Proximal Row Carpectomy: An Intraoperative Masterclass for Wrist Degeneration

Key Takeaway
Join us in the operating theater for a comprehensive masterclass on Proximal Row Carpectomy (PRC). This guide details patient selection, meticulous surgical technique, critical anatomical considerations, and management of potential pitfalls. We'll navigate each step from incision to closure, ensuring fellows gain a deep understanding of this essential procedure for wrist degeneration, emphasizing precision and optimal patient outcomes.
Comprehensive Introduction and Patho-Epidemiology
Proximal row carpectomy (PRC) represents a cornerstone in the armamentarium of the modern orthopedic hand and upper extremity surgeon. Originally described by Stamm in 1944, this procedure was conceptualized to manage complex, debilitating wrist arthrosis by converting a multi-articulated, pathologically stiff, and painful joint into a simplified, functional hinge. By excising the scaphoid, lunate, and triquetrum, the surgeon effectively removes the intercalated segment of the wrist, allowing the capitate head to articulate directly within the lunate fossa of the distal radius. This profound anatomical alteration successfully mitigates the mechanical grinding of arthritic carpal facets while preserving a highly functional, albeit reduced, arc of motion.
The patho-epidemiology driving the need for a PRC typically originates from a predictable cascade of carpal instability and subsequent articular cartilage degradation. The most common etiologies include Scapholunate Advanced Collapse (SLAC) and Scaphoid Nonunion Advanced Collapse (SNAC). In the SLAC wrist, an untreated scapholunate ligament rupture leads to rotary subluxation of the scaphoid, resulting in point-loading and progressive arthrosis starting at the radial styloid, progressing to the entire radioscaphoid joint, and eventually involving the capitolunate articulation. The radiolunate joint is characteristically spared due to the concentric, spherical nature of its articulation, which forms the fundamental pathophysiological rationale for performing a PRC.
Biomechanically, the normal wrist functions through a complex interaction between the proximal and distal carpal rows, stabilized by intrinsic and extrinsic ligamentous networks. When advanced degeneration occurs, this intricate kinematic chain becomes a source of intractable nociception. PRC fundamentally alters wrist biomechanics by shortening the carpus and creating a neojoint. While the radius of curvature of the capitate head is smaller than that of the lunate fossa—creating an initial state of incongruity and point-contact loading—clinical and biomechanical studies have demonstrated that this neojoint undergoes adaptive remodeling. Over time, fibrocartilaginous metaplasia and bony remodeling often lead to a more congruous articulation, allowing for durable load transfer.
The overarching goals of a proximal row carpectomy are threefold: the reliable eradication of radiocarpal and midcarpal pain, the preservation of functional wrist mobility, and the maintenance of adequate grip strength to perform activities of daily living. Unlike total wrist arthrodesis, which sacrifices all radiocarpal and midcarpal motion for absolute pain relief and stability, PRC offers a motion-sparing alternative. Furthermore, when compared to limited intercarpal fusions (such as the four-corner arthrodesis), PRC avoids the complications associated with hardware, nonunion, and prolonged immobilization, making it an elegant, soft-tissue-driven solution for advanced wrist degeneration.
Detailed Surgical Anatomy and Biomechanics
A profound mastery of dorsal wrist anatomy and carpal biomechanics is non-negotiable for the safe and effective execution of a proximal row carpectomy. The surgeon must navigate a complex, multi-layered anatomical landscape, respecting neurovascular boundaries while executing precise osteological resections.
The osteology of the wrist is traditionally divided into the proximal carpal row (scaphoid, lunate, triquetrum) and the distal carpal row (trapezium, trapezoid, capitate, hamate). The proximal row acts as an intercalated segment, lacking direct tendinous insertions, and its motion is entirely dictated by the mechanical forces exerted by the surrounding articular contours and ligamentous constraints. During a PRC, the excision of this entire row mandates that the capitate—the keystone of the distal row—migrates proximally to articulate with the lunate facet of the distal radius. The surgeon must acutely recognize that the proximal articular surface of the capitate is not perfectly spherical; it possesses a complex geometry that must be carefully seated within the lunate fossa to optimize the contact area of the newly formed radiocapitate articulation.
Ligamentous preservation is arguably the most critical technical aspect of this procedure. The stability of the post-PRC wrist relies entirely on the integrity of the volar extrinsic ligaments. The radioscaphocapitate (RSC) ligament is of paramount importance. Originating from the volar aspect of the radial styloid, it crosses the waist of the scaphoid to insert onto the body of the capitate. During the excision of the scaphoid and the performance of a radial styloidectomy, iatrogenic transection or avulsion of the RSC ligament will inevitably lead to catastrophic ulnar translation of the carpus. Similarly, the long radiolunate (LRL) and short radiolunate (SRL) ligaments must be respected during the enucleation of the lunate to maintain the volar capsular floor.
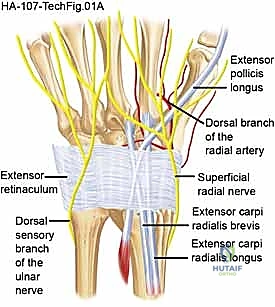
Neurovascular structures demand meticulous attention during the dorsal approach. The posterior interosseous nerve (PIN), a terminal motor branch of the radial nerve, provides critical nociceptive innervation to the dorsal wrist capsule. It is reliably located on the radial floor of the fourth dorsal compartment, intimately associated with the posterior interosseous artery. A routine neurectomy of the PIN is performed during PRC to maximize postoperative pain relief. Superficially, the surgeon must protect the dorsal sensory branches of the radial nerve radially, and the dorsal cutaneous branch of the ulnar nerve ulnarly, by maintaining thick, full-thickness fasciocutaneous flaps during the initial exposure.
The muscular and tendinous anatomy dictates our surgical windows. The dorsal wrist is organized into six extensor compartments beneath the extensor retinaculum. The standard approach for a PRC utilizes the interval between the third compartment (Extensor Pollicis Longus - EPL) and the fourth compartment (Extensor Digitorum Communis - EDC, and Extensor Indicis Proprius - EIP). By incising the retinaculum over the third compartment and transposing the EPL radially, the surgeon gains an extensile view of the dorsal wrist capsule. Retraction of the second compartment (ECRL, ECRB) radially and the fourth compartment ulnarly provides the necessary exposure to elevate a broad, distally based capsular flap, granting unhindered access to the radiocarpal and midcarpal joints.
Exhaustive Indications and Contraindications
The decision to proceed with a proximal row carpectomy hinges on a rigorous evaluation of the patient's pathology, anatomical preservation of specific articular surfaces, and the patient's functional demands. Patient selection is the ultimate determinant of long-term surgical success.
The primary indications for PRC encompass a spectrum of conditions leading to carpal collapse, provided the lunate fossa of the radius and the proximal head of the capitate remain structurally intact. Scapholunate Advanced Collapse (SLAC) and Scaphoid Nonunion Advanced Collapse (SNAC) wrists in Stages I and II are classic indications. In these stages, arthrosis is confined to the radioscaphoid articulation (and the scaphocapitate articulation in SNAC II), while the capitolunate and radiolunate joints are spared. Kienböck disease, particularly in advanced Stages IIIa, IIIb, and IV, where lunate fragmentation and carpal collapse have occurred, is another robust indication. Furthermore, PRC is highly effective for chronic, irreducible perilunate dislocations, Preiser disease (idiopathic avascular necrosis of the scaphoid), and severe spastic or congenital wrist flexion contractures where joint resection is necessary to achieve a plantigrade hand.

Absolute contraindications to PRC are primarily anatomical. The procedure is strictly contraindicated if there is advanced, full-thickness eburnation or degenerative change at either the proximal articular surface of the capitate or the lunate facet of the distal radius. Performing a PRC in the presence of capitate head arthrosis will predictably result in persistent, severe radiocapitate pain and early clinical failure. Additionally, pre-existing ulnar carpal translation or severe incompetence of the volar radioscaphocapitate (RSC) ligament is an absolute contraindication, as the removal of the proximal row will exacerbate this instability, leading to the capitate sliding off the ulnar inclination of the radius. Active, uncontrolled inflammatory arthropathies (e.g., florid Rheumatoid Arthritis) are also contraindications due to the progressive destruction of the capsuloligamentous constraints required for post-PRC stability.
Relative contraindications revolve around patient demographics and occupational demands. The use of PRC in young, highly active patients (typically under 35 years of age) or heavy manual laborers remains a subject of intense academic debate. While many young patients achieve excellent pain relief and functional motion, the long-term durability of the radiocapitate neojoint under repetitive, high-load physiological stress is questionable, with some studies suggesting a higher rate of conversion to total wrist arthrodesis in this demographic. In such cases, alternative motion-sparing procedures, such as a four-corner arthrodesis, may be considered, though the literature comparing long-term survivorship between the two procedures in heavy laborers remains equivocal.
Indications and Contraindications Summary
| Category | Specific Conditions | Rationale / Clinical Note |
|---|---|---|
| Primary Indications | SLAC Wrist (Stages I, II) | Radioscaphoid arthrosis with spared capitolunate joint. |
| SNAC Wrist (Stages I, II) | Spared radiolunate and proximal capitate articular surfaces. | |
| Kienböck Disease (Stages III, IV) | Lunate collapse/fragmentation with carpal instability. | |
| Chronic Perilunate Dislocation | Irreducible or highly arthritic midcarpal/radiocarpal joints. | |
| Severe Wrist Contractures | Salvage for spasticity to achieve a neutral wrist position. | |
| Absolute Contraindications | Capitate Head Arthrosis | Will lead to painful radiocapitate bone-on-bone articulation. |
| Lunate Facet Arthrosis | compromises the foundation of the new radiocapitate joint. | |
| Ulnar Carpal Translation | Indicates RSC ligament incompetence; PRC will worsen instability. | |
| Active Inflammatory Arthritis | Ongoing ligamentous destruction precludes a stable neojoint. | |
| Relative Contraindications | Heavy Manual Laborers | High mechanical stress may accelerate radiocapitate wear. |
| Young Age (< 35 years) | Concerns regarding decades-long durability of the neojoint. |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative preparation is the bedrock of a smooth, complication-free proximal row carpectomy. This phase requires a synthesis of clinical examination findings, advanced imaging interpretation, and strategic intraoperative contingency planning.
Clinical evaluation must precisely document the patient's preoperative range of motion, grip strength (measured with a Jamar dynamometer), and specific locations of point tenderness. This establishes a baseline for postoperative comparison and helps manage patient expectations. The surgeon must explicitly counsel the patient that while pain relief is highly predictable, they will likely lose a percentage of their preoperative arc of motion, and grip strength will typically plateau at 60% to 80% of the contralateral, unaffected limb.
Radiographic evaluation is paramount. Standard posteroanterior (PA), lateral, and scaphoid-specific oblique radiographs are mandatory. The surgeon must scrutinize the joint spaces. On the PA view, assess the radioscaphoid joint for sclerosis, osteophyte formation, and joint space narrowing. Crucially, evaluate the capitolunate and radiolunate joints. If there is any radiographic ambiguity regarding the integrity of the capitate head or the lunate fossa, advanced imaging is required. A non-contrast CT scan with sagittal and coronal reconstructions provides unparalleled osseous detail to rule out subtle capitate flattening or subchondral cysts. While MRI is excellent for diagnosing avascular necrosis (e.g., Kienböck's), it is less reliable than CT or direct intraoperative visualization for assessing the exact thickness and viability of the articular cartilage on the capitate head.

Templating and contingency planning are critical. The surgeon must enter the operating theater prepared to abandon the PRC if direct intraoperative inspection reveals unacceptable capitate or lunate facet arthrosis. Therefore, the patient must be preoperatively consented for both a proximal row carpectomy and a backup procedure, typically a four-corner arthrodesis (if the lunate facet is pristine but the midcarpal joint is destroyed) or a total wrist arthrodesis (if pan-carpal arthrosis is present). Ensure that the necessary hardware for these alternative procedures (e.g., circular plates, headless compression screws, dorsal spanning plates) is available in the room.
For the procedure, the patient is positioned supine on the operating table. The operative extremity is extended onto a radiolucent hand table. A well-padded, non-sterile pneumatic tourniquet is applied to the proximal brachium. Regional anesthesia, typically an ultrasound-guided supraclavicular or axillary brachial plexus block, is highly recommended. This provides excellent intraoperative muscle relaxation and profound postoperative analgesia, minimizing the need for systemic opioids. The block is often supplemented with general anesthesia or deep intravenous sedation to ensure patient comfort during the procedure. The arm is prepped and draped in a standard sterile fashion, and the limb is exsanguinated with an Esmarch bandage before inflating the tourniquet to 250 mmHg.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of a proximal row carpectomy demands a delicate balance between aggressive osseous resection and meticulous soft-tissue preservation.
The procedure begins with a dorsal longitudinal incision, approximately 6 to 8 centimeters in length, centered over Lister's tubercle. The skin is incised with a #10 blade. Subcutaneous dissection is performed sharply, elevating thick, full-thickness fasciocutaneous flaps radially and ulnarly. It is imperative to stay directly on the extensor retinaculum during this elevation to avoid devastating injury to the superficial sensory branches of the radial nerve and the dorsal cutaneous branch of the ulnar nerve. Once the retinaculum is exposed, attention is turned to the proximal, radial aspect of the incision. The posterior interosseous nerve (PIN) is identified on the floor of the fourth dorsal compartment. A 1 to 2-centimeter segment of the PIN is sharply resected, and the accompanying posterior interosseous artery is coagulated with bipolar electrocautery to perform a thorough dorsal denervation.

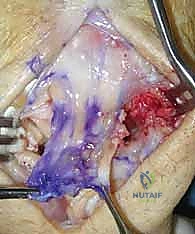
Next, the extensor retinaculum is addressed. A longitudinal incision is made directly over the third dorsal compartment. The Extensor Pollicis Longus (EPL) tendon is mobilized and transposed radially into the subcutaneous tissues. The retinacular incision is then extended proximally and distally. The second compartment tendons (ECRL, ECRB) are retracted radially, and the fourth compartment tendons (EDC, EIP) are retracted ulnarly. This exposes the dorsal wrist capsule. A ligament-sparing capsulotomy, often utilizing a distally based, inverted-U or T-shaped flap (Berger's flap), is meticulously elevated. The capsular flap must be robust, as it will be securely repaired at the conclusion of the procedure to prevent dorsal subluxation of the capitate.
With the radiocarpal and midcarpal joints exposed, the critical step of articular inspection occurs. The surgeon must directly visualize and probe the cartilage of the capitate head and the lunate fossa of the radius. If full-thickness cartilage loss is identified here, the PRC must be aborted in favor of a salvage arthrodesis. Assuming the cartilage is pristine, the carpectomy commences.

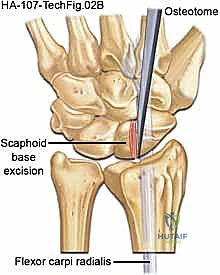
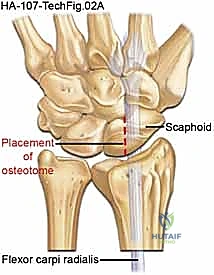
The excision of the proximal row can be performed en bloc or piecemeal. Piecemeal excision is often preferred to minimize traction on the vital volar ligaments. The scaphoid is typically addressed first. It can be sectioned at its waist using a sharp osteotome or an oscillating saw. The proximal and distal poles are then carefully enucleated using a rongeur and a Freer elevator. Extreme caution must be exercised when dissecting the volar aspect of the scaphoid to avoid violating the radioscaphocapitate (RSC) ligament.
Following the scaphoid, the lunate is excised. A threaded K-wire or a specialized corkscrew can be inserted into the lunate to act as a joystick, providing traction while the strong volar short radiolunate (SRL) and long radiolunate (LRL) ligaments are sharply released directly off the bone. Finally, the triquetrum is excised in a similar fashion, taking care to preserve the integrity of the triangular fibrocartilage complex (TFCC) ulnarly.

Once the proximal row is entirely removed, a radial styloidectomy is routinely performed. This prevents painful impingement between the base of the trapezium and the radial styloid during radial deviation. Using an oscillating saw or a sharp osteotome, an oblique cut is made, removing the distal 3 to 5 millimeters of the radial styloid. The angle of the cut is critical; it must not compromise the origin of the RSC ligament, which attaches to the volar base of the styloid.
The wound is copiously irrigated to remove all osteochondral debris. The capitate is then manually reduced into the lunate fossa. Fluoroscopy is utilized to confirm concentric reduction of the radiocapitate joint and to ensure no bony impingement occurs during a full arc of passive flexion, extension, and radioulnar deviation. Routine K-wire fixation across the radiocapitate joint is generally unnecessary unless there is profound soft-tissue instability, as the intact volar ligaments and the repaired dorsal capsule provide adequate stability.
Closure begins with the meticulous, water-tight repair of the dorsal capsular flap using non-absorbable or slowly absorbable braided sutures (e.g., 2-0 or 3-0 Ethibond or Vicryl). The extensor retinaculum is repaired loosely over the fourth compartment to prevent bowstringing, leaving the EPL transposed subcutaneously. The skin is closed with a running subcuticular suture or interrupted nylons. A bulky, sterile compressive dressing is applied, and the wrist is immobilized in a well-padded volar splint in approximately 10 to 15 degrees of extension.

Complications, Incidence Rates, and Salvage Management
While proximal row carpectomy is a highly reliable procedure, it is not without potential complications. The surgeon must be acutely aware of these risks, their incidence, and the appropriate salvage pathways.
The most frequently discussed long-term complication is progressive radiocapitate arthrosis. Because the capitate head has a smaller radius of curvature than the lunate fossa, the initial contact mechanics involve high-stress point loading. Over decades, this predictably leads to radiographic narrowing of the radiocapitate space. Interestingly, numerous long-term outcome studies have demonstrated a profound clinical-radiographic mismatch; while up to 60-70% of patients may exhibit radiographic signs of arthrosis at 10 to 15 years post-operatively, the vast majority remain entirely asymptomatic and functionally satisfied. Therefore, radiographic arthrosis alone, in the absence of clinical pain, does not warrant surgical intervention.
Weakness and stiffness are expected outcomes rather than true complications, but failure to manage patient expectations preoperatively can lead to dissatisfaction. Patients typically achieve a functional arc of motion (approximately 60-70 degrees of total flexion-extension) and a grip strength that is 60-80% of the contralateral side. However, severe, debilitating stiffness can occur, often secondary to prolonged immobilization, inadequate postoperative rehabilitation, or undiagnosed complex regional pain syndrome (CRPS).
A catastrophic mechanical complication is ulnar translation of the carpus. This occurs when the volar radioscaphocapitate (RSC) ligament is iatrogenically transected during the scaphoid excision or radial styloidectomy. Without the tethering effect of the RSC ligament, the capitate slides down the ulnar inclination of the distal radius, leading to profound instability, severe pain, and rapid failure of the neojoint.
When a PRC fails—whether due to progressive, painful radiocapitate arthrosis, ulnar translation, or deep infection—the gold standard salvage procedure is a Total Wrist Arthrodesis (TWA). TWA provides reliable, definitive pain relief and stability, albeit at the complete sacrifice of radiocarpal motion. In older, lower-demand patients, a total wrist arthroplasty may be considered as a motion-sparing salvage option, though the complication rates and lifting restrictions associated with arthroplasty must be carefully weighed.
Complications and Salvage Management Summary
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Radiocapitate Arthrosis | High (Radiographic: 50-70% at 10 yrs) | Biomechanical mismatch, heavy labor. | Observation if asymptomatic. Total Wrist Arthrodesis (TWA) if painful. |
| Ulnar Carpal Translation | Low (< 5%) | Iatrogenic injury to the RSC ligament. | Early: Ligament repair/reconstruction. Late: Total Wrist Arthrodesis. |
| Severe Stiffness / CRPS | Moderate (5-15%) | Prolonged immobilization, poor pain |
