Biomechanics of Total Knee Arthroplasty: A Clinical Guide
Key Takeaway
Understanding the biomechanics of total knee arthroplasty is paramount for achieving optimal implant survivorship and restoring native joint kinematics. This comprehensive guide details the triaxial motion of the knee, the critical debate between posterior cruciate ligament (PCL) retention and substitution, and precise surgical alignment techniques. By mastering gap balancing, femoral rollback mechanics, and evidence-based postoperative protocols, orthopedic surgeons can minimize polyethylene wear, prevent instability, and ensure superior functional outcomes in primary and complex knee reconstructions.
Comprehensive Introduction and Patho-Epidemiology
The ultimate goal of Total Knee Arthroplasty (TKA) transcends the mere eradication of nociceptive stimuli; it demands the precise restitution of native joint kinematics and dynamic stability. Achieving this standard requires the orthopedic surgeon to possess a profound, uncompromising understanding of the biomechanics of knee arthroplasty. Historically, the human knee was erroneously conceptualized as a simple unidirectional hinge joint. Early prosthetic iterations, such as the Walldius hinge, operated under this flawed paradigm, leading to catastrophic early aseptic loosening due to massive unmitigated torsional and shear stresses at the bone-cement interface. We now understand that the knee is an exquisitely complex, dynamic articulation governed by asymmetric articular geometry and a highly sophisticated network of viscoelastic ligamentous restraints.
The patho-epidemiology of knee osteoarthritis (OA) underscores the urgency of mastering these biomechanical principles. Knee OA is a progressive, non-inflammatory, degenerative joint disease characterized by the focal loss of articular cartilage, subchondral bone sclerosis, osteophyte formation, and variable degrees of synovial inflammation. As the global population ages and the prevalence of obesity reaches epidemic proportions, the incidence of end-stage knee OA has surged exponentially. Consequently, TKA has become one of the most frequently performed and highly successful surgical interventions in modern medicine, with projections indicating millions of procedures performed annually worldwide. However, this increased volume brings a concomitant rise in the absolute number of revision arthroplasties, driven largely by mechanical failures, instability, and polyethylene wear—all of which are fundamentally rooted in biomechanical mismatch.
Modern prosthetic designs and surgical philosophies attempt to reproduce normal knee kinematics as closely as possible, balancing the clinical need for a functional range of motion against the tribological demands of minimizing polyethylene contact stresses. The contemporary orthopedic surgeon must navigate a labyrinth of design rationales—from cruciate-retaining to posterior-stabilized, and from measured resection to gap balancing. The ultimate survivorship of the prosthesis is inextricably linked to how well the implanted components manage the transfer of loads during the gait cycle. A biomechanically optimized TKA distributes compressive forces evenly across the tibial plateau while accommodating the obligatory rotational moments that occur during flexion and extension.
This comprehensive clinical guide systematically deconstructs the kinematics of the native knee, the biomechanical rationale behind posterior cruciate ligament (PCL) retention versus substitution, the exacting principles of axial and rotational alignment, and the step-by-step surgical execution required to achieve a biomechanically flawless TKA. Furthermore, it addresses the tribological consequences of component malpositioning and outlines the evidence-based postoperative protocols necessary to maximize functional outcomes. The mastery of these concepts is the distinguishing hallmark of an expert reconstructive surgeon.
Detailed Surgical Anatomy and Biomechanics
Native Knee Kinematics and Triaxial Motion
Knee motion during the normal gait cycle has been extensively studied using advanced dynamic imaging and is recognized to be vastly more complex than simple sagittal plane flexion and extension. Motion occurs simultaneously in three separate planes, a phenomenon referred to as "triaxial motion," encompassing six degrees of freedom: flexion/extension, internal/external rotation, varus/valgus angulation, anterior/posterior translation, medial/lateral translation, and proximal/distal compression.
The primary arc of motion, flexion and extension, does not occur around a fixed transverse axis. Instead, it occurs around a constantly varying center of rotation that describes a J-shaped curve (the evolute) around the posterior femoral condyles. This shifting instantaneous center of rotation is dictated by the diminishing radius of curvature of the posterior femoral condyles compared to the distal condyles.
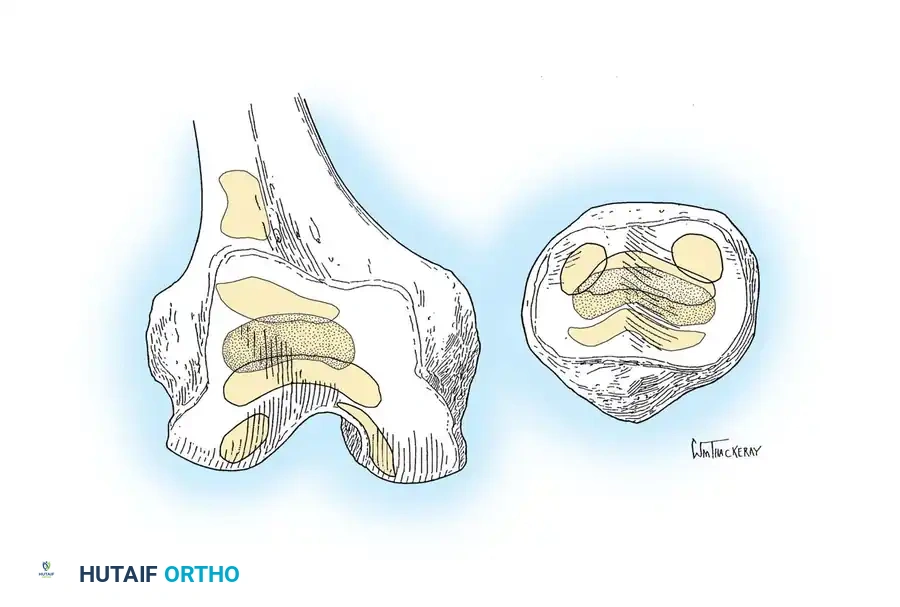
Dennis et al. revolutionized our understanding of in vivo knee kinematics by utilizing dynamic fluoroscopy coupled with three-dimensional CT scans. Their work definitively demonstrated that the flexion axis varies in a helical fashion. In the normal native knee, there is an asymmetric posterior translation (rollback) of the femoral condyles on the tibia during deep flexion. The medial femoral condyle is highly constrained by the robust medial meniscus and the anterior cruciate ligament, averaging only 1 to 2 mm of posterior translation. In stark contrast, the lateral femoral condyle is far more mobile, averaging up to 21 mm of posterior translation as it rolls backward on the convex lateral tibial plateau.
This medially based pivoting pattern explains the obligatory external rotation of the tibia on the femur during terminal extension—classically known as the "screw-home mechanism." As the knee approaches full extension, the lateral condyle halts its anterior excursion before the medial condyle, forcing the tibia to externally rotate to achieve the locked, energy-efficient position of terminal extension. Conversely, during the initiation of knee flexion, the popliteus muscle unlocks the knee by internally rotating the tibia. Modern TKA designs must account for this rotational freedom; failure to do so results in the transfer of massive torsional loads directly to the implant-bone interface, precipitating early aseptic loosening.
Prosthetic Design Paradigms: PCL-Retaining vs. PCL-Substituting
Since the concurrent development of PCL-retaining (Cruciate Retaining, CR) and PCL-substituting (Posterior Stabilized, PS) prostheses in the 1970s, the relative biomechanical merits of each have been fiercely debated within the orthopedic community. Both design philosophies boast excellent long-term survivorship exceeding 90% at 15 years, yet they achieve femoral rollback and sagittal stability through entirely disparate mechanical pathways.
The biomechanics of PCL retention (CR) rely entirely on the structural integrity and precise tensioning of the native PCL to achieve effective femoral rollback. To accommodate the necessary physiological glide and rotation, the tibial articular surface of a CR prosthesis is typically engineered to be flatter (less conforming) in the sagittal plane. Retaining the PCL theoretically preserves native proprioceptive mechanoreceptors and provides a more symmetrical gait, particularly during demanding activities such as stair climbing, as noted in the seminal kinematic studies by Andriacchi and Galante.
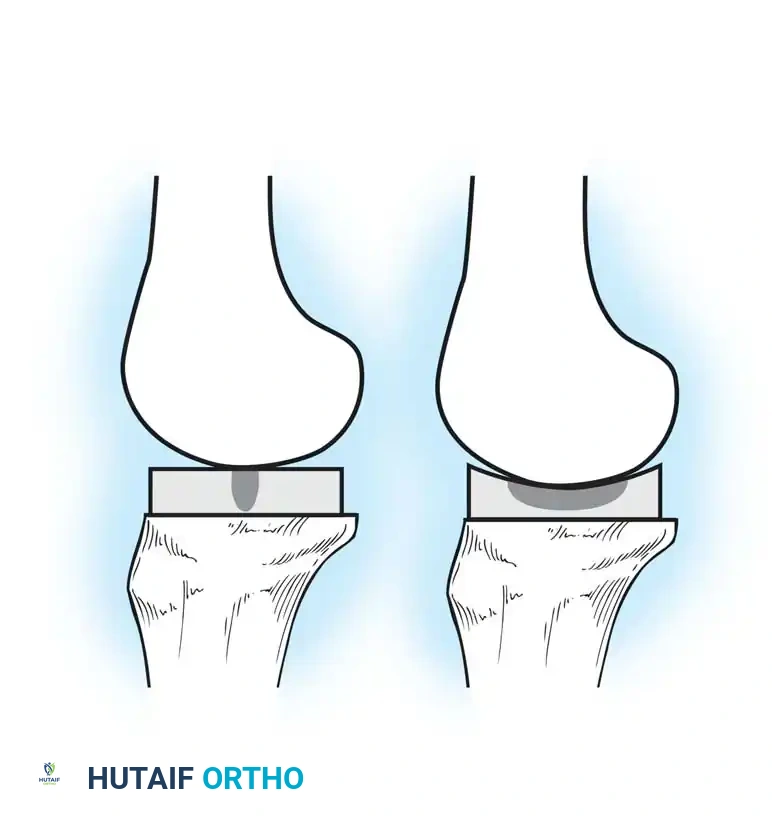
However, CR designs present formidable surgical challenges regarding soft tissue balancing. The PCL must be perfectly tensioned. A PCL that is excessively tight in flexion will cause exaggerated femoral rollback, driving the femoral condyles to override the posterior edge of the tibial polyethylene, leading to accelerated posterior wear and edge loading. Conversely, an incompetent or overly released PCL leads to paradoxical anterior tibial translation during flexion. This paradoxical motion severely limits the maximum range of motion by causing early posterior impingement and dramatically increases anterior polyethylene wear due to abnormal contact mechanics.
In PCL-substituting (PS) designs, the native PCL is deliberately resected. Posterior displacement (rollback) in flexion is mechanically forced by a central polyethylene tibial post contacting a transverse metallic femoral cam. This cam-post mechanism engages at approximately 60 to 70 degrees of flexion, ensuring uniform, reproducible femoral rollback and preventing paradoxical anterior translation regardless of the patient's native soft tissue envelope.
Originally, critics of the PS design argued that the added prosthetic constraint would inevitably transfer excessive shear stress to the prosthesis-bone interface, leading to premature aseptic loosening. However, decades of registry data have proven the loosening rates between CR and PS designs to be statistically indistinguishable. The primary biomechanical vulnerability of the PS design lies in the tibial post itself, which is subjected to massive shear forces and is a known site of wear, deformation, and potential catastrophic breakage. This risk is exponentially magnified if the femoral component is implanted in a flexed position, if the tibial slope is excessively increased, or if the knee is allowed to hyperextend, causing anterior impingement of the femoral intercondylar box against the post.
Patellofemoral Mechanics and Joint Line Elevation
The patellofemoral joint is a critical determinant of patient satisfaction following TKA, and its biomechanics are profoundly influenced by component positioning. The patella functions as a mechanical fulcrum, increasing the moment arm of the quadriceps muscle. This extensor lever arm is maximized when femoral rollback moves the tibiofemoral contact point posteriorly, effectively translating the tibial tubercle more anteriorly relative to the femur.
Patellofemoral tracking and stability are exquisitely sensitive to the restoration of the native joint line. Joint line elevation is a common technical error, particularly in revision scenarios or when attempting to correct severe flexion contractures by excessive distal femoral resection. CR designs are notoriously intolerant of significant joint line alteration; elevating the joint line in a CR knee alters the tension of the retained PCL, often necessitating its release.
While PS designs are slightly more forgiving of mild joint line elevation regarding sagittal stability, altering the joint line fundamentally changes the relationship of the patella to the prosthetic trochlear groove. In PS designs, the femoral component features an intercondylar box to accommodate the cam mechanism. If the joint line is elevated, the patella sits relatively lower (patella baja). During extension, hypertrophic superior pole synovium or a prominent quadriceps tendon nodule can become entrapped in this intercondylar box. As the knee actively extends, this tissue abruptly pops out of the box, resulting in "patellar clunk syndrome," a highly painful and functionally limiting complication unique to posterior-stabilized knees that often requires arthroscopic debridement.
Tribology and Polyethylene Wear Mechanisms
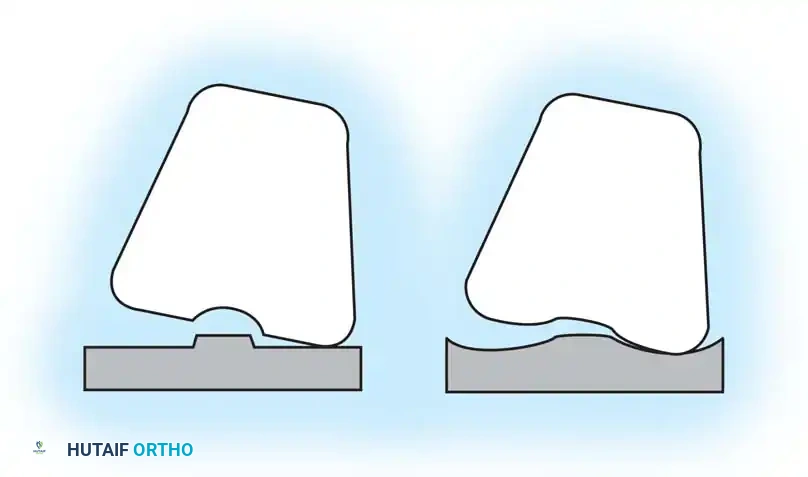
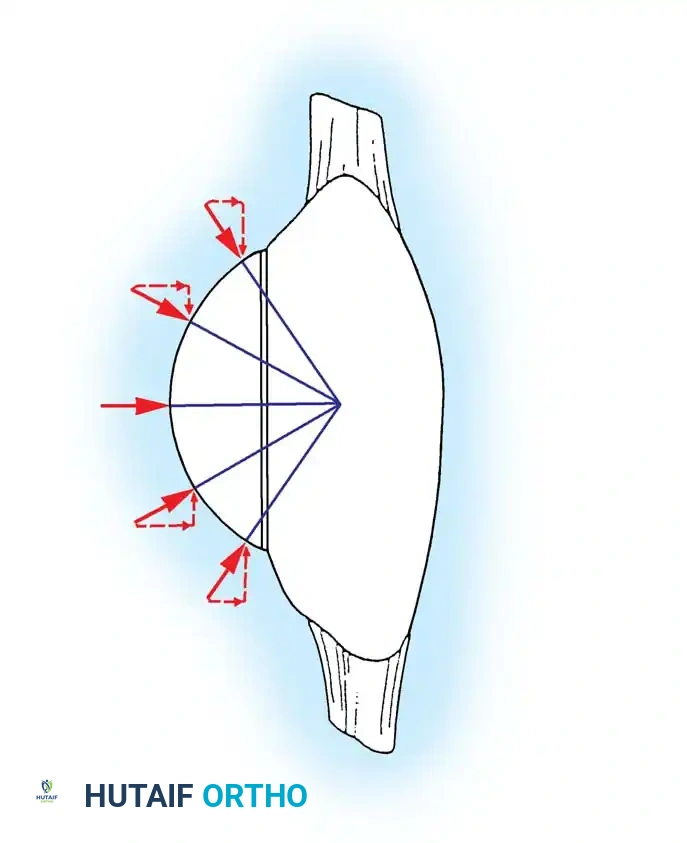
Polyethylene wear remains one of the primary limiting factors in the ultimate longevity of a total knee arthroplasty. The tribological performance of the bearing surface is dictated by a complex interplay of prosthesis design (conformity), material properties (e.g., highly cross-linked polyethylene, vitamin E doping), and the patient's in vivo kinematics. Unlike the hip joint, which is a highly conforming ball-and-socket, the knee is inherently non-conforming, leading to significantly higher and more complex contact stresses.

Because CR prostheses utilize a flatter, less conforming tibial articular surface to permit the necessary rotational freedom and femoral rollback dictated by the native PCL, the contact area between the metallic femoral condyles and the polyethylene tibia is substantially reduced. According to Hertzian contact mechanics, a decreased contact area under a given load results in exponentially higher contact stresses. These elevated subsurface shear stresses can exceed the yield strength of ultra-high-molecular-weight polyethylene (UHMWPE).

If a CR knee is poorly balanced—for instance, if the PCL is excessively tight—it acts as a rigid fulcrum during deep flexion, driving the femoral condyles violently into the posterior lip of the tibial insert. This phenomenon, known as edge-loading, dramatically amplifies local contact stress, leading to rapid subsurface delamination, gross pitting, and accelerated posterior wear of the polyethylene. The resulting generation of billions of submicron particulate debris particles triggers a macrophage-mediated inflammatory cascade, ultimately culminating in periprosthetic osteolysis and aseptic loosening.
Conversely, while PS designs generally offer higher tibiofemoral conformity and consequently lower articular contact stresses, they introduce an entirely new and highly stressed wear interface: the cam-post articulation. The anterior aspect of the post is vulnerable to impingement in hyperextension, while the posterior aspect is subjected to massive compressive and shear forces during deep flexion rollback. Aseptic loosening secondary to massive osteolysis generated specifically from post-generated polyethylene debris remains a well-recognized, design-specific failure mode in PS knees.
Exhaustive Indications and Contraindications
The decision to proceed with Total Knee Arthroplasty must be predicated on a rigorous evaluation of the patient's clinical symptoms, functional impairment, and radiographic findings. The primary indication for TKA is debilitating, refractory pain and functional disability secondary to end-stage destructive joint disease that has failed exhaustive conservative management (e.g., weight loss, activity modification, NSAIDs, physical therapy, intra-articular corticosteroid or hyaluronic acid injections).
Primary osteoarthritis is the most common etiology, characterized radiographically by asymmetric joint space narrowing, subchondral sclerosis, osteophytosis, and subchondral cysts. Other indications include inflammatory arthropathies (such as rheumatoid arthritis, where bilateral, symmetric joint space destruction is typical), post-traumatic osteoarthritis resulting from prior intra-articular fractures or chronic ligamentous instability, and severe crystalline arthropathies. It is paramount to emphasize that radiographic severity alone does not dictate the need for surgery; the patient's subjective experience of pain and objective loss of function are the true surgical triggers.
The orthopedic surgeon must also carefully evaluate the patient for contraindications to ensure that the risks of surgery do not outweigh the potential benefits. Absolute contraindications represent scenarios where TKA will almost certainly result in catastrophic failure or severe harm to the patient. Relative contraindications require a highly individualized risk-benefit analysis, often necessitating extensive preoperative optimization and multidisciplinary medical management.
| Category | Condition | Clinical Rationale and Biomechanical Impact |
|---|---|---|
| Absolute Contraindication | Active Local or Systemic Infection | Implanting foreign hardware into an infected bed guarantees periprosthetic joint infection (PJI), necessitating immediate explantation. |
| Absolute Contraindication | Incompetent Extensor Mechanism | A functioning quadriceps and patellar tendon are required for knee extension and stability. TKA in this setting results in uncontrollable giving-way. |
| Absolute Contraindication | Severe Peripheral Vascular Disease | Inadequate arterial inflow precludes wound healing, leading to massive soft tissue necrosis, deep infection, and high risk of major amputation. |
| Absolute Contraindication | Neuropathic (Charcot) Arthropathy | Loss of protective proprioception and nociception leads to rapid, catastrophic mechanical failure, massive bone loss, and implant fracture. |
| Relative Contraindication | Morbid Obesity (BMI > 40) | Exponentially increases the risk of wound complications, PJI, and early mechanical loosening due to excessive compressive forces on the implant. |
| Relative Contraindication | Poorly Controlled Diabetes (HbA1c > 7.5%) | Impairs microvascular perfusion and neutrophil function, drastically increasing the risk of surgical site infection and delayed wound healing. |
| Relative Contraindication | Severe Osteoporosis | Compromises the mechanical interdigitation of PMMA cement and increases the risk of intraoperative and postoperative periprosthetic fractures. |
| Relative Contraindication | History of Prior Knee Infection | Even if presumed eradicated, dormant sessile bacteria in biofilms can reactivate. Requires exhaustive pre-op aspiration and serological workup. |
Pre-Operative Planning, Templating, and Patient Positioning
Radiographic Assessment and Templating
Meticulous preoperative planning is the foundation of a biomechanically successful TKA. The standard radiographic series must include a standing anteroposterior (AP) view, a weight-bearing posteroanterior flexion view (Rosenberg view) to assess the posterior condylar cartilage wear, a true non-weight-bearing lateral view, and a tangential patellofemoral (Merchant or Sunrise) view. For patients with significant angular deformities, full-length standing long-leg radiographs are mandatory to accurately calculate the mechanical axis and assess for extra-articular deformities.
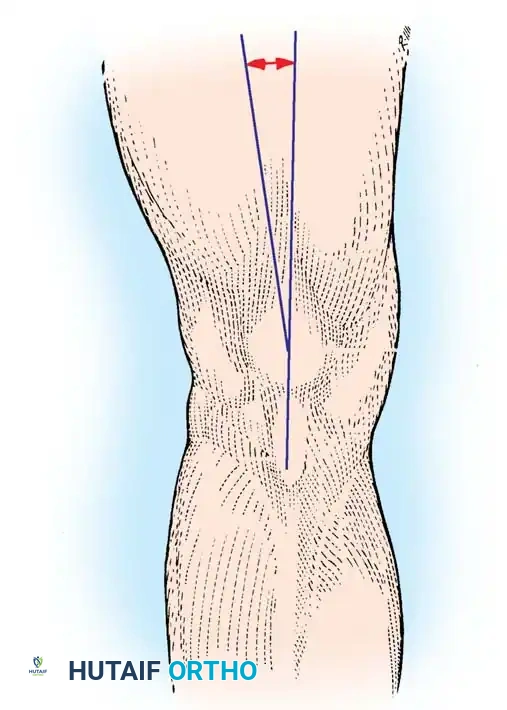
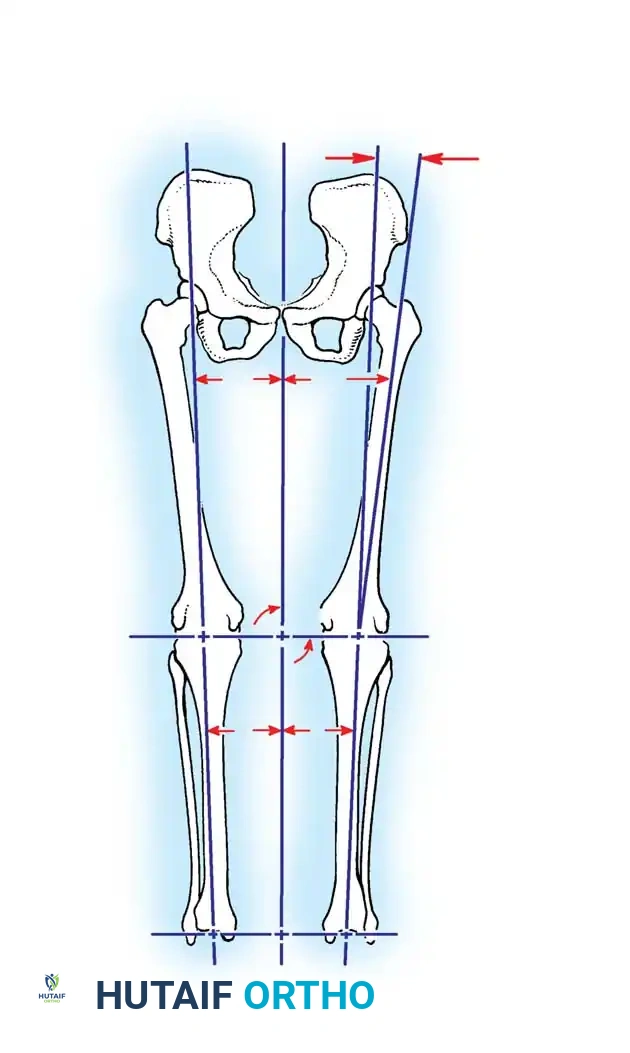
The mechanical axis of the lower extremity is defined as a line drawn from the center of the femoral head to the center of the talar dome. In a neutrally aligned, biomechanically optimized TKA, this axis should pass directly through the center of the knee joint. In contrast, the anatomical axes of the femur and tibia normally form a valgus angle of approximately 6 ± 2 degrees. The distal femoral cut is typically made at an angle relative to the anatomical axis (usually 5 to 7 degrees of valgus) to ensure the final femoral component is perpendicular to the mechanical axis.
Digital templating software is now universally employed to estimate component sizing, predict the level of bone resection, and plan the restoration of the joint line and femoral offset. On the lateral radiograph, the surgeon templates the femoral component to avoid anterior notching of the femoral cortex—a critical error that introduces a massive stress riser and significantly increases the risk of postoperative supracondylar femur fractures. Templating also aids in anticipating the need for augments or stems in cases of severe bone loss or profound deformity.
Patient Positioning and Anesthesia
The orchestration of the operating room and the positioning of the patient are critical first steps in surgical execution. The patient is placed supine on a standard radiolucent operating table. Regional anesthesia, specifically spinal anesthesia, is overwhelmingly preferred over general anesthesia. Spinal anesthesia has been definitively shown to reduce intraoperative blood loss, lower the incidence of deep vein thrombosis (DVT) by preserving venous tone, and provide superior immediate postoperative analgesia. This is frequently supplemented with an adductor canal block to provide targeted sensory blockade to the anterior knee while sparing quadriceps motor function, facilitating early mobilization.
The operative leg is placed in a specialized leg holder (such as a morph board or a standard lateral post) that allows for stable positioning during bone cuts and permits hyperflexion to at least 120 degrees. A pneumatic tourniquet is applied to the proximal thigh over copious cast padding. While the use of a tourniquet is surgeon-dependent, it is traditionally inflated just prior to the incision to provide a bloodless surgical field, thereby improving visualization and theoretically enhancing the penetration of polymethylmethacrylate (PMMA) bone cement into the cancellous bone bed.
Standard sterile orthopedic draping is utilized. It is imperative that the draping technique leaves the hip and ankle freely accessible or easily palpable, allowing the surgeon to intraoperatively assess the overall mechanical alignment of the limb using alignment rods or navigation arrays. An impervious U-drape is used to seal the operative field, minimizing the risk of contamination from the perineal region.
Step-by-Step Surgical Approach and Fixation Technique
Surgical Approach and Exposure
The standard medial parapatellar approach remains the undisputed workhorse of total knee arthroplasty, providing unparalleled, extensile exposure to all compartments of the knee. A midline longitudinal skin incision is made, extending from approximately 3 to 4 cm proximal to the superior pole of the patella down to the medial aspect of the tibial tubercle. Full-thickness fasciocutaneous flaps are meticulously elevated to preserve the subdermal vascular plexus, minimizing the risk of postoperative skin necrosis.
The arthrotomy begins proximally in the quadriceps tendon, leaving a sufficient medial cuff of tendon for robust closure. The incision skirts the medial border of the patella, preserving 2 to 3 mm of the medial retinaculum, and extends distally along the medial border of the patellar tendon to the tibial tubercle.
Once the capsule is incised, the patella is either everted or laterally subluxated into the lateral gutter, depending on the surgeon's preference and the tension of the extensor mechanism. Subluxation is increasingly favored as it reduces tension on the patellar tendon insertion, mitigating the risk of catastrophic avulsion. The deep infrapatellar fat pad is partially excised to visualize the lateral tibial plateau, taking extreme care not to damage the patellar tendon. The medial and lateral menisci, along with the anterior cruciate ligament (ACL), are sharply excised. If a posterior-stabilized design is chosen, the PCL is also resected at this stage.
Axial Alignment and Bone Resection
The biomechanical success of the procedure hinges on the precise execution of the bone cuts. The goal is to resect an amount of bone equal to the thickness of the prosthetic components being implanted, thereby restoring the native joint line.
The distal femoral resection is typically performed first using an intramedullary alignment guide. A hole is drilled into the distal femur, slightly anterior to the origin of the PCL, and an intramedullary rod is inserted. The cutting block is set to the preoperatively templated valgus angle (usually 5 to 7 degrees) to ensure the cut is perpendicular to the mechanical axis of the femur.
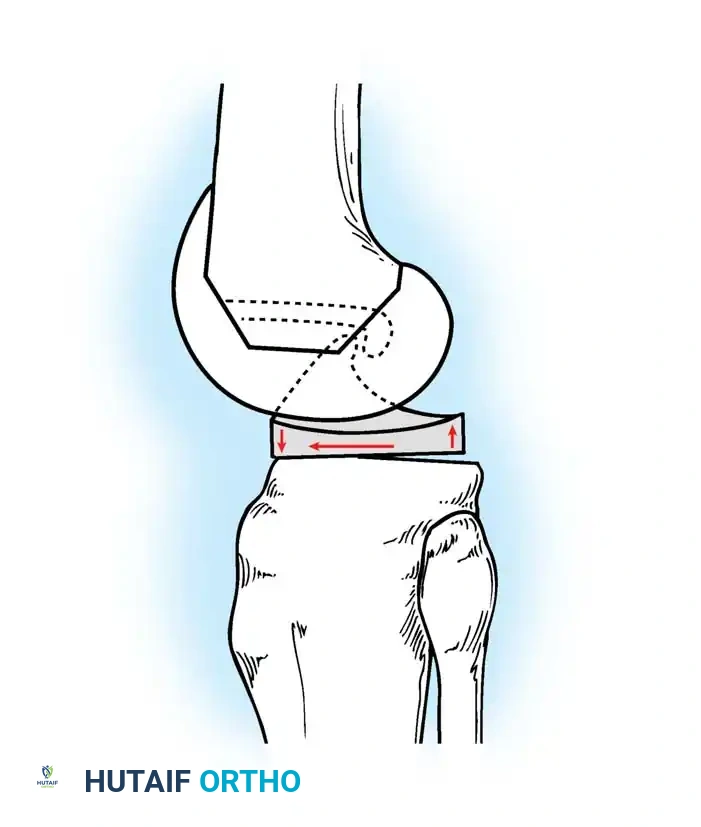
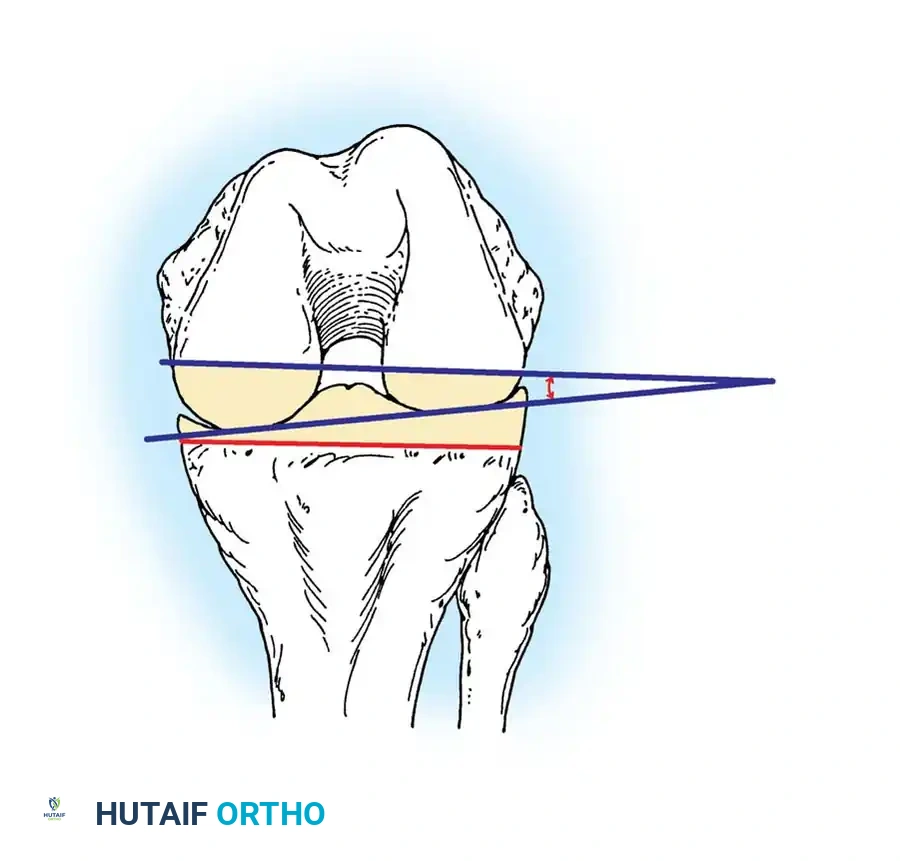
The proximal tibial resection is performed using an extramedullary alignment guide, referencing the center of the knee proximally and the center of the ankle (between the malleoli) distally. The cut is made perpendicular to the mechanical axis of the tibia in the coronal plane. In the sagittal plane, a posterior slope of 3 to 5 degrees is typically incorporated to match native anatomy and facilitate flexion, though this slope must be carefully tailored to the specific prosthesis design (CR vs. PS).
Rotational alignment of the femoral component is arguably the most critical and unforgiving step in TKA. Proper femoral rotation is essential for balancing the flexion gap and ensuring central, stable patellar tracking. The femoral component is typically externally rotated 3 degrees relative to the posterior condylar axis. This rotation compensates for the native 3 degrees of varus in the proximal tibia, ensuring a rectangular flexion gap. Intraoperatively, this rotation is cross-referenced using two primary anatomical landmarks:
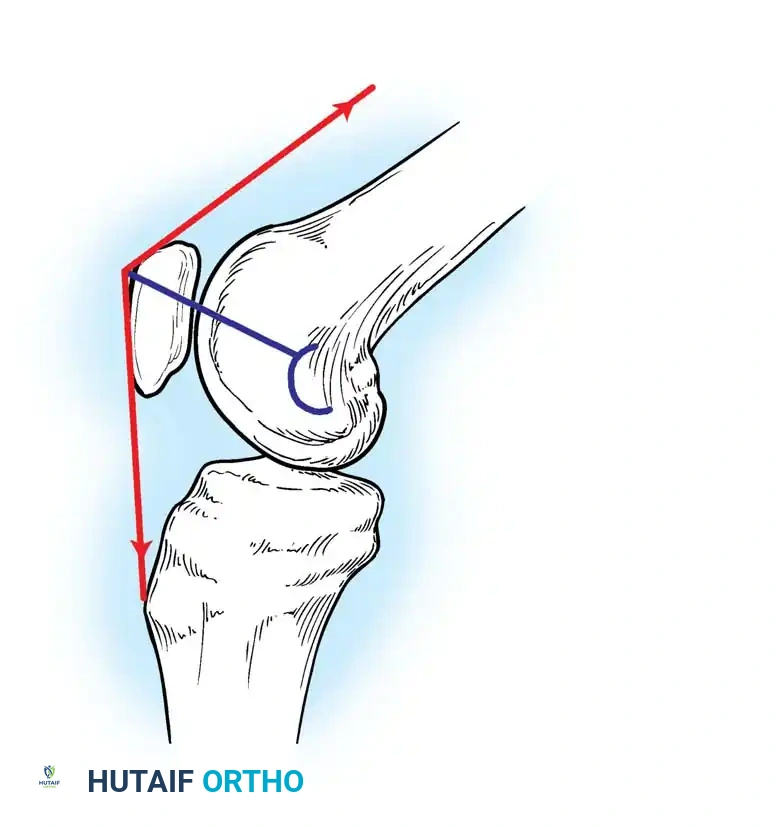
1. The Surgical Transepicondylar Axis (TEA): A line drawn from the most prominent aspect of the lateral epicondyle to the medial epicondylar sulcus. The femoral component should be placed parallel to this axis.
2. Whiteside’s Line (Anteroposterior Axis): A line drawn from the deepest part of the trochlear groove to the center of the intercondylar notch. The femoral component should be placed perpendicular to this axis.
Intraoperative Gap Balancing and Soft Tissue Management
The essence of a biomechanically sound TKA lies in creating equal, rectangular flexion and extension gaps. The surgeon must meticulously balance the bony resections against the tension of the surrounding soft tissue envelope.