Mastering Orthopaedic Trauma Principles and Open Fracture Management
Key Takeaway
The management of polytraumatized patients requires a multidisciplinary approach centered on Advanced Trauma Life Support (ATLS) protocols and Damage Control Orthopaedics (DCO). This comprehensive guide details the evidence-based evaluation of musculoskeletal injuries, the OTA 2010 open fracture classification, updated antibiotic prophylaxis guidelines, and surgical strategies for ballistic trauma. Early stabilization and physiological resuscitation remain paramount in mitigating systemic inflammatory responses and preventing mortality.
INTRODUCTION TO POLYTRAUMA MANAGEMENT
The treatment of patients with multiple traumatic injuries demands a highly coordinated, multidisciplinary approach and resources that are frequently unavailable in smaller community hospitals. The acute stabilization of long bone, pelvic, and spinal fractures requires specialized equipment, highly trained orthopaedic trauma surgeons, and dedicated nursing support personnel operating under stringent trauma center protocols.
Extensive epidemiological data documents that treatment in a Level 1 or Level 2 trauma center significantly improves the survival rates and functional outcomes of polytraumatized patients. Furthermore, the length of hospital stay and the overall economic burden of treatment are substantially lower for patients triaged directly to trauma centers compared to those who undergo secondary transfer. However, for patients who initially present to non-trauma centers, rapid secondary transfer confers a distinct survival benefit, with studies demonstrating a significantly lower 30-day mortality rate. Therefore, the gold standard for the management of multiple-injury patients—both in terms of clinical efficacy and health economics—is immediate referral and transport to a dedicated trauma center.
THE ATLS PROTOCOL IN ORTHOPAEDIC TRAUMA
The Advanced Trauma Life Support (ATLS) system, developed by the American College of Surgeons, remains the universal algorithmic foundation for evaluating and resuscitating trauma patients. The primary survey is dictated by the ABCDE mnemonic, which orthopaedic surgeons must integrate into their initial assessment:
- A - Airway: Ensure a patent and unobstructed airway while maintaining strict cervical spine precautions. Cervical spine clearance protocols must be adhered to before any rigid collar is removed.
- B - Breathing: Assess for adequate oxygenation and ventilation. Orthopaedic surgeons must be vigilant for thoracic cage injuries, such as flail chest or multiple rib fractures, which can severely compromise respiratory mechanics.
- C - Circulation: Evaluate both central and peripheral perfusion. The clinical goal is robust capillary refill in all extremities and the maintenance of normotension. Life-threatening orthopaedic hemorrhage (e.g., unstable pelvic ring disruptions, multiple long-bone fractures) must be controlled immediately.
- D - Disability: Conduct a rapid neurological assessment (Glasgow Coma Scale) and a focused musculoskeletal, urological, and reproductive evaluation. While peripheral nerve injuries or isolated fractures may not be immediately life-threatening, failure to diagnose them can result in devastating long-term disability.
- E - Environment/Exposure: Completely undress the patient to identify all injuries, but aggressively prevent hypothermia. Hypothermia exacerbates coagulopathy and acidosis, completing the "lethal triad" of trauma. Furthermore, exposure to environmental contaminants in open fractures poses a severe risk of infection to the patient and potential disease transmission to caregivers.
Clinical Pearl: Blind clamping of bleeding vessels deep within a wound is strictly contraindicated due to the high risk of iatrogenic injury to adjacent peripheral nerves. Direct, sustained manual pressure is the safest and most effective initial method for controlling extremity hemorrhage. Tourniquets should be reserved for life-threatening arterial bleeding that is refractory to direct pressure.
DAMAGE CONTROL ORTHOPAEDICS (DCO)
Polytrauma initiates a massive cascade of cellular and biochemical events, leading to a systemic immune response syndrome (SIRS). This diffuse inflammatory reaction is mediated by cytokines (such as IL-6 and TNF-alpha) released in response to massive tissue injury. Elevated cytokine levels are directly correlated with acute respiratory distress syndrome (ARDS) and multiple organ dysfunction syndrome (MODS).
Historically, Early Total Care (ETC)—the definitive fixation of all fractures within the first 24 hours—was advocated to mobilize patients and reduce pulmonary complications. However, in physiologically unstable or borderline patients, the prolonged surgical time and additional blood loss associated with ETC act as a "second hit," exacerbating the SIRS response and increasing mortality.
Damage Control Orthopaedics (DCO) was developed to mitigate this double insult. DCO is a phased approach:
1. Immediate Resuscitation: Restoration of physiological stability (reversal of coagulopathy, hypothermia, and acidosis).
2. Temporary Stabilization: Rapid, minimally invasive stabilization of major fractures (typically via external fixation) to control hemorrhage and reduce pain without inflicting significant additional surgical trauma.
3. ICU Optimization: Physiological restoration in the intensive care unit.
4. Definitive Reconstruction: Conversion of temporary external fixators to definitive internal fixation (e.g., intramedullary nails or plates) once the patient is physiologically optimized, typically 5 to 10 days post-injury.
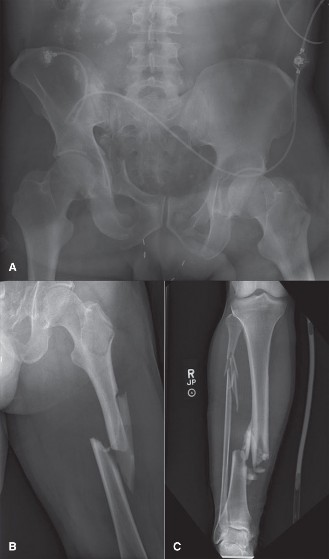
Figure 1: Initial presentation of a severe Type IIIA open tibial fracture. Note the extensive soft tissue disruption and contamination, necessitating urgent evaluation and damage control principles.

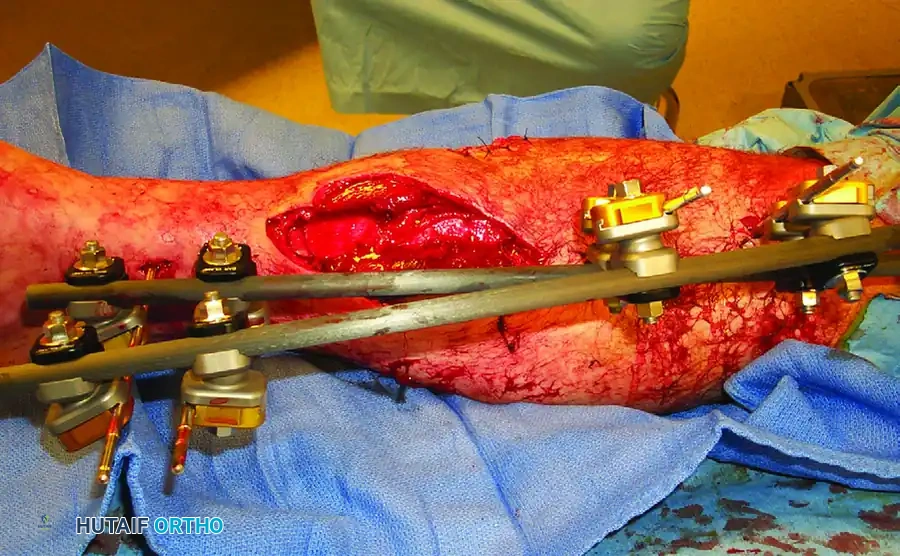
Figure 2: Damage control orthopaedics in action. The same Type IIIA open tibial fracture has been rapidly stabilized with a spanning external fixator, allowing for soft tissue resuscitation and physiological recovery prior to definitive fixation.
EVALUATION AND PREVENTION OF MISSED INJURIES
Despite rigorous primary and secondary surveys, an estimated 5% to 20% of polytrauma patients sustain injuries that go unrecognized during the initial evaluation. Factors contributing to missed injuries include:
* Altered level of consciousness (traumatic brain injury, intubation, sedation).
* Hemodynamic instability precluding a comprehensive orthopaedic examination.
* Distracting injuries (a severely mangled extremity masking a subtle contralateral injury).
* Inadequate or poorly positioned initial radiographs.
Surgical Warning: A formal "Tertiary Survey" is mandatory for all polytrauma patients. This consists of a comprehensive head-to-toe re-examination and a review of all radiological studies once the patient is conscious, extubated, and physiologically stable.
Modern trauma protocols heavily rely on computed tomography (CT). Studies consistently demonstrate that CT evaluation of the cervical spine and pelvis identifies significantly more fractures and ligamentous injuries than plain radiography, making it the gold standard for initial screening in high-energy trauma.
OPEN FRACTURE MANAGEMENT
The management of open fractures has evolved significantly, moving away from dogmatic historical rules toward nuanced, evidence-based protocols.
The OTA 2010 Open Fracture Classification
While the Gustilo-Anderson classification remains widely recognized, the Orthopaedic Trauma Association (OTA) proposed a more comprehensive and standardized classification scheme in 2010 to better guide treatment and predict outcomes.
Skin
1. Can be approximated
2. Cannot be approximated
3. Extensive degloving
Muscle
1. No muscle in area, no appreciable muscle necrosis, some muscle injury with intact muscle function
2. Loss of muscle but the muscle remains functional, some localized necrosis in the zone of injury that requires excision, intact muscle-tendon unit
3. Dead muscle, loss of muscle function, partial or complete compartment excision, complete disruption of a muscle-tendon unit, muscle defect does not approximate
Arterial
1. No injury
2. Artery injury without ischemia
3. Artery injury with ischemia
Contamination
1. No or minimal contamination
2. Surface contamination (easily removed, not embedded in bone or deep soft tissues)
3. (a) Embedded in bone or deep soft tissues; (b) High-risk environmental conditions (e.g., barnyard, fecal matter, dirty water)
Bone Loss
1. None
2. Bone missing or devascularized but still some contact between proximal and distal fragments
3. Segmental bone loss
Paradigm Shifts in Debridement and Antibiotic Prophylaxis
Historically, the "6-hour rule" dictated that all open fractures required formal surgical debridement within six hours of injury to prevent infection. However, contemporary literature has robustly challenged this dogma. Multiple high-quality studies have demonstrated that delaying surgical debridement up to 24 hours does not increase the risk of infection or nonunion, provided that the patient receives early, appropriate intravenous antibiotics. This delay is considered safe for most open fractures up to Gustilo-Anderson Type IIIA, allowing surgery to be performed by specialized orthopaedic trauma teams during daylight hours, thereby decreasing morbidity and hospital stay.
Furthermore, the requirements for prolonged prophylactic antibiotics are being critically re-evaluated. Recent literature reviews have highlighted the poor methodological quality of older studies that advocated for extended antibiotic courses. The current consensus emphasizes the rapid administration of prophylactic antibiotics within 1 to 2 hours of admission as the single most critical factor in preventing infection. The duration of antibiotic therapy is increasingly being shortened, with many centers advocating for discontinuation within 24 hours of wound closure for low-grade open fractures.
BALLISTIC AND FIREARM INJURIES
The evaluation of a patient with a firearm-induced open fracture must include orthogonal (anteroposterior and lateral) radiographs of the injured segment, encompassing the joints above and below. Arthrography or CT scanning is highly recommended to identify intra-articular projectiles or subtle articular step-offs. If the trajectory suggests proximity to major neurovascular bundles, CT angiography (CTA) or formal arteriography is mandatory to rule out intimal tears, pseudoaneurysms, or transections.
Civilian firearm wounds are broadly categorized into three distinct biomechanical types:
1. Low-Velocity Pistol or Rifle Wounds
Low-velocity projectiles (typically <1,000 feet/second) impart minimal kinetic energy to the surrounding tissues. The wounds of entry and exit are usually small, and the zone of soft tissue cavitation is negligible.
* Surgical Management: Extensive formal debridement is unnecessary. Treatment consists of local wound care, irrigation of the skin edges, and tetanus prophylaxis. The wounds should generally be left open to heal by secondary intention.
* Antibiotic Protocol: Infection rates are exceedingly low. A single dose of a long-acting intravenous cephalosporin (e.g., cefazolin) followed by a short course of oral antibiotics is highly effective. Dickson et al. demonstrated excellent outcomes (only 1 superficial infection in 44 fractures) using an outpatient protocol: 1g IV cefazolin in the ER, followed by 500mg oral cephalexin QID for 7 days, combined with local wound care and closed reduction/splinting.
* Intra-articular Exceptions: If a low-velocity bullet passes through "clean" skin into a joint, 1 to 2 days of IV antibiotics are recommended. If the bullet traverses contaminated viscera (bowel) or grossly contaminated clothing before entering the joint, a 1 to 2-week course of broad-spectrum antibiotics is required, alongside formal arthrotomy and joint irrigation.
2. High-Velocity Rifle Wounds
High-velocity projectiles (>2,000 feet/second) transfer massive kinetic energy, creating a temporary cavitational wave that stretches and tears tissues far beyond the actual bullet tract.
* Surgical Management: These injuries behave similarly to severe crush injuries or Gustilo Type III open fractures. They result in massive tissue necrosis, bone comminution, and devascularization. They mandate emergent, aggressive, and often serial surgical debridement in the operating room to remove all non-viable muscle, bone, and fascia.
3. Close-Range Shotgun Wounds
While shotgun pellets individually have low mass and velocity, a close-range blast delivers the entire kinetic energy of the payload into a concentrated area. This results in devastating soft tissue destruction, massive contamination (including the introduction of the plastic wadding into the wound), and severe bone loss, requiring aggressive surgical management akin to high-velocity injuries.
COMPARTMENT SYNDROME AND VASCULAR INJURY
Vascular injuries and acute compartment syndrome represent true orthopaedic emergencies. Tissue ischemia, if left untreated for 8 hours or more, results in irreversible myonecrosis and permanent peripheral nerve damage.
The diagnosis of compartment syndrome is primarily clinical, characterized by pain out of proportion to the injury, pain with passive stretch of the involved muscles, palpable tenseness of the compartment, and neurological deficits (late findings). However, in the polytraumatized, obtunded, or intubated patient, clinical examination is unreliable, necessitating invasive intra-compartmental pressure monitoring.
Clinical Pearl: Absolute compartment pressure values are less reliable than the differential pressure ($\Delta P$). Experimental and clinical data demonstrate that irreversible muscle damage occurs when the tissue pressure approaches the systemic diastolic blood pressure. A difference between the compartment tissue pressure and the diastolic blood pressure of 10 to 20 mm Hg (or $\Delta P < 30$ mm Hg in broader literature) is an absolute indication for immediate, four-compartment fasciotomy.
CONCLUSION
The management of orthopaedic trauma requires a profound understanding of systemic physiology, biomechanics, and evolving surgical evidence. By adhering to ATLS principles, utilizing Damage Control Orthopaedics in the physiologically unstable patient, and applying modern, evidence-based protocols for open fractures and ballistic injuries, the orthopaedic surgeon can significantly reduce mortality, minimize complications, and optimize long-term functional recovery. Continuous re-evaluation through tertiary surveys and judicious use of advanced imaging remain the cornerstones of preventing missed injuries and ensuring comprehensive patient care.
You Might Also Like