Masterclass: Cemented Total Knee Arthroplasty – Precision and Principles

Key Takeaway
This masterclass details Cemented Total Knee Arthroplasty, covering essential anatomy, meticulous preoperative planning, and granular intraoperative execution. Fellows will learn precise surgical techniques, critical pearls, and how to manage potential pitfalls for optimal patient outcomes and functional restoration.
Comprehensive Introduction and Patho-Epidemiology
Welcome, colleagues and fellows, to the operating theater and this advanced masterclass. Today, we are undertaking an exhaustive review of Cemented Total Knee Arthroplasty (TKA), an unequivocally successful surgical procedure renowned for providing excellent, durable relief of pain and profound improvement in functional status for patients suffering from end-stage osteoarthritic knees. This procedure remains a foundational pillar of reconstructive orthopaedics, offering patients a definitive restoration of mobility. As the global population ages and the prevalence of obesity rises, the demand for primary TKA is projected to grow exponentially, making mastery of its principles non-negotiable for the practicing arthroplasty surgeon.
Osteoarthritis (OA) of the knee, frequently termed degenerative joint disease (DJD), is fundamentally a consequence of the progressive mechanical and biological degradation of articular cartilage. This pathology is predominantly observed in the aging demographic, though it increasingly presents in younger cohorts due to post-traumatic sequelae or metabolic syndromes. The natural history of knee OA is typically characterized by a relentless, albeit variable, progressive deterioration. At a cellular level, the balance between chondrocyte-mediated matrix synthesis and degradation is disrupted, leading to an overexpression of matrix metalloproteinases (MMPs) and inflammatory cytokines such as Interleukin-1 (IL-1) and Tumor Necrosis Factor-alpha (TNF-α). This biochemical cascade results in the depletion of proteoglycans, disruption of the collagen network, and eventual catastrophic failure of the articular surface.
We meticulously classify knee OA into two primary etiological categories to guide our preoperative planning and manage patient expectations. Primary OA refers to idiopathic articular degeneration without a single, identifiable underlying cause. It is a complex, multifactorial disease process involving genetic predispositions, chronic aberrant biomechanical stresses, and intrinsic cellular senescence. Conversely, Secondary OA arises as a direct, identifiable consequence of either an abnormal concentration of force across the joint or from intrinsically compromised articular cartilage. Classic examples include post-traumatic arthritis following intra-articular fractures (such as tibial plateau or femoral condyle fractures), osteonecrosis, or inflammatory arthropathies like rheumatoid arthritis.

While systemic disease-modifying antirheumatic drugs (DMARDs) and biologic agents have revolutionized the medical management of rheumatoid arthritis, effectively halting its joint-destructive progression, there currently exist no proven, universally accepted disease-modifying osteoarthritis drugs (DMOADs) for primary knee OA. Consequently, when the mechanical integrity of the joint is lost and the subchondral bone is exposed, surgical intervention via arthroplasty becomes the only definitive treatment modality capable of restoring function and eliminating nociceptive pain.
Detailed Surgical Anatomy and Biomechanics
Osteology and Axes of Alignment
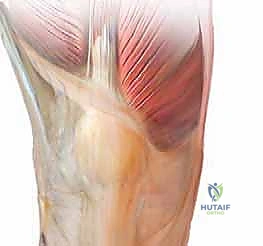
Before initiating any surgical approach, an intimate, three-dimensional understanding of the knee's intricate anatomy and its biomechanical axes is paramount. The knee is not a simple hinge; it is a complex, polycentric synovial joint that accommodates flexion, extension, and a crucial degree of coupled axial rotation. Its dynamic stability relies on a delicate, synergistic interplay between the bony congruity of the tibiofemoral and patellofemoral articulations and the robust static constraints of the collateral and cruciate ligaments.

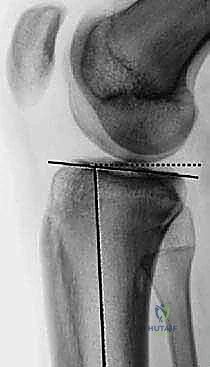
The precise restoration of the lower extremity's alignment is the most critical determinant of proper biomechanics, optimal load distribution, and long-term implant survivorship in cemented TKA. We define the mechanical axis of the lower limb as a theoretical line drawn from the center of the femoral head, passing through the center of the knee joint, and terminating at the center of the tibiotalar joint. Ideally, this forms a straight, collinear axis (0 degrees), representing the primary load-bearing vector during a single-leg stance. In stark contrast, the anatomic axis is defined by the intersection of the diaphyseal long axes of the femur and the tibia.
In a physiologically normal knee, the intersection of these two anatomic axes creates an inherent valgus angle of approximately 5 to 7 degrees. This physiological valgus is dictated by the specific bony morphology of the distal femur and proximal tibia. The proximal articular surface of the tibia typically presents in a slight constitutional varus of about 3 degrees. To compensate for this tibial varus and the lateral offset of the hip's center of rotation, the distal femur is oriented in approximately 9 degrees of valgus relative to its anatomic axis. Furthermore, in the sagittal plane, the native tibial articular surface is not orthogonal to the shaft; it exhibits a posterior slope ranging from 5 to 7 degrees, which is critical for facilitating femoral rollback and maximizing deep flexion.
Ligamentous Structures and Kinematics
The ligamentous envelope of the knee dictates its kinematic envelope. The medial collateral ligament (MCL) is the primary restraint to valgus stress. It consists of a superficial portion, which inserts distally on the medial tibial metaphysis, and a deep portion (meniscofemoral and meniscotibial ligaments). The lateral collateral ligament (LCL), a cord-like structure inserting on the fibular head, provides primary restraint against varus stress. During a TKA, achieving a balanced rectangular gap in both flexion and extension relies entirely on the precise tensioning and, when necessary, the measured release of these collateral structures.

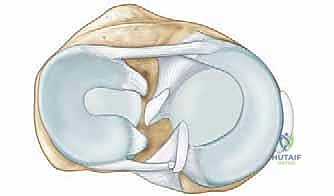
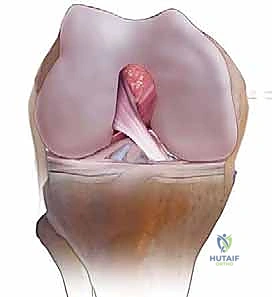
The cruciate ligaments govern the anteroposterior translation and complex roll-and-glide mechanics of the knee. The anterior cruciate ligament (ACL) prevents anterior tibial translation and is universally resected in standard TKA designs. The posterior cruciate ligament (PCL) prevents posterior tibial translation. The decision to retain or sacrifice the PCL dictates the choice of implant—Cruciate Retaining (CR) versus Posterior Stabilized (PS). PS designs utilize a tibial post and a femoral cam to mechanically substitute for the resected PCL, enforcing posterior femoral rollback during deep flexion to prevent posterior impingement.

Kinematically, the knee operates via a "screw-home" mechanism. As the knee approaches terminal extension, the tibia externally rotates relative to the femur (or the femur internally rotates on a fixed tibia), locking the joint into a highly stable, energy-efficient position for standing. This is driven by the asymmetry of the femoral condyles; the medial condyle is longer and extends further anteriorly than the lateral condyle. Restoring this complex kinematic relationship requires precise external rotation of the femoral component (typically 3 degrees relative to the posterior condylar axis) to optimize patellofemoral tracking and balance the flexion gap.
Neurovascular Considerations
Iatrogenic injury to the neurovascular structures surrounding the knee is a catastrophic complication that must be avoided through meticulous surgical technique. The infrapatellar branch of the saphenous nerve (IPBSN) consistently crosses the anterior aspect of the knee from medial to lateral. An anterior longitudinal midline incision almost invariably transects branches of this nerve, resulting in a predictable area of lateral cutaneous numbness distal to the incision. Patients must be explicitly counseled regarding this ubiquitous outcome during the preoperative consent process.

The vascular supply to the anterior knee and patella is a rich anastomotic ring, heavily reliant on the descending genicular artery medially and the superior/inferior genicular arteries. Extensive medial and lateral releases, combined with a standard medial parapatellar arthrotomy, can severely compromise patellar blood flow, potentially leading to avascular necrosis or patellar fracture. When utilizing a subvastus approach, proximal dissection must be strictly limited to avoid avulsing the descending genicular artery.
Posteriorly, the popliteal artery and vein lie intimately close to the posterior capsule, separated only by a thin layer of adipose tissue. Extreme vigilance is required during posterior capsular releases, resection of posterior osteophytes, or when passing saw blades through the posterior tibial cortex. Penetration of the posterior capsule can result in limb-threatening vascular injury. Laterally, the common peroneal nerve courses around the fibular neck. It is highly susceptible to traction injury during the correction of severe, fixed valgus deformities, potentially resulting in a devastating foot drop.
Exhaustive Indications and Contraindications
Clinical Evaluation and Differential Diagnosis
The decision to proceed with a cemented TKA is never predicated solely on radiographic findings; it is fundamentally a clinical decision based on the patient's symptomatology and functional deficit. The initial evaluation must meticulously parse out the exact etiology of the patient's pain. We must maintain a high index of suspicion for referred pain originating from ipsilateral hip osteoarthritis or lumbar spinal stenosis (radiculopathy), which can frequently masquerade as primary knee pathology. Diagnostic intra-articular injections of local anesthetic can serve as a highly effective tool to isolate the pain generator in ambiguous presentations.

A rigorous physical examination begins with observing the patient's gait, looking for antalgia, thrust (varus or valgus), and the use of ambulatory aids. In the standing position, we assess for global alignment deformities. The skin must be thoroughly inspected for previous surgical scars, which will dictate our incision placement to avoid ischemic skin necrosis between parallel incisions. Range of motion (ROM) is documented both actively and passively, noting any fixed flexion contractures or extensor lags, as these will significantly alter our intraoperative bone resection and soft tissue balancing strategies.
Ligamentous integrity is assessed via varus and valgus stress testing at both 0 and 30 degrees of flexion. Instability at 30 degrees suggests isolated collateral ligament laxity, while instability at full extension implies a more profound, multiligamentous deficiency involving the posterior capsule or cruciate ligaments. The patellofemoral joint is evaluated using the patellar apprehension test, patellar tilt test, and patellar grind test to identify concurrent patellofemoral arthritis or maltracking, which may necessitate patellar resurfacing or a lateral retinacular release.
Diagnostic Imaging Modalities
High-quality, standardized, weight-bearing radiographs are the cornerstone of preoperative planning. A standard knee series must include a weight-bearing anteroposterior (AP) view, a weight-bearing lateral view in extension, and a skyline (Merchant) view of the patella. The AP view reveals joint space narrowing, subchondral sclerosis, osteophyte formation, and the presence of subchondral cysts. The lateral view is essential for assessing patellar height (Insall-Salvati ratio) and the posterior slope of the tibia.

Crucially, we must obtain a 45-degree posteroanterior (PA) weight-bearing view (the Rosenberg view). Because cartilage wear in early-to-moderate OA predominantly affects the posterior aspect of the femoral condyles, the standard extension AP view may falsely appear normal. The flexed Rosenberg view unloads the patella and brings the worn posterior condyles into contact with the tibia, revealing hidden joint space narrowing. Furthermore, a full-length, hip-to-ankle standing radiograph is highly recommended, particularly in patients with severe deformities or a history of prior femoral/tibial fractures, to accurately determine the mechanical axis and identify any extra-articular deformities that might complicate intramedullary instrumentation.
Patient Selection Criteria
The primary indication for a TKA is debilitating, refractory pain that significantly impairs the patient's activities of daily living and quality of life, coupled with definitive radiographic evidence of advanced joint destruction. TKA is an elective, quality-of-life procedure; therefore, the patient must have exhausted all reasonable conservative modalities, including weight loss, physical therapy, NSAIDs, and intra-articular injections (corticosteroids or hyaluronic acid).

| Category | Specific Contraindications to Total Knee Arthroplasty |
|---|---|
| Absolute Contraindications | Active local or systemic infection (e.g., bacteremia). |
| Severe peripheral vascular disease (lack of palpable pulses without vascular clearance). | |
| Neuropathic (Charcot) joint (historically absolute, currently highly relative with specialized implants). | |
| Functionless extensor mechanism (e.g., chronic, irreparable patellar tendon rupture). | |
| Relative Contraindications | Severe, uncontrolled medical comorbidities (e.g., recent MI, unoptimized heart failure). |
| Morbid obesity (BMI > 40 kg/m², associated with exponentially higher rates of PJI and failure). | |
| Poor soft tissue coverage over the anterior knee. | |
| Severe osteoporosis (may necessitate long-stemmed implants or alternative fixation). | |
| Non-compliance or severe psychiatric disorders precluding postoperative rehabilitation. |
Pre-Operative Planning, Templating, and Patient Positioning
Digital Templating and Implant Selection
Meticulous preoperative templating is the blueprint for a successful TKA. Utilizing digital templating software on calibrated radiographs allows the surgeon to anticipate the required component sizes, determine the optimal level of bony resection, and identify potential anatomical anomalies. On the AP radiograph, the femoral component size is estimated by matching the mediolateral width of the implant to the distal femur, avoiding overhang which can cause soft tissue irritation. The tibial component is sized to maximize cortical coverage without impinging on the collateral ligaments.

On the lateral radiograph, templating is critical for preventing anterior femoral notching, a technical error that significantly increases the risk of postoperative periprosthetic supracondylar femur fractures. The size of the femoral component is chosen to restore the anteroposterior dimension of the native femur, ensuring the anterior flange sits flush with the anterior cortex while the posterior condyles restore the flexion gap. The expected thickness of the polyethylene insert is also estimated, aiming for a composite tibial construct that restores the native joint line elevation.
Operating Room Setup and Patient Positioning
Optimal patient positioning and operating room setup are vital for surgical efficiency and infection control. The patient is placed supine on the operating table. A pneumatic tourniquet is routinely placed on the proximal thigh. While the absolute necessity of a tourniquet is debated in the era of tranexamic acid (TXA), it remains widely used to ensure a bloodless field, particularly during the crucial cementing phase, as blood interposition severely compromises the polymethylmethacrylate (PMMA) bone-cement interface.

A lateral post or a specialized leg holder is utilized to maintain the knee in a stable, flexed position (typically 90 to 110 degrees) during the procedure. The contralateral leg must be carefully padded to prevent pressure-induced neuropathies, such as peroneal nerve palsy. Intravenous antibiotics (typically a first-generation cephalosporin like cefazolin, or vancomycin for MRSA-colonized patients) must be administered within one hour prior to the surgical incision to maximize tissue concentrations. Intravenous or topical TXA is now the standard of care to minimize perioperative blood loss and reduce transfusion requirements.

Step-by-Step Surgical Approach and Fixation Technique
Surgical Exposure and Soft Tissue Management
The most ubiquitous approach for TKA is the medial parapatellar arthrotomy. A straight, anterior longitudinal skin incision is made, extending from just proximal to the superior pole of the patella to just medial to the tibial tubercle. Full-thickness fasciocutaneous flaps are elevated to preserve the subdermal vascular plexus. The arthrotomy is then initiated through the medial retinaculum, coursing proximally into the quadriceps tendon (leaving a small medial cuff for later repair) and distally along the medial border of the patella and patellar tendon.

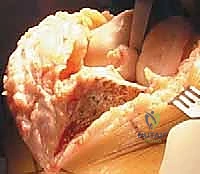
Once the joint is entered, the patella is either everted laterally or laterally subluxated, depending on the surgeon's preference and the stiffness of the extensor mechanism. A meticulous synovectomy and excision of the infrapatellar fat pad (Hoffa's fat pad) are performed to enhance visualization of the lateral compartment and the tibial plateau. All peripheral osteophytes on the femur and tibia must be aggressively resected at this stage. Retained osteophytes will artificially tension the collateral ligaments, leading to erroneous gap balancing and postoperative stiffness.

Bony Resection and Gap Balancing
The philosophy of TKA relies on creating equal and symmetrical flexion and extension gaps. This can be achieved via a "measured resection" technique (resecting bone equal to the thickness of the implant based on anatomical landmarks) or a "gap balancing" technique (tensioning the soft tissues first and making bone cuts parallel to the tensioned ligaments). Most modern surgeons utilize a hybrid approach.

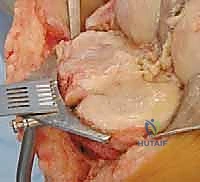
The distal femoral resection is typically performed first, utilizing an intramedullary alignment guide. The entry hole is made just anterior to the origin of the PCL. The valgus angle of the cutting block is set based on preoperative templating (usually 5 to 7 degrees) to restore a neutral mechanical axis. The distal cut removes approximately 9 mm of bone from the most prominent condyle, corresponding to the thickness of the femoral component.
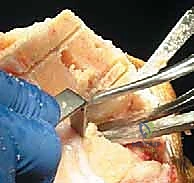
Next, the proximal tibial resection is executed, almost exclusively using an extramedullary alignment guide. The guide is aligned with the medial third of the tibial tubercle proximally and the center of the talus distally. The cutting block is set to resect 8 to 10 mm of bone from the unaffected compartment, incorporating a 3 to 5-degree posterior slope. This cut must be strictly orthogonal to the mechanical axis of the tibia in the coronal plane.

Femoral sizing and rotation are then determined. Proper femoral rotation is paramount for patellofemoral tracking and flexion gap symmetry. The rotation is typically set at 3 degrees of external rotation relative to the posterior condylar axis (PCA), or parallel to the surgical transepicondylar axis (TEA) and perpendicular to Whiteside's line (the AP axis of the trochlea). Once rotation is established, the anterior, posterior, and chamfer cuts are made using a 4-in-1 cutting block.

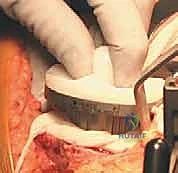
Cementing Technique and Implant Implantation
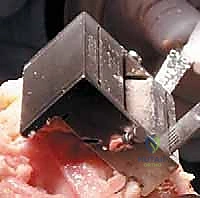
The hallmark of a cemented TKA is the creation of a durable, interlocking micro-mechanical bond between the host trabecular bone and the polymethylmethacrylate (PMMA) bone cement. PMMA is not an adhesive; it functions as a grout. Therefore, meticulous bone bed preparation is the single most critical factor in preventing aseptic loosening. The resected bony surfaces must be aggressively cleansed using pulsatile lavage to remove marrow, fat, and debris, exposing the porous cancellous bone. Sclerotic areas should be perforated with a small drill bit to enhance cement interdigitation.

The bone must be thoroughly dried immediately prior to cement application. High-viscosity cement is typically mixed under a vacuum to reduce porosity and increase fatigue strength. The cement is applied during its "doughy" phase to both the implant surfaces and the prepared bone. The components are then impacted into place.


Crucially, the cement must be pressurized into the cancellous bone to achieve a penetration depth of 3 to 4 mm. Once the components are seated, all extruded peripheral cement must be meticulously removed with a curette, particularly from the posterior aspect of the condyles and the posterolateral corner, where retained cement fragments can cause severe postoperative pain, third-body wear, or impingement. The knee is then held in full extension with axial compression applied until the exothermic polymerization process is complete and the cement is fully cured.


Complications, Incidence Rates, and Salvage Management
Intraoperative and Early Post-Operative Complications
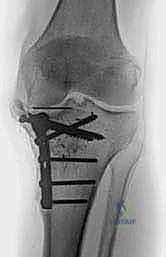
Despite advancements in surgical technique, TKA carries inherent risks that the surgeon must be prepared to manage. Intraoperative complications include periprosthetic fractures, most commonly involving the medial tibial plateau during aggressive exposure or the femoral condyles during component impaction. These require immediate recognition and appropriate rigid internal fixation (e.g., screws or stems) to allow for early mobilization. Extensor mechanism disruption, such as avulsion of the patellar tendon from the tibial tubercle, is a devastating complication requiring robust surgical repair (often utilizing synthetic mesh or allograft) and prolonged immobilization.

Early postoperative complications are dominated by venous thromboembolism (VTE), including deep vein thrombosis (DVT) and pulmonary embolism (PE). Routine pharmacological prophylaxis (e.g., low molecular weight heparin, direct oral anticoagulants, or aspirin) combined with mechanical prophylaxis (sequential compression devices) is mandatory. Acute periprosthetic joint infection (PJI) occurring within the first 4 weeks postoperatively requires emergent surgical intervention, typically an irrigation and debridement (I&D) with modular polyethylene exchange, coupled with targeted intravenous antibiotic therapy.

Late Complications and Revision Considerations
Long-term failure of a cemented TKA is most frequently attributed to aseptic loosening, chronic PJI, or polyethylene wear leading to osteolysis. Aseptic loosening presents radiographically as progressive, contiguous radiolucent lines greater than 2 mm at the bone-cement interface, often accompanied by component migration or subsidence. This necessitates a revision arthroplasty, utilizing longer diaphyseal engaging stems and potentially highly porous metaphyseal cones or sleeves to bypass the compromised bone and achieve stable fixation.

Chronic PJI is a devastating late complication. Diagnosis relies on a high index of suspicion, elevated serum inflammatory markers (ESR, CRP), and definitive synovial fluid analysis demonstrating elevated leukocyte counts, high neutrophil percentages, or positive cultures. The gold standard for managing chronic PJI in North America remains a two-stage revision protocol: explantation of all components and cement, aggressive debridement, placement of an antibiotic-impregnated PMMA spacer, a 6-week course of IV antibiotics, and subsequent reimplantation once the infection is eradicated.