Mastering Iliopsoas and Adductor Release: A Comprehensive Intraoperative Guide
Key Takeaway
Join us in the OR for an immersive masterclass on iliopsoas and adductor release. We'll meticulously cover comprehensive surgical anatomy, crucial preoperative planning, and granular, real-time intraoperative execution. Learn precise dissection techniques, instrument handling, and critical neurovascular precautions. This guide also details essential pearls, pitfalls, and comprehensive postoperative management to optimize outcomes for hip contracture patients.
Welcome, colleagues and fellows, to the operating theater. Today, we are addressing a common yet critical issue in the surgical management of neuromuscular conditions: hip flexion and adduction contractures. Our focus will be on the precise, evidence-based techniques for iliopsoas and adductor lengthening. This procedure, while seemingly straightforward in its fundamental goals, demands an intimate understanding of regional anatomy, meticulous surgical execution, and a profound appreciation for neuromuscular biomechanics to restore functional hip kinematics and prevent catastrophic long-term complications such as paralytic hip subluxation and dislocation.
Comprehensive Introduction and Patho-Epidemiology
Musculotendinous length in the developing pediatric skeleton is a dynamic, highly regulated entity, adapting in response to normal osteogenesis and the physiological stretch imparted by typical childhood activities and weight-bearing. In neuromuscular conditions, most notably cerebral palsy (CP) and myelodysplasia (spina bifida), this delicate physiological balance is severely disrupted. The combination of disuse, profound muscular imbalance, and upper motor neuron spasticity leads to a catastrophic failure of sarcomere addition at the musculotendinous junction. Consequently, the muscle belly fails to elongate in tandem with the rapidly growing femur and pelvis, resulting in rigid, fibrotic contractures.
These contractures are not merely a functional nuisance; they profoundly and negatively impact a child's mobility, seating tolerance, perineal hygiene, and overall quality of life. A hip flexion contracture, which can initially be insidious and challenging to detect due to compensatory mechanisms, severely limits functional hip extension during the terminal stance phase of gait. This restriction inevitably shortens step length and induces obligate compensatory movements, most notably excessive anterior pelvic tilt and secondary lumbar hyperlordosis. Adductor contractures, while frequently and correctly blamed for a scissoring gait pattern, more commonly contribute to this pathological pattern in conjunction with concomitant hip and knee flexion contractures, as well as internal hip malrotation driven by unremitting, excessive femoral anteversion.
In severe, persistent cases—particularly in patients classified as Gross Motor Function Classification System (GMFCS) levels IV and V, or those with L2/L3 level myelodysplasia—the unyielding muscular imbalance is devastating. Innervated, spastic hip flexors and adductors overpower weak or paralyzed abductors and extensors. This dynamic imbalance exerts a relentless lateral and superior sheer force on the developing proximal femur, predisposing the hip to progressive subluxation, acetabular dysplasia, and ultimately, irreversible paralytic hip dislocation. Longstanding dysplasia and dislocation invariably lead to painful degenerative arthrosis, severe pelvic obliquity, and an inability to maintain a seated posture. Our primary objective today is to intervene strategically with precise soft-tissue releases to mitigate these devastating biomechanical consequences and preserve the integrity of the hip joint.
Detailed Surgical Anatomy and Biomechanics
Before we make any incision, a comprehensive, three-dimensional understanding of the regional anatomy is absolutely paramount. The anterior and medial compartments of the hip and thigh represent a surgical field where millimeters matter, and an anatomical oversight can result in severe, irreversible iatrogenic neurovascular injury.
The Iliopsoas Complex and Anterior Hip Anatomy
The iliopsoas, functioning as the primary flexor of the hip joint, is a composite musculotendinous unit comprised of the psoas major and the iliacus muscles. Understanding their distinct origins and convergence is critical for selecting the appropriate level of surgical release.
* Psoas Major: This robust muscle originates from the transverse processes of the lumbar vertebrae (T12-L5), as well as the lateral aspects of the vertebral bodies and their intervening intervertebral discs. Its fleshy muscle belly descends retroperitoneally over the sacral ala into the true pelvis. As it approaches the pelvic brim, specifically at the level of the superior pubic ramus and the iliopectineal eminence, a distinct, dense intramuscular tendon begins to coalesce on its posterior aspect.
- Iliacus: Originating broadly from the superior two-thirds of the concave iliac fossa, the iliacus muscle belly lies immediately lateral and superficial to the psoas major within the pelvic basin. Unlike the psoas, the iliacus remains predominantly muscular as it crosses the pelvic brim.
- Common Tendon and Insertion: Distal to the pelvic brim, the psoas tendon and the muscular fibers of the iliacus converge intimately to form a common musculotendinous unit that inserts firmly onto the lesser trochanter of the proximal medial femur.
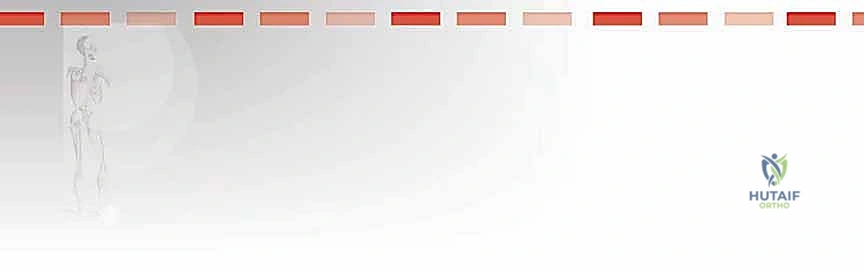
- Neurovascular Relationships: The anterior surgical approach to the iliopsoas is fraught with critical neurovascular adjacencies. The femoral neurovascular bundle—comprising the femoral nerve, femoral artery, and femoral vein (arranged lateral to medial)—lies strictly superficial and anterior to the iliacus muscle belly and the psoas tendon as they pass beneath the inguinal ligament.

Our preferred surgical approach at the pelvic brim specifically utilizes the deep, avascular tissue plane located underneath (lateral and deep to) the iliacus muscle belly. This strategic maneuver allows the surgeon to retract the entire iliacus muscle mass anteriorly and medially. By doing so, the iliacus acts as a robust, natural physical shield, effectively protecting the superficial femoral neurovascular structures from inadvertent injury during the tenotomy.
Furthermore, the lateral femoral cutaneous nerve (LFCN), a purely sensory nerve providing innervation to the anterolateral thigh, typically crosses the surgical field obliquely. It most commonly courses just medial to the anterior superior iliac spine (ASIS) beneath the inguinal ligament. However, its anatomical course is notoriously variable; it may lie more medially or branch extensively. It must be actively sought, meticulously isolated, and gently retracted if visualized within the superficial dissection plane.
The Adductor Compartment and Medial Thigh
The adductor compartment of the thigh is comprised of a complex group of muscles crucial for hip adduction and, depending on the position of the hip, secondary flexion and extension.
* Adductor Longus: This muscle is our primary surgical target for the majority of ambulatory patients requiring adductor lengthening. It originates via a distinct, easily palpable, cord-like tendinous origin from the anterior surface of the pubic body, just inferior to the pubic crest.
* Gracilis: A long, superficial, strap-like muscle originating from the anterior half of the pubic symphysis and the superior half of the pubic arch. It possesses a broad muscular fascia rather than a distinct, localized tendon at its origin, and it inserts distally on the medial proximal tibia as part of the pes anserinus.
* Adductor Brevis: Situated deep to the adductor longus and superficial to the adductor magnus, it originates from the outer surface of the inferior pubic ramus. It has a predominantly muscular origin and inserts onto the proximal linea aspera.
* Adductor Magnus: The largest, most powerful, and most posterior muscle of the adductor group. It features dual origins from the ischial tuberosity (hamstring part) and the ischiopubic ramus (adductor part). It is rarely released in ambulatory patients to prevent debilitating excessive abduction and extension weakness.

- Obturator Nerve Branches: The obturator nerve provides the primary motor innervation to this compartment and dictates our planes of dissection.
- The anterior branch of the obturator nerve emerges from the obturator canal and descends precisely in the fascial interval deep to the adductor longus and superficial to the adductor brevis. This nerve must be identified and protected when isolating the adductor longus tendon.
- The posterior branch of the obturator nerve descends in the deeper fascial interval, deep to the adductor brevis and superficial to the adductor magnus. Careful, blunt dissection is absolutely essential to avoid devastating iatrogenic denervation of the adductor musculature.
Exhaustive Indications and Contraindications
The decision to proceed with operative intervention must be grounded in a rigorous assessment of the patient's functional status, neurological prognosis, and radiographic parameters. Prophylactic soft-tissue releases are the standard of care for the "hip at risk" in neuromuscular populations, but patient selection is paramount.
| Clinical Parameter | Indications for Surgical Release | Contraindications / Cautions |
|---|---|---|
| Neurological Tone | Severe spasticity causing dynamic contracture; progressive loss of ROM despite aggressive conservative management (Botox, bracing, PT). | Pure athetosis, dystonia, or profound hypotonia (high risk of unpredictable post-operative posture and severe weakness). |
| Radiographic Status | Reimers' Migration Percentage (MP) > 30% but < 50% (Hip at Risk); intact Shenton's line; minimal to no acetabular dysplasia. | MP > 50%, broken Shenton's line, severe coxa valga, or significant acetabular dysplasia (Requires concomitant bony osteotomies: VDRO/Pelvic). |
| Functional Status | Scissoring gait impeding ambulation; severe difficulty with perineal hygiene, diapering, or seating in non-ambulatory patients. | Lack of reliable post-operative rehabilitation support; medically unstable patient unable to tolerate general anesthesia. |
| Physical Exam | Hip abduction < 30 degrees in extension; Hip flexion contracture > 15-20 degrees severely altering gait kinematics. | Fixed, rigid bony deformities that cannot be corrected by soft-tissue release alone. |
It is crucial to emphasize that isolated soft-tissue releases are rarely successful in older children (typically > 8 years old) with established bony deformities. In such cases, soft-tissue procedures must be viewed as adjuncts to comprehensive bony reconstruction (Varus Derotational Osteotomy and Pelvic Osteotomy).
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the absolute cornerstone of a successful, complication-free outcome. This phase requires a synthesis of detailed clinical assessment, rigorous imaging review, and meticulous operating room setup.
Clinical and Radiographic Evaluation
Our preoperative assessment begins in the clinic with an exhaustive patient history and a highly specific physical examination.
* Range of Motion (ROM) Assessment: We meticulously assess hip flexion-extension and abduction-adduction ROM. Normal, efficient ambulation requires approximately 7 to 10 degrees of true hip extension beyond neutral during terminal stance. Even minor flexion contractures severely limit functional ROM, forcing compensatory anterior pelvic tilt. For abduction, while maximum abduction during the swing phase of walking is minimal, limited passive abduction ROM (< 30 degrees) is a major red flag for impending hip subluxation and compromises normal acetabular development.
* Differentiating Spasticity vs. Fixed Contracture: This distinction is the crux of surgical decision-making. In the awake patient, if a sudden "catch" and subsequent resistance are felt during rapid hip extension and abduction, spasticity (a velocity-dependent increase in muscle tone) is present. While spasticity precedes contracture, true fixed musculotendinous shortening will present as a hard, unyielding end-point regardless of the velocity of the stretch.
* Radiographic Evaluation: A high-quality, standardized supine anteroposterior (AP) pelvis radiograph is mandatory.
* We systematically evaluate for early signs of paralytic hip dysplasia: a break in Shenton's line, an increased acetabular index, coxa valga (increased neck-shaft angle), and incomplete femoral head coverage. The Reimers' Migration Percentage is calculated; an MP > 30% is widely considered the threshold for surgical intervention in CP.

* Severe, uncompensated hip flexion contractures force the pelvis into an extreme anterior tilt when the patient is positioned supine. This results in an "inlet view" appearance on the standard AP radiograph, characterized by the apparent obliteration or narrowing of the obturator foramina. This radiographic artifact is highly indicative of the severity of the flexion contracture.


Examination Under Anesthesia (EUA) and Patient Positioning
The Examination Under Anesthesia (EUA) is a non-negotiable, critical step immediately preceding the incision. Under deep general anesthesia and complete neuromuscular blockade, all dynamic hypertonicity and spasticity are completely abolished. This allows the surgical team to accurately differentiate between restricted range of motion due to high muscle tone and a true, fixed musculotendinous contracture. We perform a full, unrestricted hip ROM assessment, specifically employing the Thomas test to unmask true hip flexion contractures, ensuring we are not misled by concurrent, compensatory lumbar lordosis or knee flexion contractures.
The patient is positioned supine on a standard radiolucent operating table. Ensure the patient is perfectly centered, with generous padding applied to all bony prominences to prevent perioperative pressure neuropraxias.
Crucially, the affected lower extremity—and almost universally, both lower extremities—must be prepped and draped completely free. This extensive draping is critical to allow full, unimpeded range of motion of the hip and knee joints during the procedure. The surgeon must be able to fluidly flex, extend, abduct, and internally/externally rotate the hip to dynamically assess the adequacy of the soft-tissue releases in real-time. Care must be taken with the sterile drapes to ensure wide access to the anterior pelvis, extending proximally above the ASIS for the iliopsoas release, and medially along the proximal inner thigh to the perineal crease for the adductor release.
Step-by-Step Surgical Approach and Execution Technique
Alright, fellows, let us proceed to the surgical execution. We will commence with the iliopsoas lengthening at the pelvic brim, immediately followed by the adductor release. Performing the psoas release first often reduces the tension on the adductors, facilitating a more accurate assessment of adductor tightness.
Iliopsoas Lengthening at the Pelvic Brim
Our primary objective here is a controlled, precise intramuscular lengthening of the psoas tendon directly at the pelvic brim. This specific technique preserves the muscular continuity of the iliacus, thereby maintaining essential hip flexion power for swing-phase clearance while gaining the crucial hip extension required for a normalized stance phase. This approach strictly minimizes the risk of catastrophic over-lengthening and subsequent debilitating weakness, which is of paramount importance in ambulatory patients.
- Incision and Superficial Dissection: Using a sterile surgical marker, we delineate our incision. The preferred approach utilizes a 3 to 4 cm oblique incision positioned approximately one fingerbreadth distal to the anterior superior iliac spine (ASIS) and extending inferomedially, running parallel to the inguinal ligament.

We incise the skin and subcutaneous tissues sharply down to the superficial fascia (Scarpa's fascia). Meticulous hemostasis is maintained with electrocautery. We carefully divide the superficial fascia in line with the skin incision. At this juncture, extreme vigilance is required to identify and mobilize the Lateral Femoral Cutaneous Nerve (LFCN), which typically traverses this plane. If identified, it is gently retracted medially or laterally, depending on its specific anatomical variant, to prevent painful post-operative neuromas.

- Deep Dissection and Interval Identification: We identify the fascial interval between the sartorius muscle (laterally) and the tensor fasciae latae (medially), or more commonly for this specific proximal approach, we incise the fascia lata directly over the interval between the sartorius and the rectus femoris. We bluntly retract the sartorius laterally and the rectus femoris medially.
Deep to these structures, the glistening fascia overlying the iliacus muscle belly comes into view. We do not dissect medial to the iliacus at this level to avoid the femoral nerve. Instead, we develop the plane strictly lateral to the iliacus muscle belly, sweeping it medially off the inner table of the ilium.

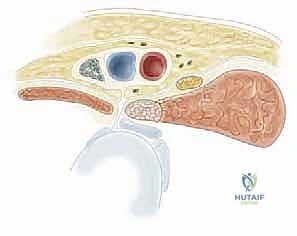
- Fractional Lengthening of the Psoas Tendon: By placing a blunt retractor (such as a Taylor or a deep right-angle retractor) over the pelvic brim and retracting the entire iliacus muscle belly medially, we simultaneously protect the femoral neurovascular bundle that lies safely superficial to our retractor.
We then longitudinally incise the epimysium of the iliacus. By bluntly spreading the muscle fibers of the iliacus, the dense, white, cord-like tendon of the psoas major is identified embedded within the posterior aspect of the muscle belly. Using a right-angle clamp to isolate the tendon, we perform a transverse tenotomy of the psoas tendon only, leaving the overlying and interspersed iliacus muscle fibers entirely intact.
Upon division of the tendon, the hip is gently extended, and the cut ends of the tendon will be felt and seen to separate, achieving a fractional lengthening while preserving continuous muscle power.
Adductor Tenotomy and Gracilis Release
Following the psoas lengthening, we shift our attention to the medial compartment. The goal is to release the tight adductor longus and, if necessary, the gracilis, to restore adequate abduction while avoiding over-release that could lead to an abduction contracture.
- Incision and Isolation: The hip is placed in a position of flexion, abduction, and external rotation (the "frog-leg" position) to place the adductor musculature under maximal tension. A 2 to 3 cm longitudinal or transverse incision is made directly over the palpable, taut origin of the adductor longus tendon, just distal to the pubic crease.

Subcutaneous
Clinical & Radiographic Imaging Archive








