Mastering Iliac Crest Bone Graft Harvest: An Intraoperative Masterclass
Key Takeaway
Join us in the OR for a detailed masterclass on iliac crest bone graft harvesting. We'll meticulously cover surgical anatomy, patient positioning, and step-by-step intraoperative execution for both anterior and posterior approaches. Learn to navigate neurovascular risks, utilize precise instrumentation, and manage potential complications, ensuring optimal outcomes for your spinal fusion patients. This guide is designed for fellows seeking to master this essential technique.
Comprehensive Introduction and Patho-Epidemiology
Autogenous iliac crest bone graft (ICBG) remains the undisputed gold standard in orthopedic and neurological spine surgery for achieving robust, predictable arthrodesis. Despite the rapid proliferation of synthetic bone void fillers, demineralized bone matrices (DBMs), allografts, and recombinant human bone morphogenetic proteins (rhBMPs), no single alternative has fully replicated the complete biological profile of fresh autograft. The intrinsic superiority of ICBG lies in its unique triad of bone healing properties: it is simultaneously osteoconductive, osteoinductive, and osteogenic. The three-dimensional trabecular scaffold provides an ideal osteoconductive matrix for vascular ingrowth and cellular migration. The extracellular matrix harbors osteoinductive growth factors, including endogenous BMPs, which stimulate the differentiation of mesenchymal stem cells (MSCs) into the osteoblastic lineage. Most critically, fresh autograft delivers living, immunocompatible osteoprogenitor cells and mature osteoblasts directly to the fusion site, fulfilling the osteogenic requirement that all synthetic and processed allogeneic options inherently lack.
The patho-epidemiology of spinal non-union (pseudoarthrosis) underscores the continued necessity of mastering the ICBG harvest. Patient-specific risk factors, such as advanced age, chronic corticosteroid use, osteoporosis, diabetes mellitus, and tobacco use, severely compromise the host's innate healing capacity. In these biologically hostile environments, or in the context of revision surgery for established pseudoarthrosis, relying solely on allograft or synthetics significantly increases the risk of clinical failure. Furthermore, the structural demands of specific procedures, such as anterior cervical corpectomy and fusion (ACCF) or complex lumbo-pelvic reconstructions, often necessitate a graft that can withstand significant axial loads while simultaneously promoting creeping substitution. The tricortical anterior iliac crest graft provides this exact combination of immediate biomechanical stability and long-term biological incorporation.
While the biological and structural benefits of ICBG are unparalleled, the procedure is not without its drawbacks. The primary deterrent to its universal application is donor site morbidity. Historically, complication rates associated with ICBG harvest have been reported to range widely, with acute pain, hematoma, infection, and nerve injury being the most frequently cited issues. Chronic donor site pain remains a significant concern, occasionally superseding the pain from the primary spinal pathology. Consequently, the contemporary spine surgeon must approach the iliac crest not merely as a generic donor site, but as a distinct surgical field requiring meticulous preoperative planning, profound anatomical knowledge, and exacting intraoperative technique. Mastering this procedure minimizes morbidity while maximizing the biological yield, ensuring that the patient receives the optimal environment for spinal fusion without enduring unnecessary iatrogenic harm.
Detailed Surgical Anatomy and Biomechanics
Before a scalpel is ever passed, a profound, three-dimensional understanding of pelvic anatomy is non-negotiable. The ilium, the largest of the three bones comprising the innominate bone, offers two primary harvest sites: the anterior and posterior crests. Each site presents unique biomechanical properties and distinct neurovascular hazards. The surgeon must respect the intricate muscular attachments and the paths of regional nerves and vessels to execute a safe harvest.
Anterior Iliac Crest Anatomy
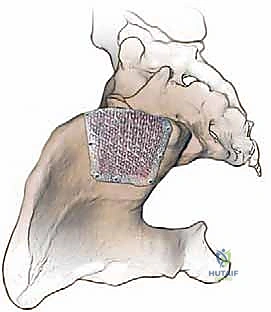
The anterior ilium presents a concave anterosuperior surface, providing an excellent source of structural, tricortical bone. The thickest portion of the anterior iliac crest, known as the iliac tubercle, is typically located 2 to 3 centimeters posterior to the anterior superior iliac spine (ASIS). This specific anatomical zone is the primary target for harvesting structural grafts, as it offers the optimal width and cortical density required to withstand axial compression in interbody fusions. Harvesting too far anteriorly compromises the ASIS, increasing the risk of avulsion fractures, while harvesting too far posteriorly yields thinner bone that may lack the necessary structural integrity.

The neurovascular anatomy of the anterior ilium is complex and highly variable, demanding meticulous surgical technique. The most critical structure at risk is the Lateral Femoral Cutaneous Nerve (LFCN). This purely sensory nerve typically courses medial to the ASIS, descending beneath the inguinal ligament to supply sensation to the anterolateral thigh. However, anatomical studies demonstrate extreme variability; in a significant minority of patients, the LFCN can cross directly over or even lateral to the ASIS. Iatrogenic injury to this nerve, either via direct transection, traction, or compression from retractors, results in meralgia paresthetica—a highly distressing condition characterized by burning pain, tingling, and numbness along the lateral thigh.

Medially, the abdominal musculature (external oblique, internal oblique, and transversus abdominis) attaches to the inner lip of the iliac crest. Deep to these attachments lie the ilioinguinal and iliohypogastric nerves. These sensory nerves are particularly vulnerable to compression when rigid retractors are placed aggressively against the inner table of the ilium. Lateral to the crest, the tensor fascia latae, gluteus medius, and gluteus minimus originate, innervated by the superior gluteal nerve. The incision directly over the crest is considered an internervous plane regarding major motor function, but the periosteal elevation must be precise to avoid unnecessary muscular trauma and subsequent gait disturbances.
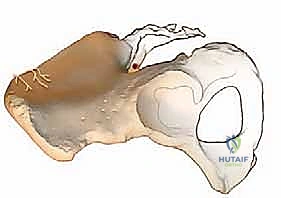
Posterior Iliac Crest Anatomy
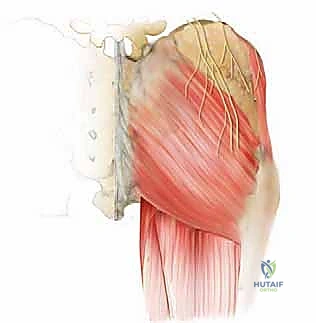
The posterior iliac crest is the preferred site for harvesting large volumes of non-structural, cancellous autograft, frequently utilized in posterolateral spinal fusions. The crest here is substantially thicker than its anterior counterpart, ranging from 14 to 17 millimeters in width, and contains a rich reservoir of osteoprogenitor-dense cancellous bone. The posterior superior iliac spine (PSIS) serves as the primary palpable landmark, often identifiable by a distinct skin dimple in the superomedial gluteal region. Harvests are typically initiated just lateral to the PSIS and can extend anteriorly along the crest.
The neurovascular risks in the posterior approach are distinct and potentially more severe than those encountered anteriorly. The superior cluneal nerves, which provide sensory innervation to the superior buttocks, cross the posterior iliac crest approximately 7 to 8 centimeters lateral (anterior) to the PSIS. Incisions or deep dissections extending into this zone place these nerves at high risk of transection or entrapment, leading to painful neuromas and chronic postoperative pain. Consequently, surgical exposure must be carefully restricted to the safe zone medial to these nerve branches.
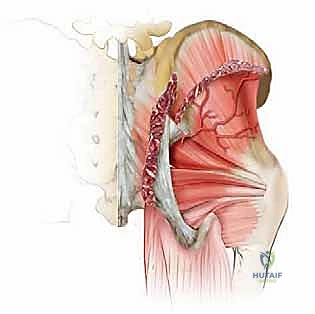
Deep to the posterior ilium lies the greater sciatic notch, a critical anatomical boundary. The superior gluteal artery, a major branch of the internal iliac artery, exits the pelvis through the uppermost portion of the greater sciatic notch. If dissection or osteotome placement extends too far inferiorly and breaches the notch, this artery can be lacerated. An injured superior gluteal artery can rapidly retract into the true pelvis, resulting in catastrophic, life-threatening hemorrhage that is notoriously difficult to control from a posterior approach. Furthermore, the sciatic nerve lies deep within this notch; while less commonly injured than the artery, deep, uncontrolled plunging with surgical instruments can result in devastating motor and sensory deficits.
Exhaustive Indications and Contraindications
The decision to harvest iliac crest bone graft must be heavily individualized, balancing the biological requirements of the primary procedure against the patient's anatomical suitability and tolerance for potential donor site morbidity. The choice between anterior and posterior harvest is dictated primarily by the type of bone required: structural (tricortical) versus non-structural (cancellous slurry).
Anterior ICBG is strictly indicated when immediate biomechanical support is required in conjunction with biological fusion. The classic indication is the anterior cervical corpectomy and fusion (ACCF), where a tricortical strut is impacted between the remaining vertebral bodies to restore anterior column height and lordosis. It is also utilized in complex maxillofacial reconstructions and certain foot and ankle arthrodeses. Posterior ICBG is indicated when massive volumes of osteogenic material are needed to pack posterolateral gutters or interbody cages, such as in multi-level lumbar fusions, deformity corrections, or the treatment of recalcitrant pseudoarthroses.
Contraindications to ICBG harvest can be absolute or relative, depending on the severity of the underlying condition. Severe osteoporosis is a primary concern; osteoporotic bone lacks both the structural integrity required for tricortical grafts and the dense cancellous volume desired from posterior harvests, rendering the procedure high-risk with low reward. Previous harvests from the same site significantly alter the local anatomy, obliterate the medullary cavity, and increase the risk of nerve injury due to epidural scarring, making repeat harvesting relatively contraindicated. Local infection or compromised soft tissue envelopes over the iliac crest are absolute contraindications to prevent the seeding of pathogens into the deep pelvic spaces.
| Category | Anterior Iliac Crest Harvest | Posterior Iliac Crest Harvest |
|---|---|---|
| Primary Indications | Cervical/Lumbar structural interbody fusion, Corpectomy strut grafts, Maxillofacial reconstruction, Joint arthrodesis requiring structural support. | Multi-level posterolateral lumbar fusions, Deformity correction (scoliosis/kyphosis), Pseudoarthrosis revision, Filling large bone cysts/defects. |
| Graft Type Yielded | Tricortical structural struts, Corticocancellous blocks, Limited cancellous bone. | Massive volume cancellous bone, Corticocancellous matchsticks/strips. |
| Absolute Contraindications | Active local infection, Severe pelvic instability/fracture, Prior extensive harvest obliterating the iliac tubercle. | Active local infection, Prior extensive harvest at the PSIS, Anatomical anomalies of the sciatic notch. |
| Relative Contraindications | Severe osteoporosis, Morbid obesity (complicates exposure/healing), Previous inguinal hernia repair (altered medial anatomy). | Severe osteoporosis, Bleeding diatheses, Chronic sacroiliac joint dysfunction. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the cornerstone of a successful and low-morbidity ICBG harvest. The surgeon must not approach the ilium blindly; advanced imaging should be utilized to assess the available bone stock. Preoperative computed tomography (CT) scans of the pelvis, often available if the patient underwent a full trauma workup or specific spinal imaging, are invaluable. The CT scan allows the surgeon to measure the cortical thickness of the anterior iliac tubercle or the cancellous volume of the posterior ilium, ensuring the targeted site can yield the required graft dimensions.
For anterior structural grafts, templating is highly recommended. By utilizing lateral cervical or lumbar radiographs, the surgeon can estimate the required height and depth of the tricortical strut needed for an interbody fusion or corpectomy. These dimensions should be noted and directly translated to the surgical field. Furthermore, a frank preoperative discussion with the patient is mandatory. Informed consent must explicitly detail the risks of donor site pain, nerve injury (meralgia paresthetica), cosmetic deformity, and the potential for prolonged gait disturbances, ensuring the patient's expectations are properly aligned with the realities of autograft harvesting.
Patient positioning is entirely dependent on the chosen harvest site and must be executed with precision to optimize exposure and minimize complications. For anterior harvests, the patient is positioned supine. The critical maneuver is placing a small bump—typically a rolled towel or a saline bag—directly beneath the ipsilateral ischial tuberosity. This effectively elevates the hemipelvis and externally rotates the hip, bringing the anterior iliac crest into prominent relief. The ipsilateral arm should be secured across the chest to allow unhindered access to the surgical site. All bony prominences must be meticulously padded to prevent pressure necrosis.
For posterior harvests, the patient is positioned prone, typically on a radiolucent Jackson table or an OSI frame, which allows the abdomen to hang free and minimizes intra-abdominal pressure, thereby reducing epidural venous bleeding during the concomitant spinal procedure. The hips should be slightly flexed to relax the gluteal musculature and reduce tension on the posterior skin envelope. The operative table should be leveled, and the PSIS should be palpated and marked prior to draping. In both approaches, the surgical site must be prepped and draped widely to allow for extension of the incision if necessary, and fluoroscopy should be readily available if anatomical landmarks are obscured by body habitus.
Step-by-Step Surgical Approach and Fixation Technique
The execution of the iliac crest harvest demands the same level of respect and precision as the primary spinal procedure. Rough handling of tissues, blind plunging of osteotomes, and inadequate hemostasis are the primary drivers of donor site morbidity.
Anterior Tricortical Iliac Crest Bone Graft Harvest
With the patient positioned supine and the ipsilateral pelvis bumped, the ASIS and the iliac tubercle (2-3 cm posterior to the ASIS) are palpated and marked. An oblique skin incision, approximately 4 to 6 centimeters in length, is made parallel to the iliac crest, centered directly over the iliac tubercle. This placement avoids the ASIS, mitigating the risk of avulsion fractures and minimizing the chance of encountering an aberrant LFCN.

Dissection proceeds sharply through the subcutaneous adipose tissue down to the fascia overlying the iliac crest. Hemostasis is maintained with bipolar or monopolar electrocautery. The fascial incision is made directly over the cartilaginous cap of the crest. A Cobb elevator is then utilized to perform a meticulous subperiosteal dissection. Laterally, the origins of the tensor fascia latae and gluteal muscles are swept inferiorly. Medially, the abdominal musculature and iliacus are elevated. It is imperative to use broad, blunt retractors (such as Taylor or Meyerding retractors) to protect these soft tissues, taking special care not to compress the ilioinguinal nerve on the medial wall.

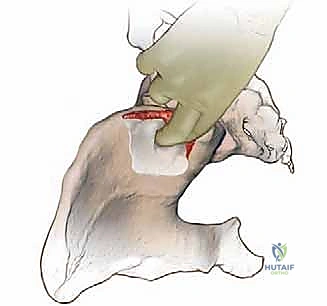
Once the inner and outer tables are adequately exposed, the dimensions of the required tricortical graft are mapped onto the bone. An oscillating saw is the preferred instrument for making the vertical cuts, as it provides precise, clean osteotomies without the micro-fracturing associated with aggressive osteotome use. Two parallel cuts are made perpendicular to the crest, extending through both the inner and outer cortices to the predetermined depth. A horizontal connecting cut is then made at the base of the vertical cuts.
Finally, a curved osteotome is gently advanced along the horizontal cut to liberate the graft. The tricortical block is carefully extracted. Following removal, meticulous hemostasis of the donor bed is paramount. Bone wax is pressed firmly into the exposed cancellous bone margins to arrest medullary bleeding, and a hemostatic agent (such as Gelfoam or Surgicel) may be packed into the defect. The wound is closed in multiple layers, ensuring a watertight fascial closure to prevent muscle herniation and a meticulous subcutaneous and subcuticular closure for optimal cosmesis.

Posterior Cancellous Iliac Crest Bone Graft Harvest
For the posterior approach, the patient is prone. The PSIS is identified, and an incision is made either vertically, parallel to the sacroiliac joint, or obliquely along the posterior iliac crest, starting just lateral to the PSIS and extending anteriorly for 5 to 7 centimeters. The incision must remain strictly within the safe zone, medial to the path of the superior cluneal nerves, which cross the crest approximately 8 cm lateral to the PSIS.
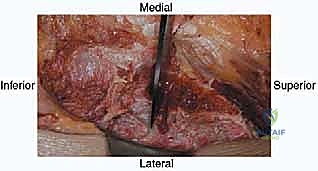
The subcutaneous tissue is divided, and the lumbodorsal fascia is incised over the crest. Subperiosteal dissection is performed laterally, reflecting the gluteus maximus and medius origins to expose the outer table of the ilium. The dissection must be carefully controlled as it proceeds inferiorly toward the greater sciatic notch. The surgeon should physically palpate the superior rim of the sciatic notch; all dissection and instrument placement must remain at least 2 to 3 centimeters cephalad to this landmark to absolutely avoid injuring the superior gluteal artery or sciatic nerve.
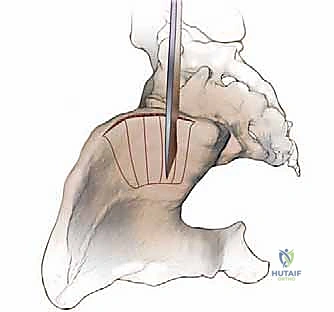
To harvest pure cancellous bone, a "trapdoor" or cortical window technique is highly effective. An osteotome or oscillating saw is used to outline a rectangular window on the outer cortex of the ilium. This cortical lid is carefully elevated or hinged open, exposing the rich cancellous reservoir within the false pelvis. Large gouges and curettes are then utilized to systematically harvest the cancellous bone, taking care not to breach the inner table, which could lead to retroperitoneal injury or hematoma.
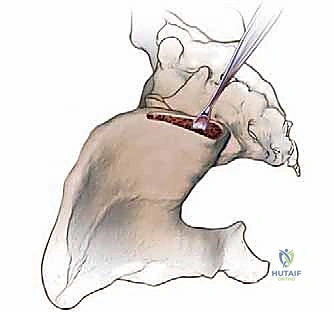
Once adequate volume is obtained, the cavity is inspected for arterial bleeders, which are cauterized or managed with bone wax. The cortical trapdoor is then repositioned over the defect, providing a structural roof that significantly reduces postoperative hematoma formation and pain. The fascial layers are closed tightly over a closed-suction drain if significant dead space or oozing is present, followed by standard layered soft tissue closure.
Complications, Incidence Rates, and Salvage Management
Despite meticulous technique, complications associated with ICBG harvest remain a clinical reality. Understanding the incidence and possessing the knowledge to manage these morbidities are essential components of the surgeon's armamentarium. Pain at the donor site is the most ubiquitous complication, often categorized as acute (resolving within weeks) or chronic (persisting beyond 6 months). Chronic pain is frequently neuropathic in nature, stemming from iatrogenic injury to regional sensory nerves.
Nerve injuries are highly specific to the approach. Anteriorly, the Lateral Femoral Cutaneous Nerve (LFCN) is at risk, leading to meralgia paresthetica. Posteriorly, the superior cluneal nerves are vulnerable. Vascular injuries, while less common, carry significantly higher morbidity. Laceration of the superior gluteal artery during a posterior harvest is a surgical emergency. Structural complications include fractures of the ilium, most notably avulsion fractures of the ASIS when anterior harvests are performed too far anteriorly, compromising the origin of the sartorius muscle.


Infection and hematoma formation are risks inherent to any surgical incision, but the creation of a large bony void in the ilium provides an ideal dead space for fluid accumulation. Meticulous hemostasis, the use of bone wax, and the strategic deployment of closed-suction drains are critical preventative measures. Herniation of abdominal contents through a full-thickness defect in the anterior ilium is a rare but documented complication, emphasizing the need for robust, multi-layered fascial closure.
| Complication | Estimated Incidence | Etiology / Risk Factor | Salvage Management & Prevention |
|---|---|---|---|
| Donor Site Pain (Chronic) | 10% - 30% | Nerve entrapment, altered pelvic biomechanics, large defect size. | Prevention: Precise internervous incisions, trapdoor technique. Management: Gabapentinoids, targeted nerve blocks, physical therapy. |
| Meralgia Paresthetica (LFCN Injury) | 2% - 10% (Anterior) | Direct transection, traction from retractors, aberrant nerve anatomy. | Prevention: Incise 2-3 cm posterior to ASIS. Management: Usually self-limiting; corticosteroid injections, rarely surgical neurolysis. |
| Cluneal Nerve Neuroma | 1% - 5% (Posterior) | Incision extending >7 cm lateral to PSIS. | Prevention: Stay within the medial safe zone. Management: Local anesthetic/steroid injections, surgical excision of neuroma. |
| Superior Gluteal Artery Hemorrhage | < 1% (Posterior) | Dissection/osteotome plunging into the greater sciatic notch. | Prevention: Palpate notch, stay 2 cm cephalad. Salvage: Immediate packing, attempt to clamp if visible; often requires emergent endovascular embolization. |
| ASIS Avulsion Fracture | 1% - 3% (Anterior) | Harvesting too close to the ASIS, compromising sartorius origin. | Prevention: Maintain a 2-3 cm bridge of intact bone at the ASIS. Management: Conservative (protected weight-bearing) vs. ORIF if widely displaced. |
| Deep Wound Infection / Hematoma | 1% - 4% | Inadequate hemostasis, dead space creation, prolonged operative time. | Prevention: Bone wax, tight fascial closure, subfascial drain. Management: I&D, targeted systemic antibiotic therapy. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation following an ICBG harvest must be carefully phased to balance the need for early mobilization (to prevent deep vein thrombosis and pulmonary complications) with the necessity of protecting the compromised pelvic ring. The immediate postoperative phase (Days 0-14) is heavily focused on pain management and safe ambulation. Multimodal analgesia is critical; the use of long-acting local anesthetics (such as liposomal bupivacaine) infiltrated directly into the periosteum and surrounding musculature at the time of closure can significantly reduce initial opioid requirements.
Weight-bearing status is generally dictated by the primary spinal procedure, but the harvest site itself warrants consideration. For standard posterior cancellous harvests or small anterior tricortical harvests, patients are typically allowed to weight-bear as tolerated (WBAT) immediately. However, if a massive anterior structural graft was taken, or if the cortical bridge near the ASIS is deemed tenuous, a period of protected weight-bearing with an assistive device (walker or crutches) may be instituted for 2 to 4 weeks to mitigate the risk of an avulsion fracture under the powerful pull of the sartorius and tensor fascia latae muscles.
The intermediate phase (Weeks 2-6) focuses on normalizing gait mechanics and initiating gentle core and pelvic stabilization exercises. Patients often exhibit an antalgic gait, leaning toward the operative side to reduce tension on the healing fascial and muscular incisions. Physical therapy should emphasize stretching of the hip flexors and abductors, alongside progressive strengthening of the gluteal complex. In the late phase (Weeks 6-12), as the bony defect begins to consolidate with fibrous tissue and early woven bone, patients can gradually return to higher-impact activities,
