
Comprehensive Introduction and Patho-Epidemiology
The operative treatment of a forearm diaphyseal nonunion represents one of the most formidable challenges in orthopedic trauma reconstruction. The forearm must not be conceptualized merely as two parallel long bones, but rather as a highly complex, interconnected joint spanning from the radiocapitellar articulation proximally to the distal radioulnar joint (DRUJ) distally. The primary objective of surgical intervention extends far beyond the simple achievement of osseous union; it demands the meticulous restoration of the intricate biomechanical axis that governs pronation and supination. Failure to recognize the forearm as a dynamic, functional ring will inevitably result in profound, long-term disability, characterized by chronic pain, restricted range of motion, and early post-traumatic arthrosis.
By strict definition, a nonunion is a fracture that has failed to demonstrate radiographic or clinical progression of healing over a minimum of three consecutive months, typically assessed at the six-to-nine-month post-injury mark. While the advent of modern rigid internal fixation techniques—specifically dynamic compression plating—has reduced the incidence of forearm diaphyseal nonunions to approximately 2% for the radius and 4% for the ulna, these complications remain devastating when they occur. The surrounding anatomical landscape is densely packed with critical neurovascular structures, demanding an exhaustive understanding of surgical exposures and internervous planes to avoid iatrogenic morbidity during revision procedures.
Nonunions of the forearm diaphysis are broadly stratified into two distinct patho-biological categories, each dictating a fundamentally different reconstructive algorithm. Hypertrophic nonunions are characterized by abundant, exuberant callus formation, signaling a biologically active environment with a robust vascular supply. The primary etiology in these cases is mechanical instability—often the result of inadequate initial plate fixation, insufficient screw purchase, or premature weight-bearing. These represent less than 10% of forearm nonunions and typically require rigid stabilization with compression to achieve union. Conversely, atrophic nonunions, which constitute the vast majority of cases, exhibit a complete absence of callus formation. The biological machinery required for osteogenesis has stalled, usually secondary to severe initial trauma, extensive periosteal stripping, thermal necrosis from aggressive drilling, or underlying infection.

The pathogenesis of these nonunions is multifactorial, frequently stemming from technical errors during the index procedure. Insufficient fixation—defined as fewer than six cortices of screw purchase in the proximal or distal fragment—failure to achieve interfragmentary compression, or the use of an inappropriately short plate are common culprits. Furthermore, patient-specific comorbidities significantly amplify the risk profile. Nicotine use, poorly controlled diabetes mellitus, chronic corticosteroid administration, severe malnutrition, and end-stage renal disease severely compromise the microvascular environment necessary for bone healing. Once established, a forearm nonunion will not resolve spontaneously; it requires aggressive, meticulously planned surgical intervention to re-establish both mechanical stability and biological viability.
Detailed Surgical Anatomy and Biomechanics
A profound mastery of forearm osteology and biomechanics is the absolute prerequisite for successful nonunion reconstruction. The ulna serves as the relatively straight, stable axis around which the radius rotates. The radius, however, is characterized by a complex, three-dimensional geometry featuring distinct apex radial and apex dorsal curvatures. The maximum radial bow typically occurs at the mid-diaphysis, and restoring this precise curvature is paramount. Biomechanical studies have unequivocally demonstrated that even minor alterations in the magnitude or location of the radial bow will drastically impede pronation and supination. Furthermore, the functional integrity of the proximal radioulnar joint (PRUJ) and the DRUJ must be preserved or restored to allow for seamless rotation.

The interosseous membrane (IOM) is a critical, yet frequently underappreciated, anatomical structure in forearm mechanics. This stout fibrous sheet, particularly its central band, is responsible for longitudinal load transfer from the radius to the ulna and prevents proximal migration of the radius under axial loading. In the setting of a chronic nonunion, especially those associated with bone loss or significant shortening, the IOM often becomes contracted and fibrotic. Excessive stripping or iatrogenic injury to the IOM during surgical exposure can precipitate the formation of a radioulnar synostosis—a catastrophic complication that completely obliterates forearm rotation and is notoriously difficult to salvage.
Navigating the muscular intervals and neurovascular structures requires precise execution of established surgical approaches. The Volar Henry approach remains the undisputed workhorse for the majority of mid-to-distal radial nonunions. This approach exploits the internervous plane between the brachioradialis (innervated by the radial nerve) and the flexor carpi radialis (innervated by the median nerve). Deep dissection requires meticulous identification and protection of the radial artery, which courses superficially, and the median nerve, which lies deeper beneath the flexor digitorum superficialis. The flexor pollicis longus (FPL) and pronator teres must be carefully elevated off the anterior radius, preserving as much periosteal attachment as possible to maintain local vascularity.
For proximal radial nonunions, particularly in heavily muscled individuals, the Dorsal Thompson approach provides superior visualization. Utilizing the interval between the extensor carpi radialis brevis (ECRB) and the extensor digitorum communis (EDC), the surgeon must navigate the most perilous structure in the forearm: the posterior interosseous nerve (PIN). The PIN penetrates the supinator muscle and wraps around the radial neck; it must be visually identified and protected from excessive traction to prevent devastating motor deficits (finger and thumb drop). The ulnar approach, while technically less demanding due to the subcutaneous nature of the ulnar diaphysis, requires vigilance to protect the dorsal cutaneous branch of the ulnar nerve distally, injury to which results in symptomatic neuromas and dorsal sensory loss.
Exhaustive Indications and Contraindications
The decision to proceed with operative reconstruction of a forearm nonunion requires a comprehensive evaluation of the patient's symptoms, functional demands, radiographic findings, and overall physiological status. The primary, absolute indication for surgery is a symptomatic nonunion characterized by localized pain, gross instability, and progressive functional decline. In the forearm, even asymptomatic nonunions are generally considered an indication for surgery, as the chronic mechanical failure of the radius or ulna will inevitably lead to hardware fatigue, plate breakage, and progressive deformity. Furthermore, shortening of either bone disrupts the delicate kinematics of the DRUJ and PRUJ, leading to subluxation, chronic wrist or elbow pain, and accelerated degenerative arthrosis.
Relative indications include delayed unions that demonstrate progressive hardware failure, such as screw back-out or plate bending, prior to the strict six-month definition of a nonunion. In these scenarios, waiting for arbitrary chronological milestones is detrimental, as the mechanical environment is already failing. Additionally, nonunions associated with significant angular or rotational deformities that impede the patient's activities of daily living or occupational requirements warrant early intervention. The surgeon must carefully weigh the risks of surgery against the anticipated functional gains, particularly in elderly, low-demand patients who may tolerate a stable, fibrous nonunion with minimal discomfort.
Contraindications to immediate definitive reconstruction must be rigorously respected to avoid disastrous outcomes. Active, untreated deep infection is an absolute contraindication to single-stage internal fixation and bone grafting. In the presence of purulence, draining sinus tracts, or osteomyelitis, the surgeon must pivot to a staged approach: radical debridement, hardware explantation, placement of an antibiotic-impregnated cement spacer (such as the Masquelet technique), and temporary stabilization with an external fixator. Definitive reconstruction is delayed until all clinical and serological markers of infection have normalized. Severe medical comorbidities that preclude safe administration of general or regional anesthesia also represent absolute contraindications.
Patient optimization is a critical, non-negotiable component of the preoperative phase. Modifiable risk factors must be aggressively addressed before any elective reconstructive procedure is undertaken. Smoking cessation is paramount, as nicotine profoundly inhibits microvascular perfusion and osteogenesis; ideally, patients should be nicotine-free for at least six weeks preoperatively and postoperatively. Glycemic control in diabetic patients must be optimized (target HbA1c < 7.0%) to mitigate infection risk and promote soft tissue healing. Nutritional deficiencies, particularly low serum albumin or vitamin D levels, should be corrected to ensure the patient possesses the physiological reserves necessary to mount a robust healing response.
| Category | Indications for Operative Reconstruction | Contraindications for Operative Reconstruction |
|---|---|---|
| Clinical | Intractable pain at the fracture site; gross clinical instability; loss of pronation/supination. | Active, untreated deep infection; severe, uncorrectable medical comorbidities precluding anesthesia. |
| Radiographic | Absence of bridging callus >6 months; hardware failure (broken plate/screws); progressive angular deformity. | Active osteomyelitis requiring staged debridement first; inadequate bone stock precluding any fixation. |
| Biomechanical | Alteration of radial bow; DRUJ/PRUJ subluxation secondary to diaphyseal shortening. | Critical soft tissue compromise requiring flap coverage prior to definitive internal fixation. |
| Patient Factors | High-demand functional requirements; occupational necessity for upper extremity strength. | Active smoking or uncontrolled diabetes (relative contraindications requiring preoperative optimization). |
Pre-Operative Planning, Templating, and Patient Positioning
Preoperative planning for forearm nonunion reconstruction is an exhaustive process that dictates the intraoperative workflow and ultimately determines the success of the procedure. The foundation of this planning relies on high-quality, orthogonal radiographic imaging. Standard anteroposterior (AP) and lateral views of the entire injured forearm, encompassing both the elbow and wrist joints, are mandatory. Crucially, identical comparative views of the contralateral, uninjured forearm must be obtained. These contralateral images serve as the patient's individualized anatomical blueprint, allowing the surgeon to precisely template the required plate length, calculate the degree of necessary lengthening to restore ulnar variance, and map the exact apex and magnitude of the radial bow.

Advanced imaging is frequently required to fully characterize the nonunion. Computed Tomography (CT) scanning, utilizing metal artifact reduction sequence (MARS) protocols to suppress scatter from existing hardware, is invaluable. CT provides high-resolution, three-dimensional data regarding the size of the osseous defect, the presence of necrotic bone segments, the integrity of the surrounding cortices, and the potential existence of an occult radioulnar synostosis. Furthermore, a rigorous infection workup is mandatory for all nonunions, particularly those with a history of open trauma or prior surgical interventions. This includes a complete blood count (CBC), erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP). If suspicion remains high despite normal serology, advanced nuclear medicine studies, such as an indium-111–labeled leukocyte scan, may be indicated to rule out indolent infection.
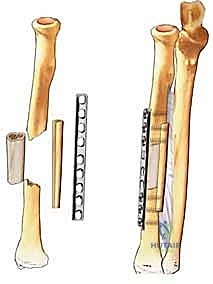
Hardware and bone graft selection must be finalized prior to entering the operating theater. For diaphyseal forearm nonunions, 3.5mm dynamic compression plates (DCP), limited-contact dynamic compression plates (LC-DCP), or locking compression plates (LCP) are the gold standards. The fundamental biomechanical rule is to achieve a minimum of six to eight cortices of secure screw purchase in healthy bone both proximal and distal to the nonunion site. This frequently necessitates the use of longer plates (e.g., 8-hole to 12-hole plates) than those utilized in acute fracture management. For atrophic nonunions, autologous bone grafting is absolutely essential. The surgeon must preoperatively determine whether a structural graft (e.g., tricortical iliac crest) is required to span a segmental defect, or if cancellous autograft (e.g., from the anterior iliac crest or proximal tibia) will suffice to stimulate osteogenesis.
Patient positioning and operating room setup must be meticulously orchestrated to facilitate seamless surgical flow. The patient is positioned supine on the operating table, with the operative extremity extended onto a fully radiolucent hand table. This setup is critical to allow unencumbered, multi-planar access for the standard C-arm fluoroscopy unit; mini C-arms provide an insufficient field of view and should not be used. A non-sterile pneumatic tourniquet is applied high on the brachium to ensure a bloodless surgical field, but it must be positioned to allow full, unrestricted flexion and extension of the elbow joint for intraoperative assessment. The selected autograft harvest site—most commonly the ipsilateral anterior iliac crest—is simultaneously prepped and draped into the sterile field to allow for a two-team approach if necessary.
Step-by-Step Surgical Approach and Fixation Technique
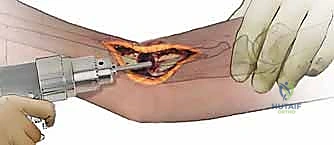
The intraoperative execution of a forearm nonunion reconstruction demands uncompromising technical precision and a systematic, step-by-step approach. Prior to making the skin incision, a comprehensive examination under anesthesia is performed to assess the baseline range of motion of the elbow, wrist, and forearm rotation. This establishes a critical benchmark against which the post-fixation kinematics will be judged. Following exsanguination of the limb, the tourniquet is inflated to 250 mmHg. The surgical approach—whether the Volar Henry, Dorsal Thompson, or direct ulnar—is executed with meticulous care, often navigating through dense, scarred tissue beds from prior surgeries. Previous incisions should be utilized when possible, excising the old scar tissue to promote optimal wound healing.
The first major intraoperative hurdle is the safe and complete removal of existing hardware. In the setting of a nonunion, screws are frequently broken, cold-welded to the plate, or stripped. The surgical team must have a comprehensive broken hardware removal set immediately available on the back table, including carbide drill bits, reverse-threaded extraction screws (easy-outs), hollow reamers, and metal-cutting burrs. Aggressive prying or levering of the plate must be strictly avoided, as this can easily cause iatrogenic fractures in the already compromised, osteopenic bone. Once the hardware is explanted, the nonunion site is fully exposed.
Preparation of the nonunion site is arguably the most critical biological step of the procedure. The fibrous pseudarthrosis tissue must be radically excised using a combination of rongeurs and sharp curettes until healthy, bleeding bone is encountered. The sclerotic bone ends are meticulously debrided. The medullary canal, which is typically sealed off by dense sclerotic bone in atrophic nonunions, must be aggressively re-opened. This is achieved by drilling the intramedullary canals proximally and distally with a 2.0mm or 2.5mm drill bit until punctate bleeding—the so-called "paprika sign"—is clearly visualized. The cortical ends are then "shingled" or petaled with a sharp osteotome to maximize the surface area of bleeding bone available for graft incorporation.
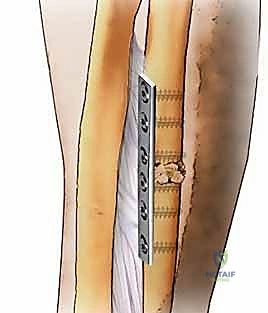
Following biological preparation, the focus shifts to mechanical reconstruction. The bone ends are mobilized, and normal anatomical length, alignment, and rotation are restored. Provisional fixation is achieved using reduction forceps. The pre-templated 3.5mm plate is then applied. In hypertrophic nonunions, rigid compression plating is the primary goal; an articulated tension device can be utilized to generate massive interfragmentary compression. In atrophic nonunions, the plate functions as a bridge or neutralization plate, and compression must not be achieved at the expense of shortening the bone.
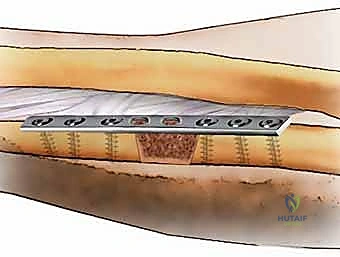
Once stable fixation is achieved with a minimum of six cortices proximal and distal, copious amounts of autologous cancellous bone graft are meticulously packed into and around the defect, ensuring complete coverage of the nonunion site while carefully avoiding spillage into the interosseous space, which could precipitate a synostosis. Before closure, the tourniquet is deflated, meticulous hemostasis is obtained, and the forearm is taken through a full, unhindered range of pronation and supination to confirm restoration of normal kinematics and DRUJ stability.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique and comprehensive preoperative planning, complications following forearm nonunion reconstruction remain a significant clinical reality. The surgeon must be prepared to rapidly identify and manage these adverse events to prevent irreversible functional loss. Deep postoperative infection is among the most devastating complications, occurring in approximately 2% to 5% of revision cases. Early superficial infections may be managed with aggressive oral or intravenous antibiotic therapy, but deep infections extending to the hardware necessitate prompt operative intervention. The standard protocol involves emergent irrigation and debridement, acquisition of deep tissue cultures, and the initiation of culture-directed intravenous antibiotics. If the fixation remains rigidly stable, the hardware may be retained to allow for osseous union; however, if the hardware is loose or the infection is recalcitrant, explantation and conversion to an external fixator are mandatory.
Neurovascular injuries, while relatively uncommon (1% to 3% incidence), carry profound medicolegal and functional implications. The posterior interosseous nerve (PIN) is highly vulnerable during the Dorsal Thompson approach to the proximal radius. The vast majority of these injuries are traction neurapraxias secondary to aggressive retraction of the supinator muscle and typically resolve spontaneously over 3 to 6 months. Superficial radial nerve injuries during the Volar Henry approach or dorsal cutaneous ulnar nerve injuries during ulnar exposures often result in exquisitely painful neuromas. If a nerve is known to be sharply transected intraoperatively, immediate microsurgical primary repair or nerve grafting is indicated. Vascular injuries, particularly to the radial artery, require immediate consultation with a vascular or microvascular surgeon for primary repair or interposition grafting to prevent ischemic contracture.
Radioulnar synostosis is a catastrophic complication characterized by the formation of a solid osseous bridge across the interosseous space, resulting in a complete, rigid loss of forearm pronation and supination. Risk factors include massive initial trauma, severe head injuries, and technical errors such as violating the interosseous membrane or allowing bone graft to spill into the interosseous space. The incidence ranges from 1% to 6% in complex trauma. Management is exceptionally difficult; early excision is universally associated with massive recurrence. The current standard of care dictates waiting a minimum of 6 to 12 months for the heterotopic bone to fully mature and for inflammatory markers to normalize before attempting surgical excision, often combined with the interposition of synthetic membranes or vascularized fat flaps to prevent recurrence.
Persistent or recalcitrant nonunion, despite adequate revision plating and autografting, represents the ultimate failure of the reconstructive effort. In these rare, limb-threatening scenarios, salvage procedures must be employed. For massive segmental defects lacking biological viability, a free vascularized fibular graft (FVFG) offers the introduction of structurally sound, living bone capable of rapid incorporation. Alternatively, the induced membrane (Masquelet) technique can be utilized for significant bone gaps. In the most extreme, unsalvageable cases where the DRUJ or PRUJ are completely destroyed and multiple reconstructive attempts have failed, the creation of a one-bone forearm (radioulnar synostosis creation) may be the only remaining option to provide the patient with a stable, albeit non-rotating, functional limb.
| Complication | Estimated Incidence | Primary Etiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Deep Infection | 2% - 5% | Poor soft tissue envelope; prolonged operative time; prior open fracture. | I&D, culture-directed IV antibiotics. Retain stable hardware; explant loose hardware. |
| PIN Palsy | 1% - 3% | Excessive traction on supinator during Dorsal Thompson approach. | Observation (most are neurapraxias resolving in 3-6 mos). EMG at 3 months if no recovery. |
| Radioulnar Synostosis | 1% - 6% | IOM violation; bone graft spillage into interosseous space; severe head trauma. | Delayed excision (6-12 months post-op) with interposition graft (fat/synthetic membrane). |
| Recalcitrant Nonunion | < 5% | Persistent avascularity; inadequate mechanical stability; patient non-compliance. | Vascularized fibular graft; Masquelet technique; One-bone forearm salvage. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation of a reconstructed forearm nonunion is a delicate, highly individualized balancing act. The surgeon and physical therapist must constantly negotiate the competing demands of protecting the fragile osteosynthesis construct while initiating early motion to prevent debilitating joint stiffness and soft tissue contractures. The immediate postoperative phase (Weeks 0-2) prioritizes wound healing, strict edema control, and pain management. The patient is typically placed in a bulky, well-padded posterior splint or a sugar-tong splint, immobilizing the wrist and elbow to minimize stress on the plate-bone interface. However, immediate, aggressive active range of motion of the digits and shoulder is mandatory to prevent collateral stiffness and promote venous and lymphatic return.
The early healing phase (Weeks 2-6) marks a critical transition. At the two-week mark, sutures are removed, and the rigid splint is typically transitioned to a custom-molded, removable thermoplastic functional brace. Under the strict supervision of a certified hand therapist, the patient initiates gentle, active, and active-assisted range of motion exercises for the elbow and wrist, specifically targeting pronation and supination. Passive stretching and any form of weight-bearing or lifting are strictly prohibited during this phase, as the bone graft is undergoing the initial, fragile stages of vascularization and creeping substitution. The functional brace must be worn at all times except during directed therapy sessions and hygiene.
The consolidation phase (Weeks 6-12) is guided entirely by radiographic progression. Serial orthogonal radiographs are scrutinized for the presence of bridging trabecular bone and the obliteration of the nonunion line. Once early clinical and radiographic union is confirmed, the functional brace is gradually weaned. The rehabilitation focus shifts toward progressive strengthening, utilizing light resistance bands and isometric exercises. Proprioceptive training and neuromuscular re-education are integrated to restore the dynamic stability of the forearm musculature. Heavy lifting, impact activities, and torsional loading remain restricted.
The return to function phase (Months 3-6 and beyond) aims to restore the patient to their pre-injury baseline. As the bone fully consolidates and remodels, aggressive strengthening and work-hardening programs are initiated. Patients are gradually cleared to return to heavy manual labor or contact sports, typically between 4 and 6 months postoperatively, contingent upon absolute radiographic union and symmetric strength compared to the contralateral limb. Routine hardware removal is strongly discouraged in the forearm due to the high risk of iatrogenic nerve injury and the well-documented risk of refract
Detailed Chapters & Topics
Dive deeper into specialized chapters regarding operative-treatment-of-radius-and-ulna-diaphyseal-nonunions