.
Patient Positioning and Operating Room Setup
Proper patient positioning is the foundation of a smooth surgical workflow. The patient is placed supine on a radiolucent operating table. For a medial OLT requiring a medial malleolar osteotomy, we place a substantial bump or bolster under the ipsilateral hip. This induces a slight internal rotation of the entire lower extremity, which naturally positions the ankle in external rotation, bringing the medial malleolus directly anterior and parallel to the floor. This orientation is crucial for visualizing the osteotomy trajectory and ensuring orthogonal hardware placement.
A well-padded pneumatic tourniquet is applied to the proximal thigh. A bloodless surgical field is absolutely non-negotiable for this procedure; the intricate preparation of the recipient bed and the precise visual matching of the allograft cartilage height cannot be performed safely in a bloody field. The tourniquet is inflated only after exsanguination with an Esmarch bandage, immediately prior to incision. The fluoroscopy unit (C-arm) is positioned on the contralateral side of the table, draped sterilely, and tested before the incision to ensure unobstructed anteroposterior (AP), lateral, and mortise views of the ankle joint can be obtained instantaneously.
Step-by-Step Surgical Approach and Fixation Technique
Incision, Superficial Dissection, and Arthrotomy
The procedure begins with a meticulously planned curvilinear incision, approximately 10 to 12 centimeters in length, centered directly over the medial malleolus. The incision starts proximally along the anterior crest of the tibia, curves gently over the center of the medial malleolus, and extends distally toward the navicular tuberosity.

Subcutaneous dissection must be performed with extreme caution. Utilizing blunt dissection techniques, we identify and mobilize the great saphenous vein and the saphenous nerve. These structures are gently retracted anteriorly with a vessel loop to prevent iatrogenic traction injury.


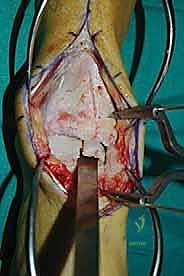
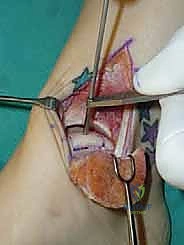
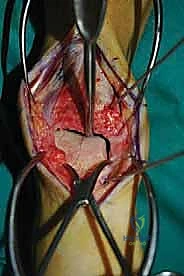
Once the superficial neurovascular bundle is protected, we proceed to an anterior ankle arthrotomy. The anterior capsule is incised longitudinally, allowing for direct visualization of the anterior aspect of the tibiotalar joint. This step is critical; it allows us to palpate the anterior margin of the OLT and visually confirm the health of the anterior tibial plafond. Following the arthrotomy, we turn our attention posteriorly. The flexor retinaculum is incised, and the sheath of the posterior tibial tendon (PTT) is opened. The PTT is mobilized from its retromalleolar groove and retracted posteriorly using a blunt Hohmann retractor, safeguarding it from the impending osteotomy.



Execution of the Medial Malleolar Osteotomy
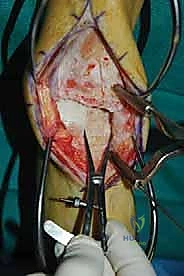
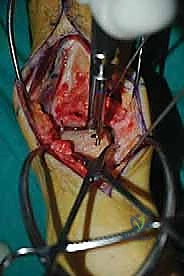
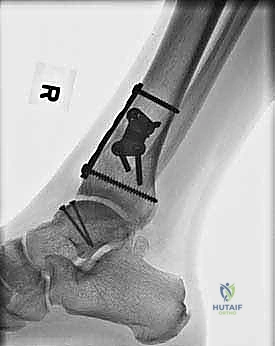
To gain unhindered access to the central and posterior aspects of the medial talar dome, a medial malleolar osteotomy is required. We prefer an oblique osteotomy directed at the axilla of the medial malleolus, as it provides excellent exposure and a broad cancellous surface area for reliable bone healing. We begin by pre-drilling the osteotomy site to facilitate accurate anatomic reduction later. Two parallel 0.062-inch Kirschner wires are driven from the tip of the medial malleolus, directed proximally and laterally into the tibial metaphysis. These tracts are then over-drilled and tapped for 4.0mm partially threaded cancellous screws, after which the screws and wires are removed.



Using a surgical marker, the osteotomy line is drawn. We utilize a micro-sagittal saw to initiate the cut. The saw blade is directed toward the intersection of the medial malleolus and the tibial plafond (the axilla). It is imperative to use intraoperative fluoroscopy during this step to ensure the saw blade does not inadvertently violate the weight-bearing cartilage of the tibial plafond.



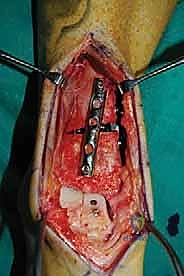
As the saw blade approaches the articular cartilage, we stop. The final few millimeters of the osteotomy are completed using a sharp osteotome. This "break-away" technique creates a rough, interdigitating cartilaginous and osseous surface that acts as an anatomic key, ensuring perfect rotational alignment during closure. The medial malleolar fragment, with the deltoid ligament still firmly attached, is then reflected distally and plantarward, completely exposing the medial talar dome and the offending lesion.


Recipient Bed Preparation and Defect Templating
With the lesion fully exposed, we meticulously assess its borders. All necrotic cartilage, fibrous tissue, and sclerotic subchondral bone must be aggressively debrided back to a rim of healthy, bleeding bone and stable, vertically oriented native cartilage margins. For contained lesions, we utilize specialized cylindrical reamers. A guide pin is placed perpendicularly into the center of the defect, and a cannulated reamer is passed over it to create a perfectly cylindrical recipient socket.


For uncontained lesions involving the talar shoulder, a cylindrical reamer is insufficient. In these cases, we must perform a "box cut" or trapezoidal resection. Using a combination of a micro-sagittal saw and high-speed burrs, we fashion a precise geometric void.

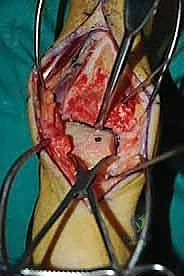

The depth of the resection is dictated by the extent of the subchondral cyst; we must reach healthy, punctate bleeding cancellous bone to ensure vascular ingress into the allograft. Copious chilled saline irrigation is used continuously during bone preparation to prevent thermal necrosis of the surrounding native tissues. Once the recipient bed is finalized, precise measurements (depth at four quadrants, diameter, and width) are taken using a sterile caliper.


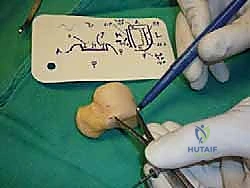
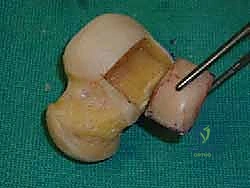
Allograft Harvesting, Contouring, and Implantation
Attention is now turned to the back table, where the fresh donor talus is secured in a specialized allograft workstation. Using the measurements obtained from the recipient bed, we map the corresponding topographical location on the donor talus to ensure the radius of curvature matches perfectly. For cylindrical grafts, a coring reamer slightly larger (typically 0.5mm to 1.0mm) than the recipient socket is used to harvest the plug, allowing for a secure press-fit.


For box cuts, the donor graft is meticulously sculpted using a saw. Throughout the cutting process, the graft is continuously irrigated with cold saline to preserve chondrocyte viability. Once harvested, the osseous portion of the allograft is aggressively pulse-lavaged with saline. This critical step removes donor marrow elements, lipids, and immunogenic cellular debris from the cancellous bone interstices, significantly reducing the risk of an inflammatory immune response and facilitating host bone ingrowth via creeping substitution.

The graft is then brought to the surgical field. It is gently impacted into the recipient bed using an oversized tamp. The articular surface must be perfectly flush with the surrounding native cartilage. If the graft is proud, it is removed, and the osseous base is trimmed.



Once a flush, stable press-fit is achieved, supplementary fixation is often required for large or uncontained grafts to prevent micromotion. We utilize headless titanium compression screws or bioabsorbable poly-L-lactic acid (PLLA) pins, driven from the non-articular margins or countersunk deeply beneath the cartilage surface.


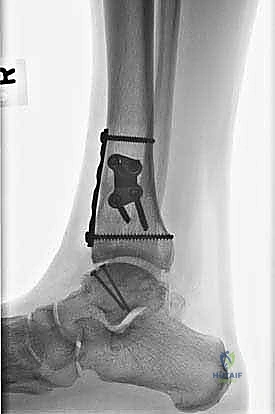
Osteotomy Closure and Final Fixation
With the allograft securely in place, the ankle joint is thoroughly irrigated to remove any remaining osseous debris. The medial malleolar fragment is anatomically reduced back to its native position, utilizing the interdigitating fracture lines as a guide. The pre-drilled tracts are located, and the two 4.0mm partially threaded cancellous screws are inserted and tightened, providing rigid interfragmentary compression.