Mastering Humeral Shaft Fixation: An Intraoperative Guide to Plate Osteosynthesis

Key Takeaway
This masterclass provides an exhaustive, step-by-step guide to plate fixation of humeral shaft fractures. Fellows will learn precise surgical anatomy, patient positioning, detailed intraoperative execution via anterolateral and posterior approaches, and critical pearls for avoiding complications. We cover fracture reduction, hardware application, and essential postoperative care, ensuring a comprehensive understanding of this vital orthopaedic procedure.
Comprehensive Introduction and Patho-Epidemiology
The humeral shaft, classically defined by Key’s landmarks as the anatomical region spanning from the upper margin of the pectoralis major tendon insertion proximally to the supracondylar ridge distally, represents a critical structural segment of the upper extremity. Fractures of the humeral diaphysis account for approximately 3% to 5% of all adult fractures. These injuries exhibit a bimodal distribution, typically affecting young males following high-energy trauma (such as motor vehicle collisions or falls from a significant height) and older females secondary to low-energy osteoporotic falls. Understanding the patho-epidemiology of these fractures is paramount for the orthopedic surgeon, as the mechanism of injury directly dictates the fracture morphology, the degree of soft tissue compromise, and the optimal treatment algorithm.
The mechanism of injury plays a determinative role in the resulting fracture pattern. Torsional forces classically produce spiral fractures, which are frequently seen in the distal third of the diaphysis (the Holstein-Lewis fracture pattern) and carry a heightened risk of radial nerve entrapment. Bending forces typically result in transverse or short oblique fractures, which are inherently unstable and prone to angulation. High-energy axial loading, conversely, yields highly comminuted or segmental fracture patterns, often accompanied by severe periosteal stripping and muscle interposition. The inherent displacement of the fracture fragments is further governed by the robust muscular attachments of the brachium. For instance, fractures proximal to the pectoralis major insertion result in abduction and external rotation of the proximal fragment via the rotator cuff, while fractures between the pectoralis major and deltoid insertions cause adduction of the proximal fragment.
Historically, the pendulum of treatment for humeral shaft fractures has rested firmly on the side of non-operative management. The seminal work of Sarmiento demonstrated that the humerus, being a non-weight-bearing bone enveloped by a robust muscular sleeve, possesses a remarkable capacity for healing via secondary intention using functional bracing. The upper extremity can tolerate significant malalignment without a precipitous drop in functional capacity—up to 20 degrees of anterior angulation, 30 degrees of varus angulation, and 3 centimeters of shortening are generally well-tolerated aesthetically and functionally. Initial management typically involves a coaptation splint or a posterior elbow splint to control pain and initial swelling, transitioning to a prefabricated functional fracture brace once the acute edema subsides, usually within 7 to 14 days.
However, the modern orthopedic landscape has witnessed a definitive paradigm shift. While non-operative management remains the gold standard for isolated, closed, low-energy fractures, there is a growing recognition of the limitations of functional bracing. Prolonged immobilization can lead to shoulder and elbow stiffness, and certain patient populations (e.g., the morbidly obese, non-compliant patients, or those with massive soft tissue injuries) cannot be adequately braced. Consequently, operative fixation—specifically plate osteosynthesis—has emerged as the definitive intervention for a distinct subset of fractures. Plating provides immediate mechanical stability, facilitates direct anatomical reduction, allows for the meticulous exploration of neurovascular structures, and permits accelerated rehabilitation. When executed with precision, plate osteosynthesis minimizes the risk of nonunion and guarantees restoration of the mechanical axis, directly translating into superior patient outcomes.
Detailed Surgical Anatomy and Biomechanics
A profound mastery of the surgical anatomy of the brachium is the absolute prerequisite for safe and effective humeral shaft plating. The humerus is not a uniform cylinder; its osteology transitions dramatically from proximal to distal. Proximally, the diaphysis is cylindrical, providing excellent cortical purchase for standard cortical screws. As one progresses distally, the shaft becomes distinctly triangular in cross-section before flattening out entirely in the distal third to form the medial and lateral supracondylar columns. This morphological transition dictates plate contouring and positioning. Proximal and midshaft fractures are typically addressed via an anterolateral approach, utilizing the broad, relatively flat anterolateral surface for plate application. Conversely, distal third fractures are often best managed via a posterior approach, applying the plate to the flat posterior cortex to maximize biomechanical stability and avoid impingement in the olecranon fossa.
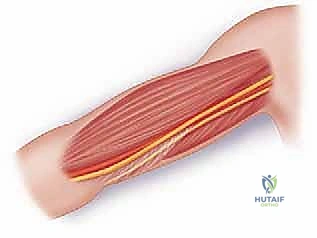
The muscular anatomy of the arm acts as both a deforming force and an anatomical roadmap. The brachium is divided into anterior and posterior compartments by the medial and lateral intermuscular septa. The anterior compartment houses the biceps brachii, coracobrachialis, and brachialis muscles, innervated primarily by the musculocutaneous nerve. The posterior compartment contains the triceps brachii, innervated by the radial nerve. Understanding the internervous planes between these compartments is critical. For the anterolateral approach, the primary working corridor is developed by splitting the brachialis muscle longitudinally. Because the medial two-thirds of the brachialis is innervated by the musculocutaneous nerve and the lateral one-third by the radial nerve, splitting the muscle at the junction of its middle and lateral thirds represents a true, safe internervous plane.
The neurovascular anatomy, specifically the radial nerve, is the most formidable obstacle in humeral shaft surgery. The radial nerve originates from the posterior cord of the brachial plexus and enters the posterior compartment of the arm through the triangular interval (bounded by the teres major superiorly, the long head of the triceps medially, and the humeral shaft laterally). It then spirals from medial to lateral along the posterior aspect of the humerus within the spiral groove. Crucially, the nerve lies directly on the periosteum in the mid-to-distal third of the humerus. On average, the radial nerve crosses the posterior humerus 20 centimeters proximal to the medial epicondyle and 14 centimeters proximal to the lateral epicondyle. It pierces the lateral intermuscular septum approximately 10 centimeters proximal to the lateral epicondyle to enter the anterior compartment. Any surgical approach, whether anterolateral or posterior, demands meticulous identification, mobilization, and protection of this structure to prevent devastating iatrogenic palsy.
The vascular supply to the humeral diaphysis must be respected to optimize biological healing. The primary nutrient artery enters the anteromedial cortex in the middle third of the diaphysis, directed distally. However, the periosteal blood supply, derived from muscular branches of the brachial artery anteriorly and the profunda brachii artery posteriorly, is equally critical, especially in comminuted fracture patterns. The profunda brachii artery accompanies the radial nerve through the spiral groove. Surgical dissection must be highly tissue-respecting. Excessive periosteal stripping during plate application completely devascularizes the cortical bone, precipitating delayed union, nonunion, or catastrophic implant failure. Modern techniques emphasize "biological plating," utilizing longer plates, fewer screws, and indirect reduction techniques to preserve the vital soft tissue envelope.
Exhaustive Indications and Contraindications
The decision to transition from non-operative bracing to surgical osteosynthesis must be predicated on a rigorous evaluation of absolute and relative indications. The goal of surgery is not merely to create a radiographically perfect bone, but to restore function, facilitate nursing care in polytraumatized patients, and prevent long-term disability. Absolute indications for immediate surgical intervention include open humeral shaft fractures, which require urgent irrigation, debridement, and stabilization to mitigate infection risk. Similarly, fractures associated with a concomitant vascular injury (such as a brachial artery tear) demand immediate skeletal stabilization to protect the vascular repair. The "floating elbow"—an ipsilateral fracture of the humeral shaft and the radius/ulna—is another absolute indication, as conservative management universally leads to profound instability and joint stiffness.
Relative indications, which constitute the majority of our surgical volume, require nuanced clinical judgment. Polytrauma patients with multiple system injuries benefit immensely from early humeral stabilization, as it allows for immediate weight-bearing through the upper extremity, facilitating transfers, upright positioning, and pulmonary toilet. Bilateral humeral shaft fractures must be fixed to allow the patient to perform basic activities of daily living and self-care. Furthermore, fractures that fail to achieve or maintain acceptable alignment in a functional brace (defined as >20 degrees anterior angulation, >30 degrees varus, or >3 cm shortening) warrant surgical correction. Pathologic fractures secondary to metastatic disease or primary bone tumors are routinely plated, often with supplemental polymethylmethacrylate (PMMA) cement, to provide immediate pain relief and mechanical stability.
The management of radial nerve palsy in the setting of a humeral shaft fracture requires specific attention. A primary (traumatic) radial nerve palsy present at the time of injury in a closed fracture is not an absolute indication for immediate exploration; literature demonstrates a spontaneous recovery rate exceeding 70%, and these are typically managed with observation and bracing. However, a secondary (iatrogenic or late-developing) radial nerve palsy that occurs after closed reduction or bracing is a strict indication for surgical exploration to rule out nerve entrapment within the fracture site. Additionally, open fractures with an associated radial nerve deficit, or the classic Holstein-Lewis distal third spiral fracture with a nerve deficit, strongly favor operative exploration and fixation.
Contraindications to operative fixation must be equally respected to avoid disastrous outcomes. Active, uncontrolled local infection is an absolute contraindication to internal fixation; such cases are better managed with external fixation. Severe soft tissue compromise, such as extensive burns, degloving injuries, or massive crush injuries overlying the surgical approach, preclude immediate plating due to the unacceptably high risk of wound breakdown and deep infection. Finally, patients who are medically unstable or possess severe medical comorbidities that make general anesthesia prohibitively dangerous should be managed non-operatively, accepting a potential malunion in favor of preserving life.
| Category | Specific Clinical Scenarios | Rationale for Management |
|---|---|---|
| Absolute Indications | Open fractures, Vascular injury, Floating elbow | Requires immediate stabilization to prevent infection, protect vascular repair, and restore limb stability. |
| Relative Indications | Polytrauma, Bilateral fractures, Pathologic fractures, Failure of conservative management | Facilitates early mobilization, nursing care, pain control, and prevents unacceptable functional malunion. |
| Nerve-Related Indications | Secondary/Late radial nerve palsy, Open fracture with nerve deficit, Holstein-Lewis with deficit | High suspicion for nerve entrapment or laceration requiring direct microsurgical evaluation and skeletal protection. |
| Absolute Contraindications | Active local infection, Severe medical instability, Massive overlying soft tissue compromise (burns/degloving) | High risk of deep hardware infection, anesthetic mortality, or catastrophic wound dehiscence. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the bedrock of a successful humeral osteosynthesis. The surgeon must never approach the operating table without a definitive, templated surgical blueprint. Planning begins with high-quality orthogonal radiography. Anteroposterior (AP) and lateral views of the entire humerus, inclusive of the shoulder and elbow joints, are mandatory to assess fracture morphology, comminution, and rule out intra-articular extension. In cases of severe comminution or high-energy trauma, traction radiographs can be invaluable for determining the true length of the humerus and the behavior of the fracture fragments under tension. If there is any suspicion of proximal or distal articular involvement, a dedicated non-contrast Computed Tomography (CT) scan with 3D reconstructions should be obtained to evaluate the joint surface and plan periarticular screw trajectories.
Templating is performed using digital software or traditional acetate overlays. The surgeon must select the appropriate implant type and length. For the adult humeral shaft, a 4.5mm narrow or broad Locking Compression Plate (LCP) or a dedicated pre-contoured humeral shaft plate is standard. The biomechanical goal is to achieve a minimum of six to eight cortices of secure fixation both proximal and distal to the fracture zone. In osteoporotic bone or highly comminuted patterns, longer plates spanning the entire diaphysis with fewer, widely spaced screws (bridge plating) are preferred to increase the working length of the construct and minimize strain at the fracture site. The surgeon must also anticipate the need for independent lag screws to compress simple spiral or oblique fracture planes prior to the application of the neutralization plate.
Patient positioning is dictated by the chosen surgical approach, which in turn is dictated by the fracture location. For proximal and middle-third fractures, the anterolateral approach is preferred. The patient is positioned supine on the operating table, shifted towards the edge of the bed on the operative side. A radiolucent hand table is securely attached to the bed. The injured arm is draped free and placed on the hand table in slight abduction (approximately 45 to 60 degrees). This position allows the surgeon to sit comfortably, provides unhindered access to the anterior brachium, and allows the C-arm to easily roll in from the head or foot of the bed to obtain orthogonal views without moving the patient's arm.


For distal-third fractures, or fractures requiring extensive exploration of the radial nerve in the spiral groove, the posterior approach is indicated. The patient may be positioned prone or in the lateral decubitus position. The lateral decubitus position is often favored as it poses fewer airway management challenges for the anesthesia team. The patient is secured with a beanbag, and all bony prominences are meticulously padded. The operative arm is draped free and supported over a padded post or a sterile stack of pillows, allowing the elbow to flex to 90 degrees. This position affords gravity-assisted retraction of the triceps and provides an unparalleled, direct en face view of the posterior humeral cortex and the radial nerve.
Step-by-Step Surgical Approach and Fixation Technique
The Anterolateral Approach
The anterolateral approach provides excellent exposure for the proximal two-thirds of the humeral shaft. The incision begins proximally at the level of the coracoid process, following the deltopectoral groove, and extends distally along the lateral border of the biceps brachii muscle belly, curving gently toward the center of the antecubital fossa.

Following skin incision, the subcutaneous tissues are sharply divided. Hemostasis is meticulously maintained using electrocautery. The deep fascia enveloping the arm is identified. As the dissection proceeds distally, the surgeon must maintain a high index of suspicion for the lateral antebrachial cutaneous nerve, which pierces the deep fascia lateral to the biceps tendon to become superficial. This nerve must be identified, mobilized, and protected with a vessel loop to prevent painful postoperative neuromas.

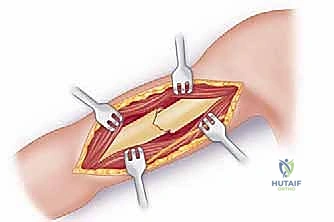
The deep dissection involves identifying the interval between the biceps brachii and the brachialis muscle. The biceps is retracted medially, exposing the underlying brachialis muscle draped over the anterior humerus. The brachialis is then split longitudinally. To utilize the true internervous plane, the split is made at the junction of the medial two-thirds (musculocutaneous nerve) and lateral one-third (radial nerve). The muscle is incised down to the periosteum.


Subperiosteal dissection is then performed to expose the fracture site. Retractors (such as Hohmann retractors) are carefully placed subperiosteally to protect the radial nerve laterally. The anterior half of the brachialis acts as a soft tissue cushion, protecting the radial nerve from the retractors.

The Posterior Approach
For distal third fractures, the posterior approach is utilized. A midline longitudinal incision is made over the posterior arm, extending from the tip of the olecranon proximally toward the acromion, tailored to the length of the plate required. The deep fascia is incised in line with the skin. The triceps can be managed via a muscle-splitting or a paratricipital (triceps-sparing) technique. In the classic splitting approach, the interval between the lateral and long heads of the triceps is developed proximally. Distally, the medial head of the triceps is split sharply in the midline down to the bone.
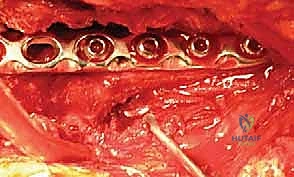
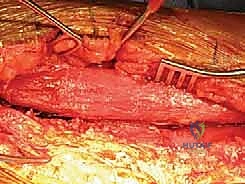
The absolute critical step in the posterior approach is the identification of the radial nerve and the profunda brachii artery. These structures cross the operative field from medial to lateral in the spiral groove. They must be meticulously dissected, tagged with a vessel loop, and gently mobilized. The plate will eventually be passed deep to the radial nerve, requiring careful spatial awareness to avoid compression or traction injury during fixation.

Fracture Reduction and Plate Osteosynthesis
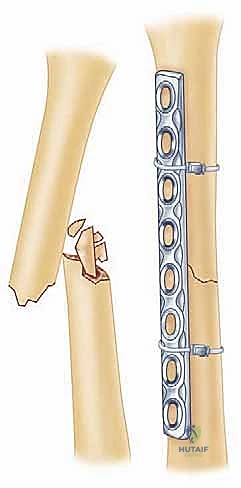
Once the fracture is adequately exposed and the neurovascular structures are protected, reduction is achieved. For simple fracture patterns (transverse, short oblique), the goal is absolute stability. The fracture ends are meticulously cleaned of hematoma and interposed soft tissue. Reduction is obtained using bone reduction forceps (e.g., Verbrugge clamps) or provisional Kirschner wires. If the fracture geometry allows, an independent 3.5mm or 4.5mm cortical lag screw is placed across the fracture plane to achieve interfragmentary compression.


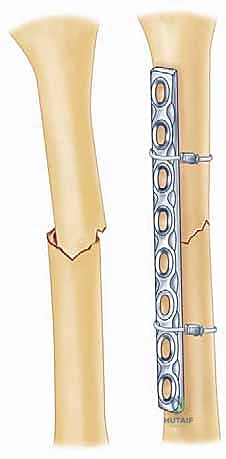
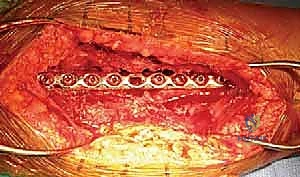
A properly contoured 4.5mm LCP is then applied to the tension side of the bone. For the anterolateral approach, this is the anterolateral cortex; for the posterior approach, it is the posterior cortex. The plate is secured using a combination of non-locking cortical screws to draw the plate to the bone and locking screws in osteoporotic bone or short end segments. If a lag screw cannot be placed independently, axial compression can be achieved dynamically using the eccentric drilling technique through the dynamic compression holes of the plate, or by utilizing an articulated tension device.


In cases of severe comminution, the biological bridge plating technique is employed. The fracture hematoma is left undisturbed. The plate is slid submuscularly across the comminuted zone, and fixation is achieved strictly in the healthy proximal and distal segments. This provides relative stability, promoting robust callus formation while preserving the fragile blood supply to the intermediate fragments.
Prior to final closure, the radial nerve is directly inspected to ensure it is free from hardware impingement. Copious irrigation is performed. The muscle fascia is loosely reapproximated to prevent compartment syndrome, and the
Clinical & Radiographic Imaging Archive