Mastering Medial Unicondylar Knee Arthroplasty: An Intraoperative Masterclass

Key Takeaway
Master the nuanced surgical technique of medial unicondylar knee arthroplasty (UKA) with this immersive guide. We cover detailed anatomy, rigorous patient selection, meticulous intraoperative execution, and essential pearls for optimal outcomes. Learn precise bone resections, gap balancing, and component implantation, preparing you for successful UKA procedures and managing potential complications.
Welcome, esteemed colleagues, fellows, and residents, to the operating theater. Today, we are undertaking a comprehensive exploration of medial unicondylar knee arthroplasty (UKA). This procedure is not merely a partial knee replacement; it is a profound testament to surgical precision, kinematic restoration, and meticulous technique. When executed flawlessly in an appropriately selected patient, UKA offers exceptional outcomes, rapid rehabilitation, and a knee that feels remarkably "native" compared to total knee arthroplasty (TKA).
Comprehensive Introduction and Patho-Epidemiology
The knee joint is classically divided into three distinct biomechanical compartments: the medial tibiofemoral, the lateral tibiofemoral, and the patellofemoral articulations. Unicondylar knee arthroplasty is specifically indicated for unicompartmental osteoarthritis (OA), a condition most commonly afflicting the medial compartment due to the natural mechanical axis of the lower extremity. The patho-epidemiology of medial unicompartmental OA is unique; it typically presents as anteromedial osteoarthritis (AMOA), a distinct clinical entity separated from generalized, tricompartmental degenerative joint disease. Understanding this distinction is the bedrock of successful UKA.
Historically, the success and widespread adoption of UKA were hampered by a confluence of less-than-ideal patient selection criteria, highly variable and evolving surgical techniques, and early component designs that failed to replicate native kinematics. Early pioneers faced unacceptably high revision rates, leading to a period of skepticism within the orthopedic community. However, the fundamental key to achieving a consistently successful, reproducible outcome in modern UKA lies in the harmonious marriage of three critical variables: rigorous and unyielding patient selection, meticulous surgical technique, and appropriate, anatomically driven component design.
Consider the biomechanics of the arthritic knee for a moment: to expose the subchondral bone surfaces on both the tibia and femur for optimal implant seating, we typically lose approximately 5 mm of articular cartilage and subchondral bone. This inherent material loss can predictably lead to about 5 degrees of varus deformity if not meticulously accounted for and corrected during the procedure. Our ultimate intraoperative goal is to restore the native alignment and kinematics without resorting to over-resection or inducing iatrogenic ligamentous imbalance.
The modern philosophy of UKA dictates that we are performing a resurfacing procedure, not a realignment procedure. Unlike a TKA, where we routinely release soft tissues to balance the knee to a mechanical neutral axis, in UKA, we rely entirely on the native, intact ligamentous envelope. We must respect the native joint line, restore the pre-diseased tension of the medial collateral ligament (MCL), and ensure the anterior cruciate ligament (ACL) can function optimally. Any deviation from this philosophy invariably leads to altered kinematics, accelerated polyethylene wear, and premature catastrophic failure of the construct.

Detailed Surgical Anatomy and Biomechanics
Compartmental and Osteological Anatomy
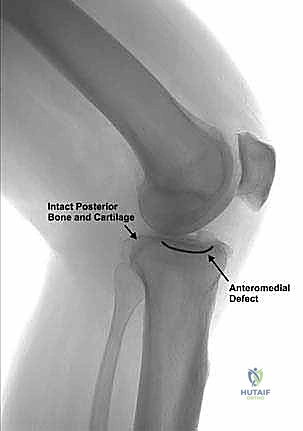
A profound, three-dimensional understanding of knee osteology is paramount for safe and effective bone resection. The medial tibial plateau typically exhibits a slight posterior slope, varying between 3 to 10 degrees in the native population, and can exhibit significant anterior and central erosion in AMOA. We must appreciate the extent of this erosion for accurate resection; the intact posterior cartilage on the medial plateau is a critical, non-negotiable indicator of ACL integrity. If the posterior plateau is eburnated, the ACL is functionally incompetent, and the patient requires a TKA.
The medial femoral condyle features a distinct trochlear groove anteriorly and a broad flexion surface posteriorly. The pattern of wear in appropriately selected UKA patients typically involves the anteromedial and distal weight-bearing surfaces, with complete preservation of the posterior flexion surface. This "extension disease" pattern is the hallmark of AMOA. Furthermore, intercondylar osteophytes frequently form on the lateral aspect of the medial femoral condyle; these must be meticulously resected, as they can impinge on the ACL, causing pseudo-laxity or accelerating ligamentous degeneration.
The patellofemoral joint, while not directly resurfaced in a medial UKA, plays a crucial role in overall knee biomechanics and patient satisfaction. Its health is a crucial selection criterion. While mild, asymptomatic patellofemoral chondromalacia is not an absolute contraindication, severe eburnation, lateral facet subluxation, or deep grooving will lead to persistent anterior knee pain postoperatively. The surgeon must evaluate the tracking of the patella dynamically during the initial exposure to ensure that restoring the medial joint space will not adversely alter patellofemoral kinematics.

Ligamentous Kinematics and Cruciate Degeneration
The intricate interplay of the knee's ligamentous structures dictates both stability and coupled motion. In a normal knee, most ligaments are at their resting, unstretched lengths in full extension, providing inherent stability during the stance phase of gait. As we flex the knee to approximately 20 to 30 degrees, the posterior capsule and the lateral collateral ligament (LCL) begin to slacken. This allows for a slight physiological gapping under tension, which is completely normal and expected during clinical examination.
Further gapping, particularly in the medial compartment, is strongly resisted by the ACL, the posterior cruciate ligament (PCL), and the deep and superficial bundles of the MCL. These ligaments are crucial for maintaining stability throughout the entire arc of motion. At 90 degrees of flexion, the lateral compartment typically distracts by approximately 7 mm under stress, while the medial compartment maintains a relatively constant 2-mm gap. This differential gapping highlights the importance of preserving the healthy lateral compartment and dictates our balancing strategy during UKA.
The cruciate ligaments and the MCL exert an isometric effect on the medial compartment throughout the entire range of motion, ensuring consistent tension and stability. This isometric behavior is precisely why we strive to avoid any release of the MCL in UKA. The ACL, in particular, can undergo a progressive cascade of degenerative failure: starting from a healthy, intact synovial covering, progressing to loss of synovium, longitudinal intra-substance splits, stretching, and eventually complete rupture and resorption. Degenerative failure of the ACL is the inciting event that transitions AMOA to posteromedial OA, leading to posterior subluxation of the tibia and structural shortening of the MCL. An intact, functional ACL is an absolute prerequisite for a successful UKA.

Neurovascular Considerations and Muscular Intervals
During our medial parapatellar approach and subsequent bony resections, the surgical team must be acutely aware of vital neurovascular structures. The saphenous nerve, a purely sensory branch of the femoral nerve, descends through the adductor canal and emerges medially, often crossing the surgical field just distal to the joint line. It is highly susceptible to injury during the initial skin incision and capsular exposure. Meticulous blunt dissection and careful retraction are crucial to avoid neuropraxia or transection, which can lead to persistent, debilitating medial knee pain or numbness.
Similarly, the infrapatellar branch of the saphenous nerve typically pierces the sartorius fascia and courses anteriorly, often within the subcutaneous tissue directly in the path of our standard incision. While some degree of lateral skin numbness is common and generally well-tolerated, direct sharp injury can lead to a painful neuroma. We must also respect the genicular arterial anastomoses. The superior and inferior medial genicular arteries are particularly relevant to our medial approach; while smaller in caliber, they can cause significant postoperative hematoma if not cauterized meticulously during the exposure.
Posteriorly, the popliteal artery and vein represent the most catastrophic risk during UKA. Positioned directly posterior to the capsule, these major vessels are somewhat protected by the posterior capsule and PCL. However, excessive posterior penetration with a reciprocating saw blade or osteotome during the horizontal tibial resection is a devastating error. Always ensure your saw blade does not violate the posterior tibial cortex excessively. The surgeon must keep a finger or a protective retractor on the posterior capsule to provide tactile feedback during this critical bone cut.

Exhaustive Indications and Contraindications
Clinical Presentation and Patient Selection
The classic presentation of a patient ideally suited for a medial UKA involves pain that is highly localized to the medial joint line. This pain is typically exacerbated by weight-bearing activities, prolonged standing, and walking, but is notably absent or minimal when sitting or resting. The patient will often point directly to the medial compartment with a single finger—the "one-finger sign." If the patient describes diffuse, poorly localized pain, or severe pain at rest, the surgeon must be highly suspicious of alternative pathologies, such as inflammatory arthropathy, complex regional pain syndrome, or referred pain from the lumbar spine or hip.
Physical examination is equally critical. In a single-leg stance, the load across the medial compartment is approximately 70%. This significantly increases to 90% when there is a varus deformity of 4 to 6 degrees, explaining the progressive, unrelenting nature of medial compartment wear. The surgeon must assess for a flexion contracture; while a contracture of less than 15 degrees is generally correctable through osteophyte removal and joint resurfacing, a contracture exceeding 15 degrees suggests severe capsular contracture and potential ACL compromise, pushing the patient toward a TKA.
Crucially, the varus deformity observed in standing must be manually correctable. This correctability often occurs spontaneously with 90 degrees of flexion and upon valgus stress at 20 degrees of flexion. Why does this happen? With chronic varus deformity, the posterior capsule and MCL shorten. However, when the capsule is relaxed at 20 degrees of flexion, the knee can be manually corrected to its pre-diseased alignment. At 90 degrees of flexion, the knee corrects spontaneously as the preserved cartilage on the flexion surface of the femur comes into contact with the posterior tibia, tensioning the MCL to its normal length. If the varus is fixed and rigid, UKA is contraindicated.

Radiographic Diagnostic Criteria
Plain radiographs remain the gold standard and are absolutely critical in determining whether the patient is an appropriate candidate for UKA. The weight-bearing anteroposterior (AP) radiograph is essential to assess joint space narrowing, subchondral sclerosis, cystic changes, and marginal osteophytes in the medial compartment. We are looking for true "bone-on-bone" eburnation. If there is only partial joint space narrowing, a UKA may over-stuff the joint, leading to persistent pain and early failure.

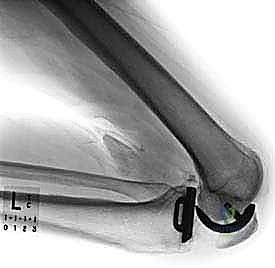
The lateral radiograph is arguably the most informative view for predicting ACL integrity. This view reveals the extent of posterior tibial wear. Preservation of posterior cartilage on the medial plateau suggests an intact, functioning ACL that is keeping the tibia reduced under the femur. If the wear extends to the posterior margin, the ACL is incompetent. Furthermore, the lateral view allows for assessment of patella alta/baja and the presence of significant patellofemoral osteophytes.
If only medial compartment arthritis is appreciated on the AP view, a valgus stress view is absolutely necessary. This dynamic radiograph demonstrates the normal thickness of the cartilage in the lateral compartment and, critically, shows whether the varus deformity is correctable. It confirms if the lateral compartment is healthy and if the MCL is functionally intact. A proper valgus stress view radiograph demonstrates realignment of the mechanical axis and preservation of the lateral joint space.
Indications vs. Contraindications Matrix
To synthesize these complex decision-making parameters, we rely on strict adherence to established criteria. The following table delineates the absolute indications and contraindications for medial UKA.
| Clinical Parameter | Indications for Medial UKA | Absolute Contraindications for Medial UKA |
|---|---|---|
| Pain Localization | Unicompartmental medial pain | Diffuse, generalized, or lateral pain |
| Ligamentous Status | Intact, functional ACL and MCL | ACL deficiency, MCL laxity/rupture |
| Deformity | Correctable varus (<15°), Flexion contracture <15° | Fixed varus, Valgus deformity, Flexion contracture >15° |
| Radiographic Wear | Bone-on-bone AMOA, preserved lateral/posterior cartilage | Tricompartmental OA, posterior medial wear |
| Inflammatory Status | Osteoarthritis, Osteonecrosis (SONK) | Rheumatoid arthritis, active infection, crystalline arthropathy |
| Patient Factors | Motivated, understands risk of revision | Morbid obesity (relative), non-compliant |

Pre-Operative Planning, Templating, and Patient Positioning
Digital Templating and Sizing
Meticulous preoperative digital templating is not an optional adjunct; it is a mandatory step in the UKA workflow. Templating allows the surgeon to anticipate component sizing, estimate the depth of bone resection required to restore the joint line, and predict the necessary posterior slope of the tibial cut. On the AP radiograph, the tibial component is sized to maximize cortical coverage without medial or posterior overhang. Overhang of even 1-2 mm can cause severe soft tissue irritation, particularly of the MCL and pes anserinus tendons, leading to intractable postoperative pain.
Femoral templating is performed primarily on the lateral radiograph. The goal is to match the native "J-curve" of the medial femoral condyle. The implant must sit flush with the anterior cartilage transition zone to avoid "catching" the patella during extension. Furthermore, the posterior condylar offset must be restored to ensure proper tensioning of the posterior capsule and optimal flexion kinematics. Undersizing the femur can lead to a loose flexion gap, while oversizing can restrict flexion and cause posterior impingement.
During templating, the surgeon must also evaluate the mechanical axis of the lower extremity using full-length standing alignment films. While we do not aim to correct the knee to a neutral 0-degree mechanical axis (which would over-tension the medial compartment and rapidly degrade the lateral compartment), we must understand the baseline deformity. The goal of UKA is to restore the patient's pre-morbid slight varus alignment, typically leaving them in 2 to 4 degrees of residual varus.
Operating Room Setup and Patient Positioning
The operating room setup for a UKA must be optimized for efficiency and ergonomics. The procedure is typically performed under regional anesthesia (spinal block) combined with a robust peripheral nerve block (such as an adductor canal block) to facilitate rapid postoperative mobilization and minimize opioid consumption. A tourniquet is generally applied to the proximal thigh but may be inflated only during cementation based on surgeon preference and the patient's vascular status.
Patient positioning is critical for achieving the necessary exposure without applying undue stress to the collateral ligaments. The patient is placed supine with a lateral thigh post or placed in a specialized leg holder that allows for unhindered flexion past 120 degrees. The ability to hyperflex the knee is absolutely essential for accessing the posterior aspect of the medial femoral condyle and ensuring adequate clearance for the posterior femoral bone cuts.
The sterile field must be meticulously prepared, draping the limb free to allow for dynamic manipulation throughout the procedure. The primary surgeon typically stands on the operative side, with the first assistant directly opposite. The surgical scrub technician should be positioned to anticipate the rapid sequence of instrumentation, as UKA procedures, once the exposure is complete, progress swiftly through a highly standardized sequence of bone preparation and trialing.

Step-by-Step Surgical Approach and Fixation Technique
Surgical Exposure and Joint Inspection
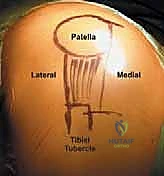
The procedure begins with a meticulously planned medial parapatellar incision. The skin incision extends from the superior pole of the patella to approximately 2-3 cm distal to the joint line, staying slightly medial to the tibial tubercle. We utilize a mini-midvastus or a standard medial parapatellar arthrotomy, taking great care to preserve the vastus medialis obliquus (VMO) insertion. The goal is to access the joint with minimal disruption to the extensor mechanism, which directly correlates with accelerated early rehabilitation.
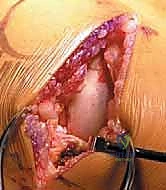
Upon entering the joint, a thorough, systematic intraoperative inspection is mandatory. This is the final checkpoint before committing to a unicompartmental replacement. The surgeon must directly visualize and probe the ACL to confirm its structural integrity and tension. The lateral compartment is inspected; the cartilage should be pristine, and the lateral meniscus intact. The patellofemoral joint is evaluated for severe eburnation. If the ACL is ruptured, or if there is full-thickness cartilage loss in the lateral compartment, the surgeon must immediately abort the UKA and transition to a TKA.
Once suitability is confirmed, the anterior horn of the medial meniscus is excised, and a portion of the retropatellar fat pad may be resected to improve visualization. Crucially, all medial, intercondylar, and patellar osteophytes must be aggressively resected using a rongeur or osteotome. Osteophytes tent the joint capsule and the MCL, creating artificial tightness. Removing them often corrects the varus deformity and restores the true, physiologic tension of the medial compartment. Never release the MCL to balance a UKA; if the joint remains too tight after osteophyte removal, you must resect more bone.


Tibial and Femoral Resections
Bone preparation begins with the tibia. An extramedullary tibial alignment guide is secured to the ankle and proximal tibia. The guide is adjusted to achieve a neutral varus/valgus cut (0 degrees to the mechanical axis of the tibia) and to match the patient's native posterior slope (typically 3 to 7 degrees). The depth of resection is conservative; we aim to resect 2-3 mm of bone from the deepest part of the defect, just enough to create a flat, bleeding cancellous surface for cement interdigitation.
The vertical sagittal cut is made first, positioned just medial to the apex of the medial tibial spine, taking extreme care not to violate the ACL footprint. This cut is made with a reciprocating saw. The horizontal cut is then executed with an oscillating saw, ensuring the blade does not plunge past the posterior cortex to protect the popliteal neurovascular bundle. The resected tibial plateau is removed, and the gap is measured.
Attention then turns to the femur. Depending on the specific implant system, an intramedullary or extramedullary guide is used to establish femoral alignment. Drill holes are placed in the distal femur to set the rotation and position of the cutting block. The distal femoral resection is performed, followed by the posterior chamfer cuts. The goal is to remove an amount of bone equal to the thickness of the femoral implant, thereby perfectly restoring the native joint line and preserving the kinematics of the knee.

Trialing, Balancing, and Final Implantation
With the bone cuts complete, trial components are inserted. This is the most critical phase of the operation: balancing the flexion and extension gaps. In a properly executed UKA, the extension gap and the flexion gap should be equal, and the knee should feel stable but not overly tight. We assess this by inserting spacer blocks or trial polyethylene inserts. The knee is taken through a full range of motion.
A fundamental principle of UKA trialing is the concept of "under-stuffing." The medial compartment should have approximately 1-2 mm of laxity in both flexion and extension. If the joint is stuffed too tightly with a thick polyethylene insert, the knee will be pushed into valgus, shifting the mechanical axis laterally and rapidly destroying the preserved lateral compartment. The surgeon must be able to slightly open the medial joint line with a valgus stress when the trials are in place. If it is completely unyielding, the insert is too thick, or insufficient bone has been resected.
Once the optimal sizes are confirmed, the bone surfaces are thoroughly pulsatile-lavaged and dried. Meticulous cementation technique is employed. High-viscosity bone cement is applied to both the implants and the bone surfaces. The components are impacted into place, and the knee is held in 45 degrees of flexion while the cement polymerizes. Great care must be taken to remove all extruded cement, particularly from the posterior aspect of the joint and around the ACL, as retained cement can cause severe third-body wear and impingement. The wound is closed in standard anatomical layers.


Complications, Incidence Rates, and Salvage Management
Intraoperative and Early Postoperative Complications
While UKA is a highly successful procedure, it is technically demanding, and complications, though relatively rare, can be unforgiving. Intraoperative tibial plateau fractures are a devastating complication, usually occurring during the impaction of the tibial component or if the vertical sagittal cut intersects the horizontal cut too deeply, creating a stress riser. Prevention relies on meticulous saw control and using a hand osteotome to finish the corner of the tibial cut. If a non-displaced fracture occurs, it may be managed with screw fixation; displaced fractures often necessitate immediate conversion to a stemmed TKA.
Neurovascular injuries, as discussed in the anatomy section, are rare but catastrophic. Popliteal artery injury requires immediate vascular surgery consultation and repair. More commonly, patients may experience neuropraxia of the saphenous nerve or its infrapatellar branch, leading to medial or anterior numbness. This is usually self-limiting but requires patient reassurance. Infection rates in UKA are generally lower than in TKA (typically <1%), but when deep infection occurs, it necessitates aggressive debridement, implant removal, and placement of an antibiotic spacer, followed by a two-stage revision to a TKA.
Deep vein thrombosis (DVT) and pulmonary embolism (PE) remain significant risks, although early mobilization protocols have drastically reduced their incidence. Postoperative hematoma can occur, particularly if the genicular arteries were not adequately cauterized. A tense hematoma can compromise wound healing and increase the risk of infection, occasionally requiring surgical evacuation.


Late Complications and Failure Modes
The most common cause for late revision of a UKA is aseptic loosening, most frequently affecting the tibial component. This is often heralded by progressive medial-sided pain and radiographic evidence of subsidence or radiolucent lines exceeding 2 mm. Aseptic loosening is frequently technical in origin, stemming
Clinical & Radiographic Imaging Archive