

Comprehensive Introduction and Patho-Epidemiology
Proximal humerus fractures represent a significant and growing proportion of orthopedic trauma, accounting for approximately five percent of all fractures presenting to the emergency department. The epidemiologic distribution is classically bimodal, affecting high-energy trauma patients in younger demographics and, vastly more commonly, low-energy falls in the osteoporotic elderly population. While the majority of these injuries are minimally displaced and amenable to non-operative management, complex three- and four-part fractures, fracture-dislocations, and head-splitting variants present a formidable reconstructive challenge. Historically, open reduction and internal fixation (ORIF) in osteoporotic bone yielded unacceptably high rates of hardware failure, screw cut-out, and avascular necrosis (AVN).
The advent of proximal humerus hemiarthroplasty, pioneered by Charles Neer in the 1970s, revolutionized the management of these devastating injuries. However, it is a profound misconception to view this procedure merely as the insertion of a metallic spacer. Proximal humerus hemiarthroplasty is, in its essence, a complex soft-tissue reconstruction masquerading as a bony operation. The metallic stem and head serve primarily as a stable scaffold upon which the critical rotator cuff tuberosities must be anatomically reduced and rigidly fixed to achieve osseous union. Failure to achieve tuberosity healing inevitably leads to superior migration of the prosthesis, devastating loss of active elevation, and profound functional disability.
In recent years, the pendulum has swung towards reverse total shoulder arthroplasty (RTSA) for elderly patients with complex fractures, largely due to its reliance on deltoid mechanics rather than tuberosity healing. Nevertheless, hemiarthroplasty remains an indispensable tool in the armamentarium of the orthopedic surgeon. It is the procedure of choice for younger, active patients with non-reconstructable articular segments but robust, repairable tuberosities, where preserving the native glenoid and restoring native biomechanics is paramount. The success of this operation hinges on an uncompromising understanding of surgical anatomy, meticulous preoperative templating, and flawless intraoperative execution.
Detailed Surgical Anatomy and Biomechanics
Before the scalpel touches skin, the orthopedic surgeon must possess a three-dimensional mastery of the proximal humerus and its surrounding soft-tissue envelope. The proximal humerus is a marvel of biomechanical engineering, functioning as the fulcrum for the most mobile joint in the human body. It is conceptually divided into four critical osseous segments, as codified by Neer: the articular segment (the humeral head), the greater tuberosity, the lesser tuberosity, and the humeral diaphysis. The dynamic interplay between these segments and their muscular attachments dictates both the fracture pattern and our reconstructive strategy.
Osteology and Articular Geometry
The native humeral head is not a perfect sphere; it is a complex ovoid that articulates with the shallow glenoid fossa. The geometric relationship between the articular surface and the surrounding landmarks is crucial for prosthetic reconstruction. The native humeral version averages approximately 30 degrees of retroversion relative to the epicondylar axis of the distal humerus, though this can range widely from 10 to 55 degrees in the normal population. Furthermore, the most cephalad surface of the articular segment typically sits roughly 8 millimeters superior to the superior tip of the greater tuberosity.
Restoring this precise height and version is the crux of intraoperative trialing. If the prosthesis is placed too high (proud), it will over-tension the rotator cuff, leading to tuberosity pull-off, impingement, and secondary rotator cuff failure. If placed too low, the deltoid and remaining cuff will be lax, resulting in profound weakness and inferior subluxation. The intertubercular groove, or bicipital groove, lies between the greater and lesser tuberosities, providing a crucial passageway for the long head of the biceps tendon. This tendon serves as the intraoperative "lighthouse," guiding the surgeon to the interval between the subscapularis and the supraspinatus, and orienting the rotational alignment of the reconstruction.
Critical Vascular Supply and Osteonecrosis Risk
The lifeblood of the humeral head, and a primary concern in the evaluation of displaced fractures, relies on a delicate and easily disrupted vascular network. Historically, the anterolateral branch of the anterior humeral circumflex artery, famously known as the arcuate artery of Laing, was considered the dominant blood supply. This vessel typically courses parallel to the lateral aspect of the long head of the biceps tendon, penetrating the humeral head at the proximal extent of the intertubercular groove.
However, modern microvascular injection studies have definitively proven that the posterior humeral circumflex artery provides the vast majority of the intraosseous blood supply to the humeral head. Despite this paradigm shift, the anterior circulation remains a critical surgical landmark, and extensive disruption of the medial calcar hinge—often seen in highly displaced four-part fractures or anatomic neck fractures—predictably severs the intraosseous anastomoses, condemning the articular segment to avascular necrosis. Understanding this vascular compromise is what drives the indication for arthroplasty over internal fixation in specific fracture patterns.
Neurovascular Topography and Muscular Deforming Forces
The surgical approach and the fracture deformity itself are dictated by the surrounding neurovascular structures and muscular attachments. The axillary nerve is the most vulnerable structure during this procedure. It exits the quadrangular space and wraps around the surgical neck of the humerus, typically 5 to 7 centimeters distal to the lateral edge of the acromion. It innervates the deltoid and teres minor; iatrogenic injury results in catastrophic loss of shoulder abduction. We must identify and protect it, recognizing that external rotation of the humerus helps relax the nerve and move it away from the retractor blades.
The musculocutaneous nerve, located more medially and posterior to the conjoint tendon, innervates the coracobrachialis, biceps brachii, and brachialis muscles. Aggressive medial retraction of the conjoint tendon can cause a traction neuropraxia.
The deforming forces on the fracture fragments are predictable and powerful. The supraspinatus, infraspinatus, and teres minor insert on the greater tuberosity, pulling it superiorly and posteriorly. The subscapularis inserts on the lesser tuberosity, pulling it medially and creating internal rotation. The pectoralis major, inserting on the lateral lip of the bicipital groove, pulls the humeral shaft medially and anteriorly, while the deltoid pulls the shaft proximally. Overcoming these forces is essential for mobilizing the shaft and reducing the tuberosities around the prosthesis.
Exhaustive Indications and Contraindications
The decision to proceed with proximal humerus hemiarthroplasty requires a nuanced evaluation of the patient's physiologic age, bone quality, fracture morphology, and functional demands. It is not a universally applicable solution, and inappropriate patient selection is a primary driver of poor clinical outcomes.
Patient Selection Algorithms
Hemiarthroplasty is generally indicated for complex fractures where the articular segment is deemed non-viable or non-reconstructable, but the tuberosities and rotator cuff are intact and amenable to robust surgical repair. This classically includes head-splitting fractures, where the articular cartilage is severely comminuted, and true anatomic neck fractures, which carry a near 100% rate of avascular necrosis.
In the physiologically younger patient (typically under 65 years of age) with a high-energy four-part fracture, hemiarthroplasty is often preferred over RTSA to preserve the native glenoid bone stock and theoretically allow for a higher ceiling of postoperative function, provided the tuberosities heal. However, in the elderly, osteoporotic patient with a four-part fracture, the literature increasingly supports RTSA due to the high rate of tuberosity nonunion and subsequent functional failure associated with hemiarthroplasty in this demographic.
Tabular Summary of Indications and Contraindications
| Category | Specific Clinical Scenarios | Rationale / Considerations |
|---|---|---|
| Primary Indications | Head-splitting articular fractures | Cartilage is irreparably damaged; ORIF is impossible. |
| True anatomic neck fractures | Complete disruption of blood supply; inevitable AVN. | |
| 4-part fractures in younger/active patients | Preserves glenoid bone stock; relies on robust tuberosity healing. | |
| Chronic fracture-dislocations (>40% head defect) | Massive impaction injuries (e.g., severe Hill-Sachs or reverse Hill-Sachs) precluding joint salvage. | |
| Relative Contraindications | Elderly patients (>70 years) with osteopenia | High risk of tuberosity nonunion; RTSA is generally preferred. |
| Pre-existing rotator cuff arthropathy | Hemiarthroplasty will fail without a competent cuff; requires RTSA. | |
| Parkinson's disease or severe neurologic deficits | Inability to comply with rehab; high risk of dislocation or tuberosity failure. | |
| Absolute Contraindications | Active glenohumeral or systemic infection | High risk of prosthetic joint infection. |
| Irreparable rotator cuff tear in the acute setting | Tuberosities cannot be reconstructed; prosthesis will migrate superiorly. | |
| Moribund patient / non-ambulatory status | Surgical risks outweigh potential functional benefits; non-operative management indicated. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the bedrock of a successful hemiarthroplasty. The surgeon must enter the operating theater with a clear, three-dimensional understanding of the fracture geometry and a precise plan for implant sizing and placement.
Advanced Imaging and Classification Paradigms
Standard radiographic evaluation must include a true anteroposterior (AP) view of the glenohumeral joint (Grashey view), a scapular Y view, and an axillary lateral view.
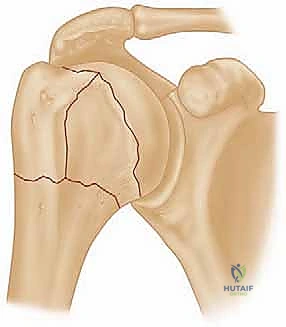
FIG 1 • Neer classification of proximal humerus fractures: 1, greater tuberosity; 2, lesser tuberosity; 3, articular surface; 4, shaft.

FIG 2 • AP view of a displaced three-part proximal humerus fracture without evidence of concomitant dislocation.

FIG 2 • Axillary view of a displaced three-part proximal humerus fracture without evidence of concomitant dislocation.
If patient pain precludes a standard axillary view, a Velpeau axillary view is mandatory to rule out subtle posterior dislocations and assess glenoid version. However, plain radiography is often insufficient for complex proximal humerus fractures. A non-contrast computed tomography (CT) scan with 3D reconstructions is virtually mandatory. The CT scan allows the surgeon to precisely quantify the degree of tuberosity comminution, identify occult head-splitting components, and assess the available metaphyseal bone stock for stem fixation. We classify these fractures using the Neer classification, which focuses on the displacement of the four anatomical segments.
Digital Templating and Implant Selection
Digital templating is performed using the AP and axillary radiographs of the contralateral, uninjured shoulder. Because the fractured proximal humerus is distorted, the normal side provides the most accurate blueprint for restoring native anatomy. We template to determine three critical parameters: the radius of curvature of the humeral head, the diameter of the humeral diaphysis to select the appropriate stem thickness, and the distance from the superior margin of the pectoralis major insertion to the top of the humeral head.
This last measurement is a vital intraoperative landmark. On average, the distance from the proximal edge of the pectoralis major tendon to the superior aspect of the articular surface is approximately 5.6 centimeters. Knowing this specific patient's measurement allows us to accurately set the height of the prosthesis even when the proximal landmarks are completely destroyed.
Anesthesia and Optimal Beach Chair Positioning
The procedure is typically performed under general endotracheal anesthesia, heavily supplemented by a regional interscalene nerve block. The block provides profound intraoperative muscle relaxation, which is essential for mobilizing retracted fracture fragments, and ensures excellent postoperative analgesia, minimizing the need for systemic narcotics.
The patient is meticulously positioned in the beach chair position. The torso is elevated to 45 to 60 degrees, and the hips and knees are flexed to prevent sliding and reduce tension on the sciatic nerve. The head must be secured in a neutral position within a specialized headrest to prevent catastrophic cervical spine extension or brachial plexus traction injuries. The operative arm is draped free and ideally suspended in a sterile, articulating arm positioner (e.g., a Spider or Trimano arm). This device allows the surgeon to independently control the arm's position—abduction, adduction, internal, and external rotation—which is critical for exposing the various facets of the proximal humerus during the procedure. The C-arm fluoroscopy unit is brought in from the contralateral side or the head of the bed, ensuring that unobstructed AP and axillary views can be obtained without compromising the sterile field.
Step-by-Step Surgical Approach and Fixation Technique
With the patient prepped and draped, and prophylactic antibiotics circulating, the surgical reconstruction commences. The procedure demands meticulous soft-tissue handling, precise osseous preparation, and a rigid, biomechanically sound reconstruction of the tuberosities.
The Deltopectoral Approach and Interval Development
We utilize the classic deltopectoral approach, which provides extensile exposure to the anterior shoulder without denervating any musculature. The incision begins just lateral to the tip of the coracoid process and extends distally and laterally along the deltopectoral groove toward the deltoid tuberosity.
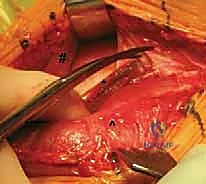
TECH FIG 1 • A. The skin incision is centered over the anterior deltoid. The deltopectoral interval is developed with lateral retraction of the cephalic vein.
Subcutaneous dissection reveals the deltopectoral fascia. The key landmark is the cephalic vein. While historically there has been debate regarding whether to retract the vein medially or laterally, the current consensus favors lateral retraction. Retracting the vein laterally with the deltoid preserves its primary venous tributaries from the deltoid muscle, reducing postoperative edema and the risk of vein thrombosis.

TECH FIG 1 • B. For more exposure, the superior 1 cm of the pectoralis major tendon may be incised. (^, pectoralis major; #, deltoid; , cephalic vein.)*
The clavipectoral fascia is incised lateral to the conjoint tendon. At this juncture, the fracture hematoma is usually encountered and evacuated. To gain adequate exposure of the humeral shaft, especially in cases with significant proximal migration of the diaphysis, it is often necessary to release the proximal 1 to 2 centimeters of the pectoralis major tendon insertion. This release must be carefully documented and repaired at the conclusion of the case, but it is essential for mobilizing the shaft without placing undue traction on the soft tissues.
Tuberosity Mobilization and Humeral Head Extraction
The next critical step is identifying and gaining control of the tuberosity fragments before the humeral head is removed. Once the head is extracted, the soft-tissue tension is lost, and the tuberosities will retract massively into the subacromial and posterior spaces, making them exceedingly difficult to retrieve.
We identify the long head of the biceps tendon in the bicipital groove. The lesser tuberosity lies medial to the groove, and the greater tuberosity lies lateral. Heavy, non-absorbable, braided sutures (e.g., #5 or #2 high-strength tape) are passed through the bone-tendon junction of the rotator cuff insertions. Typically, two sutures are passed through the subscapularis (lesser tuberosity), two through the supraspinatus (superior greater tuberosity), and two through the infraspinatus/teres minor (posterior greater tuberosity).

TECH FIG 2 • Heavy nonabsorbable sutures are placed at the bone-tendon junction of the subscapularis, supraspinatus, and infraspinatus to control the tuberosities.
Only after the tuberosities are securely tagged and mobilized do we proceed to extract the articular segment. The head is gently grasped with a tenaculum or towel clip and removed. It is preserved on the back table to be measured; its radius of curvature and thickness will guide the selection of the prosthetic head size.
Humeral Shaft Preparation and Trialing
Attention is now turned to the humeral diaphysis. The shaft is elevated out of the wound using a bone hook or a blunt elevator. The medullary canal is sequentially broached or reamed according to the specific implant system's protocol. It is critical to avoid over-reaming, as the osteoporotic cortical bone is easily perforated or fractured.
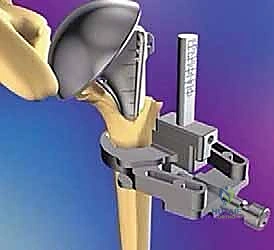
TECH FIG 3 • The humeral canal is prepared with sequential broaches. The trial stem is inserted, and height and version are assessed.
Once the canal is prepared, a trial stem is inserted. Determining the correct height and version of the prosthesis is the most technically demanding aspect of the procedure. Version is typically set at 20 to 30 degrees of retroversion. This can be assessed by referencing the epicondylar axis of the elbow (using a dedicated alignment jig) or by aligning the lateral fin of the prosthesis just posterior to the bicipital groove.
Height is determined using multiple data points: the preoperative templating of the pectoralis major distance (typically 5.6 cm from the upper border of the pec major to the top of the head), the "gothic arch" alignment of the medial calcar, and the tension of the soft tissues when the trial head is reduced. With the trial components in place and reduced, the tagged tuberosities are pulled around the prosthesis. They should meet anatomically below the articular margin without excessive tension. If they do not reach, the prosthesis is likely too proud.
Tuberosity Reconstruction and Biomechanical Restoration
Once the optimal stem size, height, and version are confirmed, the canal is thoroughly irrigated with pulsatile lavage, brushed, and dried. A restrictive cement plug is placed distally. Polymethylmethacrylate (PMMA) bone cement is introduced in a retrograde fashion using a cement gun.
TECH FIG 4 • The definitive stem is cemented in place. Note the heavy sutures passed through the fin of the prosthesis prior to cementation.
Crucially, before inserting the final stem, heavy cerclage sutures must be passed through the holes in the proximal fin of the prosthesis. These sutures will form the foundation of the tuberosity repair. The definitive stem is inserted into the cement mantle, meticulously maintaining the predetermined height and version until the cement fully polymerizes.
The final, and most vital, step is the tuberosity reconstruction. The previously placed tagging sutures and the sutures passed through the prosthetic fin are used to create a biomechanically rigid construct. We employ a combination of vertical tension-band sutures and horizontal cerclage sutures. The horizontal sutures wrap around both tuberosities, compressing them against the prosthetic stem and each other. The vertical sutures pass through the rotator cuff insertions, down through the holes in the prosthetic fin or the humeral shaft, and tie back on themselves, neutralizing the superior pull of the supraspinatus and deltoid.
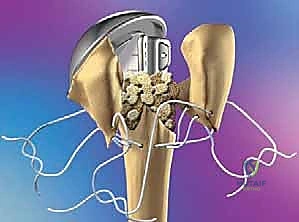
TECH FIG 5 • Final tuberosity reconstruction utilizing a combination of vertical tension-band and horizontal cerclage sutures, securing the tuberosities to each other and the shaft.
Bone graft harvested from the excised humeral head is meticulously packed into the interstices between the tuberosities and the shaft to promote osteoinduction and osseous union. The wound is copiously irrigated, a closed-suction drain is placed, and the deltopectoral interval is loosely approximated before layered closure of the subcutaneous tissue and skin.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, proximal humerus hemiarthroplasty carries a substantial complication profile, largely driven by the precarious nature of tuberosity healing in osteoporotic bone. The surgeon must be prepared to identify and manage these complications aggressively.
Tuberosity Failure and Malunion
Tuberosity nonunion, malunion, or resorption is the "Achilles heel" of this operation. Historically, failure rates have been reported as high as 30% to 50% in older literature, though modern fracture-specific stems and advanced suturing techniques have improved these numbers. If the greater tuberosity fails to heal or migrates superiorly, the patient will experience profound weakness in abduction and external rotation, often resulting in a pseudoparalytic shoulder.
Superior migration of the prosthesis is a direct consequence of tuberosity failure. Without the compressive force of the rotator cuff, the unopposed deltoid pulls the humerus proximally, leading to painful impingement against the acromion and progressive erosion of the coracoacromial arch.
Tabular Summary of Complications and Salvage Strategies
| Complication | Estimated Incidence | Pathophysiology & Clinical Presentation | Salvage Strategy / Management |
|---|---|---|---|
| Tuberosity Nonunion / Resorption | 15% - 40% | Failure of osseous integration; superior migration of prosthesis; pseudoparalysis. | Conversion to Reverse Total Shoulder Arthroplasty (RTSA). |
| Glenoid Erosion | 10% - 20% (Long-term) | Articular mismatch or over-tensioning; painful crepitus and progressive stiffness. | Conversion to anatomic Total Shoulder Arthroplasty (if cuff intact) or RTSA. |
| Shoulder Stiffness / Adhesive Capsulitis | 10% - 15% | Over-tensioning of tuberosities or inadequate rehabilitation; severe restriction of active and passive ROM. | Aggressive physical therapy; arthroscopic capsular release if refractory. |
| Nerve Injury (Axillary/Musculocutaneous) | 1% - 5% | Iatrogenic traction or direct laceration; deltoid or biceps weakness/atrophy. | Observation and EMG at 3 months; nerve exploration/grafting if no recovery. |
| Prosthetic Joint Infection (PJI) | 1% - 2% | Hematogenous seeding or intraoperative contamination; pain, erythema, elevated CRP/ESR. | Irrigation and debridement (acute); two-stage revision with antibiotic spacer (chronic). |
Phased Post-Operative Rehabilitation Protocols
The surgical intervention is only the first half of the treatment paradigm. The postoperative rehabilitation protocol must strike a delicate, often contradictory, balance: it must protect the fragile tuberosity repair from disruptive muscular forces while simultaneously preventing catastrophic adhesive capsulitis.
Phase I: Immediate Postoperative Protection (Weeks 0 to 6)
Immediately following surgery, the operative arm is immobilized in a sling or abduction orthosis. The primary goal of Phase I is the protection of the tuberosity reconstruction to allow for initial soft-tissue and early osseous healing.
During this phase, active range of motion of the shoulder is strictly prohibited. The patient is instructed on active motion of the elbow, wrist, and hand to prevent distal edema and stiffness. Physical therapy initiates gentle, supine, passive forward elevation and passive external rotation. External rotation is strictly limited to the safe zone determined intraoperatively (typically 20 to 30 degrees) to prevent tension failure of the lesser tuberosity repair.
Phase II and III: Active Motion and Strengthening (Weeks 6 to 12+)
At approximately 6 weeks postoperative, assuming radiographic evidence of early tuberosity consolidation and clinical stability, the sling is discontinued, and Phase II begins. This phase transitions the patient from passive motion to active-assisted range of motion (AAROM). Pulle
Detailed Chapters & Topics
Dive deeper into specialized chapters regarding hemiarthroplasty-for-proximal-humerus-fractures