Proximal Realignment: Masterclass in Medial Patellofemoral Ligament Repair
Key Takeaway
This masterclass provides an exhaustive, real-time walkthrough of Medial Patellofemoral Ligament (MPFL) repair. We cover comprehensive surgical anatomy, meticulous preoperative planning, and granular, step-by-step intraoperative execution from a surgeon's perspective. Learn critical pearls, pitfalls, and post-operative management for patellar instability, ensuring optimal outcomes for your patients.
Comprehensive Introduction and Patho-Epidemiology
Patellar instability represents a complex, multifactorial biomechanical challenge that demands a rigorous, anatomically precise approach from the orthopedic surgeon. Today, we are addressing a highly specific and critical intervention: the primary repair of the Medial Patellofemoral Ligament (MPFL) at its patellar insertion. While MPFL reconstruction utilizing autograft or allograft tissue has become the gold standard for chronic, recurrent instability, there remains a vital, distinct role for primary repair in the acute or subacute setting. This procedure is specifically indicated for patients experiencing recurrent patellar dislocations or a severe first-time dislocation where an acute, amenable avulsion tear pattern is identified at the patellar footprint. Restoring the native ligamentous anatomy before chronic attenuation occurs can effectively re-establish patellofemoral kinematics without the morbidity associated with graft harvest.
To truly master this procedure, one must first understand the underlying pathophysiology of patellofemoral instability. In the vast majority of lateral patellar dislocations, there is an obligatory failure of the medial retinacular restraints. The MPFL is the undisputed primary soft-tissue restraint against lateral patellar displacement, contributing between 50% and 60% of the total medial restraining force during the critical early degrees of knee flexion (0 to 30 degrees). When this ligament is compromised—whether through a midsubstance rupture, a femoral avulsion, or, as in our focus today, a patellar avulsion—the patella's lateral mobility increases drastically beyond normal physiological limits. Our surgical objective is not merely to tether the patella, but to precisely restore the functional competency and isometric tension of this native check-rein.
The natural history and epidemiology of patellar dislocation underscore the necessity for decisive intervention. Literature demonstrates that a first-time dislocator managed non-operatively faces an approximate 17% to 44% chance of redislocation. However, for those who experience a second dislocation, the risk of recurrent instability soars to greater than 50%, often accompanied by progressive damage to the medial patellar facet and lateral trochlear cartilage. Patient demographics play a massive role; young, skeletally immature athletes, particularly females with underlying generalized ligamentous laxity, are at the highest risk. The presence of osteochondral shear fractures at the time of the initial dislocation further mandates early surgical exploration, providing an opportunistic window to perform a primary MPFL repair concurrently.
Historically, the orthopedic community oscillated between conservative management and non-anatomic medial reefing procedures for acute dislocations. However, the paradigm has shifted dramatically toward anatomic, pathology-specific interventions. By identifying the exact location of the MPFL tear via high-resolution magnetic resonance imaging (MRI), surgeons can now tailor their approach. A discrete avulsion off the proximal two-thirds of the medial patella, with robust, unretracted ligamentous tissue, presents the ideal scenario for primary repair. This masterclass will delineate the precise steps required to execute this repair, ensuring anatomic restoration, preventing over-constraint, and optimizing long-term functional outcomes.
Detailed Surgical Anatomy and Biomechanics
The stability of the patellofemoral joint relies on an intricate interplay between dynamic muscular forces, static ligamentous restraints, and bony architecture. The main osseous stabilizer is the congruence between the patella and the trochlear groove. However, in a significant proportion of instability patients, trochlear dysplasia flattens this groove, shifting a disproportionate mechanical burden onto the medial soft tissues. Even in the presence of a perfectly normal, deeply sulcated trochlea, an isolated deficiency of the MPFL is sufficient to cause symptomatic, recurrent lateral instability. Understanding the exact topography of these structures is the absolute foundation of successful surgical intervention.

The MPFL is an extra-articular, fascial band residing within Layer 2 of the medial knee, as classically described by Warren and Marshall. It is meticulously nestled between the superficial medial retinaculum (Layer 1) and the deeper joint capsule (Layer 3). The distal, oblique fibers of the vastus medialis obliquus (VMO) muscle are intimately associated with the MPFL. The VMO tendon lies superficially and anteriorly, dynamically inserting onto the anterior third of the MPFL and the superomedial pole of the patella. This dynamic-static relationship means that VMO contraction actively tensions the MPFL, pulling the patella medially and seating it firmly within the trochlea during early flexion.
The macroscopic dimensions of the native MPFL are highly consistent across the adult population. It measures approximately 58 mm in length, with an average width of 12 mm and a remarkably thin cross-sectional thickness of roughly 0.44 mm at its midpoint. From its femoral origin, the ligament fans out anteriorly, broadening as it approaches the patella. Its insertion footprint covers the proximal two-thirds of the patella's medial margin, transitioning from a distinct ligamentous band into a broader retinacular expansion. Recognizing this broad patellar footprint is critical; a point-to-point repair using a single anchor often fails to recreate the native biomechanics, necessitating a dual-anchor technique to restore the broad insertion.
The femoral attachment is a critical anatomical landmark, dictating the isometric behavior of the ligament. The origin is located posterosuperior to the medial femoral epicondyle and just distal to the adductor tubercle. Radiographically, this is defined by Schöttle's point. Specifically, the center of its anterior edge lies approximately 9.5 mm proximal and 5.0 mm posterior to the center of the medial femoral epicondyle. While our focus today is a patellar-sided repair, understanding the femoral origin is paramount for assessing overall tissue tension. Furthermore, surgeons must maintain strict vigilance regarding neurovascular structures. The saphenous nerve and its infrapatellar branch cross the medial knee superficially and are highly vulnerable during skin incision and dissection. Deep to the VMO and superior to the MPFL lies the descending genicular artery, which requires meticulous hemostasis to prevent postoperative hematoma.
Exhaustive Indications and Contraindications
Patient selection is the absolute crucible of success in primary MPFL repair. Not every dislocating patella requires surgery, and certainly, not every torn MPFL is amenable to primary repair. The ideal candidate is a patient presenting with acute or subacute recurrent lateral patellar dislocations (or a severe primary dislocation with an osteochondral fracture) where an MRI confirms a discrete, full-thickness avulsion of the MPFL from its patellar insertion. The tissue must be of high quality, without significant midsubstance comminution, chronic attenuation, or severe retraction. The procedure is most successful in patients who have failed a rigorous trial of non-operative management, including dedicated VMO strengthening and core stabilization, yet continue to experience mechanical instability.
Indications vs Contraindications for Primary MPFL Repair
| Parameter | Indications for Primary Patellar-Sided Repair | Absolute/Relative Contraindications |
|---|---|---|
| Chronicity of Injury | Acute or subacute (< 3-4 months from injury) allowing mobilization of native tissue. | Chronic instability (> 6 months) with attenuated, scarred, or absent native MPFL tissue. |
| Tear Location | Discrete avulsion at the patellar footprint (proximal 2/3 of medial margin). | Midsubstance ruptures, femoral avulsions (require different approach), or diffuse retinacular tearing. |
| Tissue Quality | Robust, thick ligamentous stump capable of holding high-tensile suture material. | Frayed, "mop-end" tissue, or underlying connective tissue disorders (e.g., Ehlers-Danlos, Marfan syndrome). |
| Bony Anatomy (Trochlea) | Normal trochlea or mild dysplasia (Dejour Type A). | Severe trochlear dysplasia (Dejour Type B, C, D) requiring concurrent or isolated trochleoplasty. |
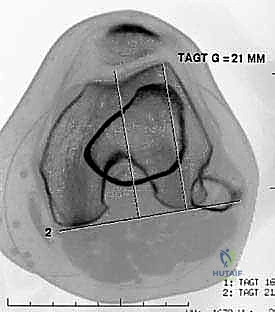
| Bony Anatomy (Alignment) | Normal TT-TG distance (< 15 mm), normal patellar height (Caton-Deschamps < 1.2). | Severe TT-TG offset (> 20 mm) or severe patella alta requiring concurrent tibial tubercle osteotomy (TTO). |
Differentiating between the need for a primary repair versus a full reconstruction requires astute clinical judgment. If the surgeon explores the medial retinaculum and discovers that the native MPFL is structurally inadequate to provide a robust check-rein—even if the MRI suggested a clean avulsion—the surgeon must be prepared to seamlessly pivot to an MPFL reconstruction using autograft (e.g., gracilis) or allograft. Primary repair relies entirely on the healing capacity of the native tissue against the decorticated patellar bone; if the tissue is compromised, the repair will inevitably stretch out, leading to recurrent instability and a frustrated patient.
Contraindications must be rigorously respected to avoid catastrophic failure. Severe underlying bony malalignment is the most common reason for soft-tissue repair failure. If a patient possesses a Tibial Tubercle-Trochlear Groove (TT-TG) distance exceeding 20 mm, an isolated MPFL repair will be subjected to insurmountable lateralizing vectors and will fail. Such patients require a concurrent medializing Tibial Tubercle Osteotomy (TTO). Similarly, profound patella alta (Caton-Deschamps ratio > 1.2) prevents the patella from engaging the trochlea during early flexion, rendering the MPFL repair useless against lateral forces. In cases of severe bony deformity, the soft tissue repair is secondary to correcting the osseous architecture.
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the roadmap to a successful surgical outcome. The process begins with a meticulous review of high-quality imaging. Standard plain radiographs are mandatory and must include a standing anteroposterior (AP) view, a true lateral view taken at exactly 30 degrees of knee flexion, and an axial (Merchant or sunrise) view at 30 to 45 degrees of flexion. On the true lateral radiograph, we meticulously assess for trochlear dysplasia by looking for the "crossing sign," where the floor of the trochlea intersects the anterior borders of the femoral condyles.
We also quantify the trochlear prominence; a measurement of 3 mm or greater is highly indicative of dysplasia that may compromise isolated soft-tissue procedures.
The lateral view is also utilized to calculate the Caton-Deschamps ratio to rule out significant patella alta.
Advanced cross-sectional imaging, specifically MRI and occasionally CT, is indispensable. Axial CT or MRI is used to accurately measure the TT-TG offset, ensuring it falls within the acceptable range (< 15-20 mm) for an isolated MPFL procedure.
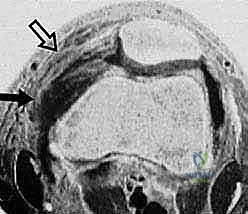
However, MRI is the primary modality for evaluating the soft-tissue envelope. We scrutinize the T2-weighted axial and coronal sequences to identify the exact location of the MPFL failure. We look for the classic "wavy" appearance of a detached ligament, surrounding edema, and the presence of a distinct stump at the patellar margin.
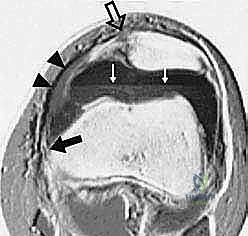
Crucially, the MRI must be reviewed for concomitant articular cartilage damage; osteochondral loose bodies originating from the medial patellar facet or the lateral femoral condyle are common and must be addressed concurrently.
Once in the operating theater, before the first incision is made, an Examination Under Anesthesia (EUA) is a non-negotiable step. With the patient fully relaxed, the surgeon can accurately assess the degree of lateral patellar translation, comparing it to the contralateral limb. We evaluate the patellar glide into quadrants; translation of 3 or more quadrants laterally without a solid endpoint confirms gross MPFL incompetence. We also assess for the "J-sign" (abrupt lateral deviation of the patella as it exits the trochlea in terminal extension) and perform the check-rein test to evaluate the integrity of the medial restraints.
Patient positioning is critical for optimal exposure and dynamic intraoperative assessment. The patient is placed supine on a standard operating table. While a leg holder is frequently used for arthroscopy, for an open MPFL repair, it is often advantageous to have the leg draped freely to allow unencumbered evaluation of patellar tracking through a full arc of motion. A proximal thigh tourniquet is applied over generous padding. Fluoroscopy must be available in the room; while not strictly necessary for identifying the patellar footprint, it is an invaluable tool for verifying anchor trajectory and dynamically assessing patellar reduction if any doubt exists. The entire lower extremity is prepped and draped in a standard sterile fashion.
Step-by-Step Surgical Approach and Fixation Technique
The surgical approach begins with a meticulously planned incision. A longitudinal incision, approximately 4 to 6 centimeters in length, is made over the medial border of the patella, centered over the proximal two-thirds where the MPFL natively inserts. Alternatively, if a diagnostic arthroscopy was performed, the medial portal can sometimes be incorporated into the exposure. Sharp dissection is carried down through the subcutaneous tissues. Extreme care must be taken during this superficial dissection to identify and protect the terminal branches of the saphenous nerve, particularly the infrapatellar branch, which courses transversely across the medial retinaculum. Retraction should be gentle to avoid neuropraxia.
Upon reaching the superficial fascia, the surgeon develops the interval between Layer 1 and Layer 2. The fascia overlying the VMO is identified, and the distal muscular fibers are traced to their insertion on the medial patella and the underlying MPFL. The avulsed edge of the MPFL is typically identified by a localized hematoma or organized scar tissue in the subacute setting.
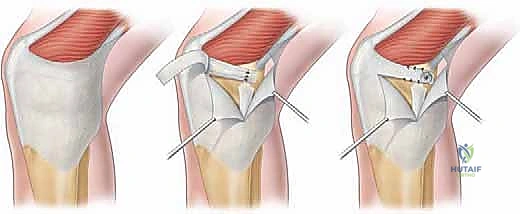

The retinaculum is incised longitudinally, slightly medial to the patellar border, to expose the torn edge of the ligament. The stump is carefully mobilized, freeing it from underlying capsular adhesions to ensure it can be advanced to the patellar footprint without excessive tension. The quality of the tissue is reassessed at this stage; it must be robust enough to hold high-strength suture.
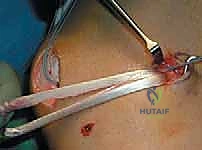
Preparation of the patellar bed is a critical step for biologic healing. The native insertion site on the proximal two-thirds of the medial patellar facet is exposed. Using a curette, rongeur, or a high-speed burr, the medial cortical margin is lightly decorticated down to bleeding cancellous bone.


This bleeding bed provides the necessary marrow-derived mesenchymal stem cells and growth factors to facilitate robust ligament-to-bone healing. Two suture anchors (typically 4.75 mm or smaller, biocomposite or PEEK) double-loaded with ultra-high-molecular-weight polyethylene (UHMWPE) sutures are then placed into the decorticated patellar margin. The anchors are spaced appropriately (one proximal, one distal) to recreate the broad native footprint.
The sutures are then passed through the mobilized MPFL stump. A secure, tissue-gripping stitch configuration is mandatory to prevent pull-through. A Krackow stitch or a locking Mason-Allen configuration is placed using the limbs from both anchors, effectively grasping the robust fibrous tissue of the MPFL and the overlying VMO fascia.


The critical moment of the procedure is tensioning. The knee is placed in 30 to 40 degrees of flexion, the point at which the patella should be fully engaged within the trochlear groove. The sutures are drawn tight, advancing the MPFL stump directly onto the decorticated bleeding bone bed. The surgeon must manually assess patellar tracking and lateral translation. The goal is to restore a firm endpoint with 1 to 2 quadrants of lateral glide. Overtensioning must be strictly avoided; the MPFL is a check-rein, not a medializing tether. Once the ideal tension is achieved, the knots are tied securely. The knee is then cycled through a full range of motion to ensure the repair is isometric, does not capture the patella in extension, and maintains stability in flexion.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, primary MPFL repair carries distinct risks and potential complications. The most devastating iatrogenic complication is over-constraint of the patellofemoral joint. If the MPFL is tied too tightly, or tensioned with the knee in full extension rather than 30 degrees of flexion, the patella will be forcefully tethered against the medial trochlea. This results in severe, intractable anterior knee pain, loss of terminal flexion, and rapid acceleration of medial compartment patellofemoral osteoarthritis. The incidence of clinically significant over-tensioning ranges from 2% to 5% in the literature. Avoidance relies entirely on intraoperative vigilance: tensioning at the correct flexion angle and verifying normal, uninhibited patellar glide prior to final knot tying.
Recurrent instability is the most common mode of failure, with incidence rates reported between 5% and 15% following primary repair. This typically occurs for two reasons: either the native tissue was too attenuated or poor in quality to hold the repair, or the surgeon failed to recognize and address underlying bony malalignment (e.g., severe trochlear dysplasia or an excessive TT-TG distance). When the repaired tissue is subjected to abnormal lateralizing vectors, it will inevitably stretch out or fail at the anchor interface.
Hardware-related complications, including anchor pull-out or patellar fracture, are rare but disastrous. Placing anchors too deep or violating the anterior patellar cortex creates a stress riser.
Neurologic complications, specifically saphenous neuralgia or numbness in the distribution of the infrapatellar branch, occur in up to 10% of cases due to the superficial nature of these nerves during the surgical approach.
Complications and Salvage Management Strategies
| Complication | Estimated Incidence | Avoidance Strategy | Salvage/Management |
|---|---|---|---|
| Recurrent Instability | 5% - 15% | Strict patient selection; address bony malalignment (TTO) if present. | Revision to MPFL Reconstruction (autograft/allograft); concurrent TTO if indicated. |
| Over-constraint / Stiffness | 2% - 5% | Tension at 30-40° flexion; ensure 1-2 quadrants of lateral glide remain. | Arthroscopic or open MPFL release/lengthening; aggressive physical therapy. |
| Patellar Fracture | < 1% | Use small diameter anchors (< 4.75mm); avoid penetrating anterior cortex. | ORIF of patella; revision of MPFL fixation to soft-tissue or alternative bony sites. |
| Saphenous Neuralgia | 5% - 1 |
