Mastering Hand & Forearm Surgical Approaches: An Intraoperative Guide
Key Takeaway
Welcome, fellows, to an immersive masterclass on hand, wrist, and forearm surgical approaches. We'll meticulously dissect crucial anatomy, navigate internervous planes, and execute precise techniques. From skin incisions to carpal tunnel release, this guide emphasizes real-time intraoperative decision-making, comprehensive neurovascular protection, and strategies to manage potential pitfalls, ensuring optimal patient outcomes.
Welcome, fellows, to the operating theater. Today, we embark on a critical journey: mastering the surgical approaches to the hand, wrist, and forearm. This region, unique in its intricate blend of bone, muscle, tendons, vessels, and nerves, demands an unparalleled depth of anatomical understanding. Our success hinges not just on knowing what to do, but why and how to do it with precision. The margin for error in the upper extremity is measured in millimeters; a slight deviation can result in devastating functional deficits for our patients.
As orthopedic surgeons, we must view the forearm and hand not merely as a collection of structures, but as a highly sophisticated, interconnected biomechanical engine. Every incision we make disrupts this delicate equilibrium. Therefore, our surgical approaches must be meticulously designed to exploit natural anatomical corridors, minimizing collateral damage while maximizing exposure. This chapter will serve as your definitive intraoperative guide, bridging the gap between textbook anatomy and practical, in-vivo surgical execution.
Comprehensive Introduction and Patho-Epidemiology
The surgical management of the hand and forearm encompasses a vast spectrum of pathology, ranging from high-energy traumatic injuries to insidious degenerative conditions. Epidemiologically, upper extremity trauma accounts for a significant proportion of emergency department visits worldwide, with distal radius fractures, flexor tendon lacerations, and peripheral nerve injuries being ubiquitous in clinical practice. Furthermore, elective procedures for conditions such as compressive neuropathies, inflammatory arthritides, and primary osteoarthritis constitute a major volume of an orthopedic hand surgeon's caseload. Understanding the patho-epidemiology of these conditions is essential, as the nature of the disease dictates the required surgical exposure.
Traumatic injuries often distort normal anatomy, making standard surgical approaches challenging. In cases of severe crush injuries or open fractures, the surgeon must adapt traditional incisions to incorporate traumatic wounds, always adhering to the principles of flap viability and soft tissue coverage. Degenerative conditions, conversely, often present with contracted tissues, osteophytes, and altered joint mechanics, requiring precise, tissue-sparing approaches to restore function without destabilizing the joint. The surgeon must anticipate these pathological alterations during preoperative planning to select the most appropriate and forgiving surgical corridor.
The evolution of surgical approaches in this region has been driven by a deeper understanding of microvascular anatomy and biomechanics. Historically, extensive, extensile exposures were favored, often at the expense of tissue devascularization and postoperative stiffness. Today, the paradigm has shifted toward minimally invasive techniques and meticulous preservation of the blood supply to tendons and bones. This evolution underscores the necessity of mastering internervous and intervascular planes, which allow for profound exposure without compromising the physiological integrity of the limb.
Detailed Surgical Anatomy and Biomechanics
The cornerstone of safe surgical dissection in the hand and forearm lies in the judicious use of internervous planes. These are anatomical corridors situated between muscles innervated by different nerves. By meticulously following these planes, we achieve extensive mobilization and exposure with minimal risk of muscle denervation, thereby preserving postoperative function. We must review the key compartments and their innervation, as this knowledge will guide every incision and dissection we make.
Volar Forearm and Hand Compartments
The volar aspect of the forearm and hand is densely packed with structures responsible for flexion, pronation, and intricate fine motor control. The superficial volar forearm consists of the pronator teres, flexor carpi radialis (FCR), palmaris longus, flexor carpi ulnaris (FCU), and flexor digitorum superficialis (FDS). With the exception of the FCU (innervated by the ulnar nerve), these superficial muscles are innervated by the median nerve. This shared innervation limits true internervous planes in the superficial volar forearm, forcing us to utilize intermuscular intervals, such as the plane between the FCR and the brachioradialis (the classic Henry approach), where we exploit the boundary between median and radial nerve territories.
Deep to this layer lies the deep volar forearm compartment, housing the flexor digitorum profundus (FDP), flexor pollicis longus (FPL), and the pronator quadratus. The innervation here is split: the anterior interosseous branch of the median nerve supplies the FPL, pronator quadratus, and the radial half of the FDP (index and middle fingers), while the ulnar nerve supplies the ulnar half of the FDP (ring and small fingers). Understanding this split is vital during deep dissections, particularly when addressing complex distal radius fractures or performing tendon transfers, as careless retraction can result in selective denervation of the profundus muscle bellies.
Moving distally into the hand, the anatomy compartmentalizes further. The thenar compartment (abductor pollicis brevis, flexor pollicis brevis, opponens pollicis) is primarily innervated by the recurrent motor branch of the median nerve—a structure of paramount importance that must be protected during carpal tunnel releases and thenar explorations. The adductor compartment (adductor pollicis) and hypothenar compartment (abductor digiti minimi, flexor digiti minimi brevis, opponens digiti minimi) are governed by the ulnar nerve. The interosseous compartment, comprising both dorsal and volar interossei, is also exclusively ulnar-innervated. Navigating the hand requires a profound respect for these terminal nerve branches, as true internervous planes are virtually nonexistent; dissection relies instead on precise interfascial separation.


Dorsal Forearm and Extensor Compartments
The dorsal forearm is primarily responsible for wrist and digital extension, as well as forearm supination. The musculature is broadly divided into the mobile wad and the dorsal extensor compartments. The mobile wad, consisting of the brachioradialis, extensor carpi radialis longus (ECRL), and extensor carpi radialis brevis (ECRB), is innervated by the radial nerve and its posterior interosseous branch (PIN). The interval between the mobile wad and the extensor digitorum communis (EDC) provides the classic Thompson approach to the proximal radius, utilizing the internervous plane between the radial nerve proper and the PIN.
The dorsal forearm musculature includes the abductor pollicis longus (APL), extensor pollicis brevis (EPB), extensor pollicis longus (EPL), EDC, extensor indicis proprius (EIP), extensor digiti quinti (EDQ), extensor carpi ulnaris (ECU), and the supinator. All these structures are innervated by the PIN. Because they share a single nerve source, surgical approaches on the dorsal forearm frequently rely on intermuscular planes rather than true internervous corridors. Careful blunt dissection and an intimate knowledge of the PIN's course through the supinator and along the interosseous membrane are mandatory to avoid iatrogenic nerve palsy.
At the level of the wrist, the extensor tendons are organized into six distinct dorsal compartments by the extensor retinaculum. This retinacular system prevents bowstringing during wrist extension and provides biomechanical advantage. Surgical approaches to the dorsal wrist, whether for ligamentous repair, carpectomy, or arthrodesis, often involve elevating these compartments subperiosteally or performing step-cut lengthenings of the retinaculum to prevent postoperative tendon subluxation or bowstringing.
Internervous Planes and Biomechanical Considerations
Understanding these relationships is paramount. Any deviation from these internervous planes risks injury to the underlying neural structures or denervation of critical musculature, leading to functional deficits. When we exploit an internervous plane, we are physically separating muscles that receive their electrical signals from entirely different sources. This means that aggressive retraction on one side of the plane will not stretch or avulse the nerve supply to the muscle on the opposite side.
Biomechanically, the preservation of these muscular units is essential for the intricate balance of the hand. The hand operates on a complex system of agonist-antagonist relationships, coupled with the tenodesis effect of the wrist. If a surgical approach damages the motor branch to the FPL, for example, the patient loses interphalangeal joint flexion of the thumb, severely compromising pinch strength and fine manipulation. Similarly, damage to the PIN during a dorsal approach will lead to a devastating drop finger or drop wrist deformity, requiring complex secondary tendon transfers to salvage function.
Furthermore, the vascular supply to the tendons and nerves must be respected. Tendons in the hand and forearm receive their blood supply through delicate vincula and specialized paratenon networks. Extensive stripping of these structures during surgical exposure will lead to tendon ischemia, increasing the risk of postoperative rupture or dense adhesion formation. Our approaches must be designed to lift full-thickness flaps, preserving the microvascular networks that are crucial for primary tissue healing and the restoration of gliding mechanics.
Exhaustive Indications and Contraindications
The selection of a surgical approach is never arbitrary; it is a calculated decision based on the specific pathology, the required exposure, and the patient's individual anatomy. A comprehensive understanding of the indications and contraindications for each approach ensures that the surgeon can achieve their operative goals while minimizing iatrogenic harm. The following table outlines the general parameters guiding approach selection in the hand and forearm.
| Surgical Approach | Primary Indications | Relative Contraindications | Absolute Contraindications |
|---|---|---|---|
| Volar Henry (Forearm) | Distal radius fractures (volar shear/bending), flexor tendon repairs, median nerve exploration, radial artery repair. | Severe volar soft tissue compromise, extensive dorsal comminution requiring dorsal plating. | Active volar compartment infection (unless for I&D), unsalvageable volar skin necrosis. |
| Dorsal Thompson (Forearm) | Proximal/mid-shaft radius fractures, PIN exploration, radial head/neck fractures (extensile). | Isolated volar pathology, preexisting PIN palsy (unless exploring the nerve). | Overlying burn eschar or severe dorsal soft tissue trauma precluding closure. |
| Midaxial (Digit) | Flexor tendon sheath infections, digital nerve/artery repair, complex phalangeal fractures. | Pathology requiring bilateral exposure of the digit, severe crush injury to the midaxial line. | None, provided the neurovascular bundle can be safely identified and protected. |
| Bruner Zigzag (Digit) | Flexor tendon repair/tenolysis, trigger finger release, Dupuytren's fasciectomy. | Severe joint contractures where straight incisions might be preferred for local flap coverage. | Previous longitudinal incisions that would create narrow, non-viable skin bridges. |
| Dorsal Longitudinal (Wrist) | Carpal tunnel release (dorsal approach rarely used), proximal row carpectomy, wrist arthrodesis, extensor tendon repairs. | Volar carpal pathology (e.g., volar perilunate dislocations requiring volar ligament repair). | Inadequate dorsal skin coverage, active dorsal cellulitis. |
When considering a volar approach, particularly the modified Henry approach to the distal radius, the indications are broad. It is the workhorse approach for the vast majority of distal radius fractures, allowing for the application of volar locking plates which biomechanically buttress the subchondral bone. However, if the patient presents with a severe dorsal shear injury or a highly comminuted dorsal cortex that cannot be indirectly reduced from the volar side, a dorsal or combined approach may be indicated.
Conversely, dorsal approaches to the hand and wrist are heavily utilized for extensor tendon pathology, carpal instability, and arthrodesis. The dorsal skin is highly mobile, allowing for extensive exposure through relatively small incisions. However, the dorsal soft tissue envelope is thin, and prominent hardware placed dorsally is notorious for causing extensor tendon irritation and eventual rupture. Therefore, a relative contraindication to a purely dorsal approach is the need for massive, bulky internal fixation, unless the surgeon is prepared to perform complex retinacular flaps to shield the tendons.
Midaxial and volar zigzag (Bruner) incisions are the mainstays of digital surgery. The Bruner incision provides unparalleled exposure to the volar flexor apparatus and is indicated for almost all flexor tendon repairs. However, in cases of severe finger trauma where the volar skin is compromised, a midaxial approach may be preferred, as it utilizes the relatively pristine lateral skin and avoids placing a surgical scar directly over the gliding surface of the flexor tendons. The surgeon must weigh these factors meticulously before putting scalpel to skin.
Pre-Operative Planning, Templating, and Patient Positioning
Before we even consider making an incision, meticulous planning is essential. The success of a complex hand or forearm reconstruction is often determined before the patient enters the operating room. This phase requires a systematic approach, integrating clinical findings, advanced imaging, and ergonomic preparation to ensure a flawless intraoperative execution.
Radiographic Evaluation and Templating
Radiographic templating is a non-negotiable step for any bony procedure in the upper extremity. We must review pre-operative radiographs, including true orthogonal AP and lateral views, and often specialized views such as the scaphoid or carpal tunnel view. For complex intra-articular fractures or carpal instability, a fine-cut computed tomography (CT) scan with 3D reconstructions is invaluable. It allows us to map fracture lines, understand articular step-offs, and plan the exact trajectory of our fixation devices.
Once the imaging is thoroughly analyzed, we proceed to digital or acetate templating. We must select the appropriate implant sizes, anticipate screw lengths, and plan the sequence of reduction and fixation. For instance, when templating a volar plate for a distal radius fracture, we must ensure the plate does not extend past the watershed line, which would risk flexor tendon attrition. We must also template the subchondral support screws to ensure they are of adequate length to support the articular surface without penetrating the dorsal cortex or the radiocarpal joint.
Furthermore, we must clearly define the surgical procedure and be prepared for potential intraoperative variations or alternatives. If a primary repair of a flexor tendon is deemed impossible due to retraction or tissue loss, we must have the equipment and consent ready for a tendon graft or a staged reconstruction with a silicone rod. Anticipating these scenarios and having the necessary implants, grafts, and specialized micro-instruments immediately available prevents dangerous intraoperative delays.
Operating Room Setup and Ergonomics
For most hand, wrist, and forearm procedures, the patient will be in a supine position. The operative extremity is extended on a stable, well-secured hand table. This table must allow ample space for the limb, as well as for the surgeon's and assistants' elbows and forearms to minimize fatigue and enhance stability during delicate maneuvers. An unstable or cramped hand table is a recipe for surgical disaster, particularly when performing microsurgical anastomoses or precise articular reductions.
Ergonomics cannot be overstated. We will be seated on stable, comfortable stools. Adjust your stool height so your knees are level with your hips, and your feet are resting flat on the ground. Your elbows should rest comfortably on the hand table, providing a stable fulcrum for your hands. This ergonomic setup is critical for maintaining focus, eliminating physiological tremor, and ensuring precision over extended periods. If you are straining or uncomfortable, your surgical technique will inevitably suffer.
Lighting and hemostasis are the final pillars of our setup. Angle the operating lights directly over the hand table. Crucially, avoid positioning them behind the surgeon's or assistant's shoulder, as this will cast shadows on our operative field, obscuring critical structures. A pneumatic tourniquet is routinely advised for nearly all hand and forearm surgeries. This provides a bloodless field, which is absolutely essential for clear visualization of delicate neurovascular structures, tendons, and joint anatomy. We will inflate the tourniquet after meticulous limb exsanguination with an Esmarch bandage, typically setting the pressure to 100 mmHg above the patient's systolic blood pressure, monitoring the tourniquet time meticulously to prevent ischemic nerve injury.

Step-by-Step Surgical Approach and Fixation Technique
Now, let's move into the specifics of our approaches. Remember, fellows, every cut, every retraction, every stitch is a deliberate act informed by our anatomical knowledge. We do not simply cut through tissue; we navigate through anatomical corridors, respecting the physiological boundaries that dictate postoperative function.
Principles of Hand and Digit Incisions
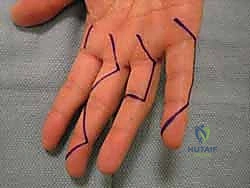
The skin of the hand is unique. While it offers versatility in incision placement, strict adherence to certain principles is mandatory to prevent functional impairment and unsightly scarring. Before any skin is incised, use a sterile surgical marker to meticulously outline your planned incision. This confirms the appropriate position, ensures adequate skin bridges if multiple incisions are planned, and serves as a guide for accurate closure.
A cardinal rule of hand surgery is to never make an incision perpendicular to a volar flexion crease. Such incisions will inevitably lead to scar formation and secondary skin contractures, severely limiting motion and function. While incisions can be made within volar skin creases, especially in the palm, deep creases should be approached with caution. The subcutaneous tissue here is thin, making skin edge apposition difficult upon closure and increasing the risk of maceration.
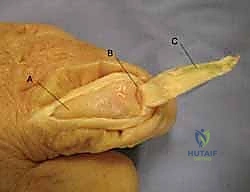
For volar digital exposures, the Bruner zigzag pattern is preferred. This pattern crosses creases laterally and at angles (typically 90 degrees), distributing tension and allowing for better scar maturation. The apices of the zigzag flaps must reach the midaxial line to ensure adequate exposure and prevent the scar from migrating volarly and causing a flexion contracture. When elevating these flaps, the dissection must remain superficial to the flexor tendon sheath, preserving the delicate neurovascular bundles that lie just volar to Cleland's ligaments.
Alternatively, midaxial incisions are ideally placed at the junction of the glabrous (hairless, volar) and non-glabrous (hairy, dorsal) skin. This approach provides excellent access to the flexor sheath and phalanges while keeping the scar off the volar tactile surface. Pay meticulous attention to the neurovascular bundle. You can either take the bundle volarly with the volar skin flap, requiring sharp dissection, or leave it in situ by dissecting superficial to it. Always visualize or palpate the bundle; uncontrolled dissection here is unacceptable.

Approaches to the Interphalangeal Joints
When approaching the proximal interphalangeal (PIP) or distal interphalangeal (DIP) joints, our primary concern is the integrity of the extensor mechanism and the delicate germinal matrix at the DIP joint. Dorsal approaches are standard for joint fusions, fracture reductions, and extensor tendon repairs.
Skin incisions over the IP joints can be straight dorsal longitudinal, which is straightforward but carries a slight risk of scar contracture. For broader exposure or to avoid straight-line scars, consider an S-type, chamfered, or chevron-style incision. These curvilinear incisions provide excellent access while minimizing tension on the healing skin edges during joint flexion.
At the PIP joint, there is no true internervous plane dorsally. The extensor mechanism will be immediately evident once the skin and subcutaneous tissue are incised. To access the joint, the surgeon can split the extensor tendon longitudinally (often utilized for central slip avulsion fractures) or elevate the interval between the central slip and the lateral bands. Extreme care must be taken not to damage the central slip insertion on the base of the middle phalanx, as this will result in a devastating boutonniere deformity.

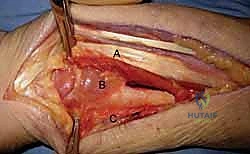
Volar Approach to the Forearm and Wrist
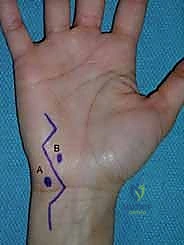
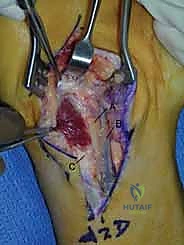
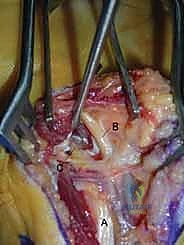
The volar approach to the forearm, primarily utilizing the Henry interval, is the gold standard for exposing the volar radius. The incision is typically made along the course of the FCR tendon. After incising the skin and superficial fascia, the FCR sheath is opened, and the tendon is retracted ulnarly. This protects the median nerve, which lies ulnar to the FCR.
Deep to the FCR, the surgeon encounters the flexor pollicis longus (FPL) and the pronator quadratus (PQ). To expose the distal radius, the PQ must be elevated. This is traditionally done via an L-shaped incision along its radial and distal borders, leaving a small cuff of tissue for later repair. The PQ is then reflected ulnarly, exposing the pristine volar cortex of the distal radius.
During this deep dissection, the radial artery must be identified and protected. It runs along the radial border of the FCR and can be mobilized radially. Furthermore, when dissecting proximally in the forearm, the surgeon must be acutely aware of the superficial branch of the radial nerve, which emerges from beneath the brachioradialis in the mid-forearm. Retraction must be gentle to avoid neuropraxia.


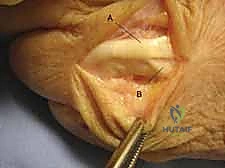
Dorsal Approach to the Forearm and Wrist
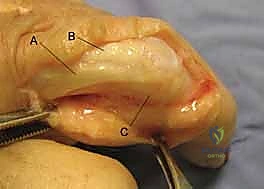
The dorsal approach to the wrist is utilized for carpal procedures, distal radius plating (when indicated), and extensor tendon surgery. A longitudinal incision is typically centered over Lister's tubercle. The dissection proceeds through the subcutaneous tissue, taking care to identify and protect the dorsal sensory branches of the radial and ulnar nerves, which are highly susceptible to painful neuroma formation if injured.
The extensor retinaculum is then exposed. To access the radiocarpal joint or the distal radius, the third extensor compartment is opened, and the extensor pollicis longus (EPL) tendon is transposed radially. This allows the surgeon to elevate the second and fourth compartments subperiosteally, creating a robust, full-thickness flap that protects the extensor tendons from underlying hardware or bony irregularities.
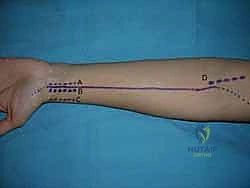
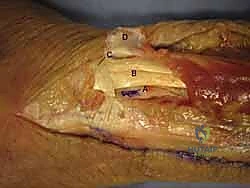
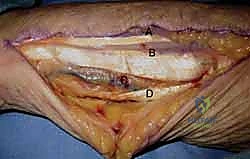
When approaching the proximal dorsal forearm, the Thompson approach utilizes the interval between the ECRB and the EDC. This approach is excellent for exposing the proximal and middle thirds of the radius. The critical structure here is the posterior interosseous nerve (PIN), which emerges from the supinator muscle. The supinator must be carefully elevated off the radius, often requiring supination of the forearm to move the PIN safely out of the surgical field.
Complications, Incidence Rates, and Salvage Management
Despite meticulous technique and adherence to anatomical principles, complications can and do occur in hand and forearm surgery. Recognizing these potential pitfalls, understanding their incidence, and knowing how to manage them are hallmarks of a master surgeon. The dense concentration of critical structures means that a minor technical error can translate into significant morbidity.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Iatrogenic Nerve Injury | 1% - 5% | Overzealous retraction, errant scalpel placement, failure to identify anatomical variants (e.g., Martin-Gruber anastomosis). | Immediate microsurgical primary repair if recognized intraoperatively. Late recognition requires EMG mapping, neurolysis, or nerve grafting. |
| Tendon Adhesions | 10% - 30% | Excessive tissue handling, failure to repair paratenon, prolonged postoperative immobilization, prominent hardware. | Aggressive hand therapy. If refractory after 6 months, surgical tenolysis and potential application of anti-adhesion barriers. |
| Complex Regional Pain Syndrome (CRPS) | 2% - 15% | High-energy trauma, tight cast application, unaddressed nerve irritation, psychological factors. | Early recognition is paramount. Multidisciplinary approach: aggressive physical therapy, gabapentinoids, sympathetic nerve blocks, Vitamin C prophylaxis. |
| Hardware Prominence / Tendon Rupture | 3% - 8% | Volar plates placed distal to the watershed line (FPL rupture), prominent dorsal screws (extensor rupture). | Hardware removal once fracture is healed. If tendon rupture occurs, requires tendon transfer (e.g., EIP to EPL) or grafting. |
| Infection (Deep Space) | < 2% | Prolonged operative time, severe open fractures, immunocompromised state (diabetes, smoking). | Emergent surgical irrigation and debridement (I&D), targeted intravenous antibiotic therapy based on intraoperative cultures. |
Iatrogenic nerve injury is perhaps the most feared complication. The superficial sensory branches of the radial nerve (Wartenberg's nerve) and the dorsal ulnar sensory nerve are particularly vulnerable during dorsal approaches. Injury to these nerves can result in debilitating neuromas, which are notoriously difficult to treat and often require surgical excision and burying of the nerve stump into deep muscle or bone. Prevention through careful, blunt subcutaneous dissection is the only true solution.
Tendon adhesions are a frequent consequence of surgical trauma, particularly in zone II of the hand (the "no man's land"). The delicate balance between allowing tissues to heal and preventing them from scarring together requires masterful surgical technique and precise postoperative therapy. If dense adhesions form, a secondary tenolysis may be necessary. This is a technically demanding procedure where the surgeon must meticulously free the tendon from surrounding scar tissue without devascularizing it or causing it to rupture.
Complex Regional Pain Syndrome (CRPS) is a devastating complication characterized by disproportionate pain, swelling, stiffness, and sudomotor changes. While its exact pathophysiology remains elusive, it is often triggered by surgical trauma or tight immobilization. Prevention involves meticulous, atraumatic surgical technique, adequate postoperative pain control
Clinical & Radiographic Imaging Archive



