Primary Tricompartmental Knee Replacement: Advanced Surgical Technique

Key Takeaway
Primary tricompartmental total knee arthroplasty (TKA) requires meticulous surgical technique, precise soft-tissue balancing, and accurate restoration of the mechanical axis. This comprehensive guide details the medial parapatellar, subvastus, and midvastus approaches, alongside advanced bone preparation principles. By mastering femoral rotational alignment and gap balancing techniques, orthopedic surgeons can optimize patellofemoral tracking, ensure joint stability, and significantly improve long-term functional outcomes for patients undergoing knee reconstruction.
Comprehensive Introduction and Patho-Epidemiology
Primary tricompartmental total knee arthroplasty (TKA) stands as one of the most successful and transformative surgical interventions in the history of modern orthopedics. Designed to alleviate debilitating pain and restore functional kinematics in patients suffering from end-stage arthropathy, TKA has evolved from a salvage procedure into a highly reproducible operation with exceptional long-term survivorship. The following comprehensive description of surgical technique encompasses the foundational and advanced principles applicable to primary tricompartmental knee reconstruction. While this guide provides an exhaustive academic framework, it is not intended to replace the individual technique manuals specific to proprietary implant systems. A profound understanding of the biomechanical principles involved allows the orthopedic surgeon to exercise sound clinical judgment in any knee reconstruction, regardless of the particular type of implant or constraint level being utilized.
The patho-epidemiology of knee arthritis is predominantly driven by primary osteoarthritis (OA), which accounts for the vast majority of TKA indications. Osteoarthritis is a progressive, degenerative disease characterized by articular cartilage degradation, subchondral bone sclerosis, osteophyte formation, and variable degrees of synovial inflammation. The global burden of OA is staggering, with demographic shifts toward an aging population and rising obesity rates driving an exponential increase in the demand for joint arthroplasty. Projections indicate that the annual volume of primary TKA procedures will continue to surge, necessitating a rigorous understanding of both the procedure and the perioperative optimization required to minimize complications.
Beyond primary osteoarthritis, orthopedic surgeons must be adept at managing secondary arthritides. Rheumatoid arthritis (RA) and other inflammatory arthropathies present unique challenges, including profound osteopenia, severe soft-tissue attenuation, and multi-joint involvement that complicates rehabilitation. Post-traumatic arthritis, often resulting from prior intra-articular tibial plateau or distal femoral fractures, introduces complexities such as retained hardware, distorted anatomic landmarks, compromised soft-tissue envelopes, and latent infection. Regardless of the underlying etiology, the ultimate goal of tricompartmental TKA remains consistent: the precise resection of diseased articular surfaces and the restoration of a stable, well-aligned, and kinematically functional joint.
To achieve these goals, the modern arthroplasty surgeon must synthesize a deep knowledge of functional anatomy, biomechanics, and materials science. The transition from traditional mechanical alignment philosophies—which strive to place the components strictly perpendicular to the mechanical axes of the femur and tibia—to more contemporary concepts such as kinematic or restricted kinematic alignment requires an intimate understanding of the native knee's complex motion. This chapter will meticulously detail the surgical execution of primary TKA, providing the academic surgeon with the foundational knowledge required to navigate both routine and highly complex primary reconstructions.
Detailed Surgical Anatomy and Biomechanics
A masterful execution of a primary tricompartmental TKA demands an encyclopedic knowledge of the knee's surgical anatomy and its complex biomechanical behavior. The knee is not a simple hinge joint; it operates with six degrees of freedom, encompassing flexion/extension, internal/external rotation, varus/valgus angulation, anterior/posterior translation, medial/lateral translation, and proximal/distal translation. The intricate interplay between the osseous geometry and the dynamic soft-tissue envelope dictates these kinematic patterns.
The distal femur features two distinct condyles that articulate with the tibial plateau and the patella. The medial femoral condyle is larger, more curved, and extends further distally than the lateral condyle, acting essentially as a ball-and-socket joint during the arc of motion. Conversely, the lateral femoral condyle has a flatter sagittal profile, facilitating the posterior rollback of the femur on the tibia during deep flexion. This asymmetric rollback is driven by the anterior cruciate ligament (ACL) and the posterior cruciate ligament (PCL), which act as a crossed four-bar linkage system. In TKA, the sacrifice of the ACL (and often the PCL) dramatically alters these native kinematics, requiring the prosthetic design—whether cruciate-retaining (CR), posterior-stabilized (PS), or medial-pivot—to compensate for the lost ligamentous restraints.
The soft-tissue envelope is the primary determinant of coronal and sagittal stability. The medial collateral ligament (MCL) complex consists of the superficial MCL, which provides primary resistance to valgus stress across the entire arc of motion, and the deep MCL (meniscofemoral and meniscotibial ligaments), which acts as a secondary restraint. On the lateral side, the lateral collateral ligament (LCL), popliteus tendon, and the iliotibial (IT) band form a complex posterolateral corner that resists varus stress and external rotatory instability. During TKA, meticulous soft-tissue balancing is paramount; the surgeon must sequentially release contracted structures to create symmetric, rectangular flexion and extension gaps. Failure to respect the distinct tensioning of these ligaments leads to kinematic conflict, accelerated polyethylene wear, and clinical instability.
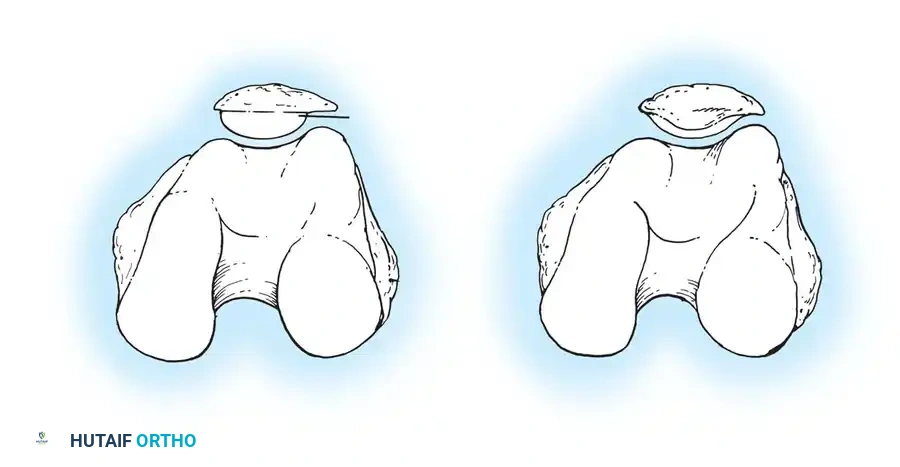
The extensor mechanism, comprising the quadriceps tendon, patella, and patellar tendon, is critical for knee function and is often the source of post-operative dissatisfaction if mishandled. The patella acts as a fulcrum, increasing the moment arm of the quadriceps muscle. Optimal patellofemoral tracking depends on the precise rotational alignment of the femoral and tibial components, the restoration of the native joint line, and the appropriate resurfacing of the patellar dome. Internal rotation of the femoral or tibial components increases the Q-angle, leading to lateral patellar subluxation, anterior knee pain, and catastrophic extensor mechanism failure.
Exhaustive Indications and Contraindications
The decision to proceed with primary tricompartmental TKA must be predicated on a rigorous clinical evaluation, radiographic evidence of end-stage joint destruction, and the exhaustion of non-operative modalities. The primary indication for TKA is recalcitrant pain that significantly impairs the patient's activities of daily living and quality of life. Non-operative management—including weight loss, physical therapy, non-steroidal anti-inflammatory drugs (NSAIDs), intra-articular corticosteroid injections, and viscosupplementation—must be thoroughly trialed and documented as ineffective before surgical intervention is offered.
Patient selection is arguably the most critical determinant of a successful outcome. The orthopedic surgeon must meticulously evaluate the patient's medical comorbidities, psychological readiness, and functional expectations. Pre-operative optimization is mandatory; parameters such as glycemic control (HbA1c < 7.5%), body mass index (BMI < 40 kg/m²), smoking cessation, and nutritional status must be addressed to mitigate the risk of perioperative complications, particularly periprosthetic joint infection (PJI) and wound healing failures.
The following table delineates the established indications, absolute contraindications, and relative contraindications for primary TKA.
| Category | Clinical Parameters and Conditions |
|---|---|
| Primary Indications | End-stage osteoarthritis with debilitating pain; Rheumatoid arthritis with severe structural damage; Post-traumatic arthritis failing conservative care; Severe functional impairment limiting ADLs. |
| Absolute Contraindications | Active local or systemic infection (e.g., bacteremia); Neuropathic (Charcot) arthropathy (relative in highly specialized centers, but generally absolute); Severe peripheral vascular disease precluding wound healing; Functionless extensor mechanism; Terminal illness with life expectancy < 6 months. |
| Relative Contraindications | Morbid obesity (BMI > 40-45 kg/m²); Poorly controlled diabetes mellitus (HbA1c > 8.0%); Active smoking or nicotine use; Severe osteoporosis (risk of periprosthetic fracture); Non-compliance or severe psychiatric disorders; History of prior joint infection (requires extensive workup). |
In cases of relative contraindications, the surgeon must engage in extensive shared decision-making with the patient, explicitly detailing the exponentially higher risks of complications. For instance, performing a TKA on a patient with a functionless extensor mechanism will inevitably lead to profound instability and failure, necessitating complex salvage procedures such as extensor mechanism allograft reconstruction or arthrodesis.
Pre-Operative Planning, Templating, and Patient Positioning
Successful TKA begins long before the first incision. Meticulous preoperative templating using weight-bearing full-length standing radiographs is mandatory. These images allow the surgeon to determine the mechanical axis of the lower extremity, assess the extent and location of bone loss, anticipate the need for augments or stems, and estimate the appropriate implant sizing. The mechanical axis of the femur is defined by a line connecting the center of the femoral head to the center of the intercondylar notch, while the anatomical axis follows the intramedullary canal. The angle between these two axes—typically 5 to 7 degrees of valgus—dictates the distal femoral resection angle.
Advanced pre-operative planning may also incorporate computed tomography (CT) or magnetic resonance imaging (MRI) for robotic-assisted or patient-specific instrumentation (PSI) cases. These three-dimensional modalities offer unparalleled precision in pre-determining component sizing, rotational alignment, and the exact depth of bone resections, thereby minimizing intra-operative guesswork and reducing operative time.
The patient is positioned supine on the operating table. A well-padded tourniquet is applied to the proximal thigh, ensuring it is positioned high enough to prevent impingement on the vastus lateralis during the surgical approach. The leg is prepped and draped free to allow full, unhindered flexion to at least 120 degrees and complete extension. A lateral post or a dedicated knee positioner is often utilized to maintain the limb in flexion during critical stages of the procedure, providing a stable platform for bone resection and cementation.
💡 Clinical Pearl: Tourniquet Management
While traditional TKA utilizes a tourniquet inflated to 250–300 mm Hg prior to incision, modern protocols often favor a "tourniquet-less" approach or delayed inflation (only during cementation). This paradigm shift aims to reduce postoperative pain, minimize quadriceps inhibition, lower the risk of deep vein thrombosis (DVT), and allow for meticulous intra-operative hemostasis.
Careful attention must be paid to the padding of the contralateral limb to prevent iatrogenic nerve palsies, particularly of the common peroneal nerve. The operative suite should be optimized for efficiency, with all necessary proprietary instrumentation, backup implant sizes, and potential revision components (e.g., tibial stems, augments) readily available in the room prior to the induction of anesthesia.
Step-by-Step Surgical Approach and Fixation Technique
The execution of a primary tricompartmental TKA is a highly choreographed sequence of soft-tissue mobilization, precise osseous resection, kinematic balancing, and rigid component fixation. The following subsections detail the advanced surgical techniques required to achieve a reproducible and durable reconstruction.
Surgical Approaches to the Knee
The most commonly used skin incision for primary TKA is an anterior midline incision. The choice of deep arthrotomy dictates the exposure of the joint and influences postoperative quadriceps recovery.
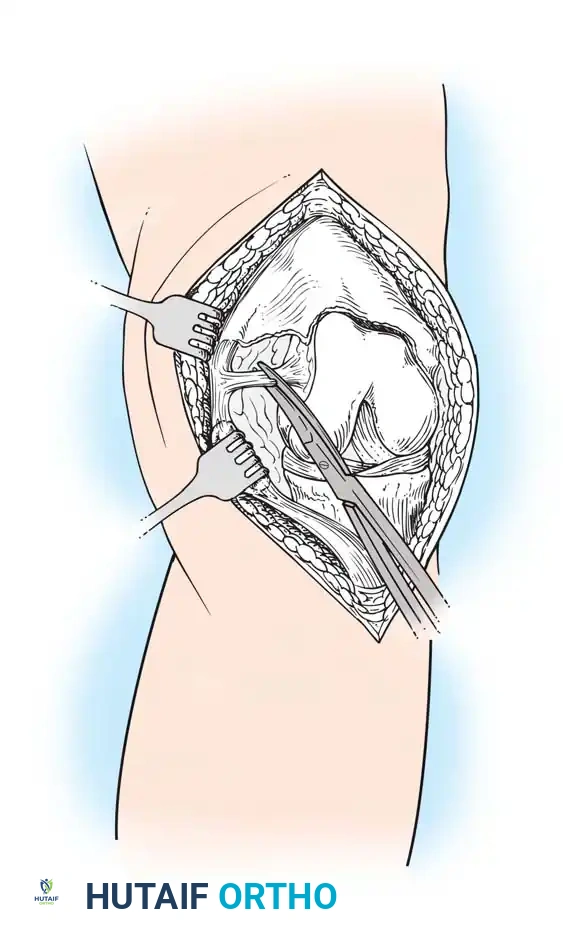
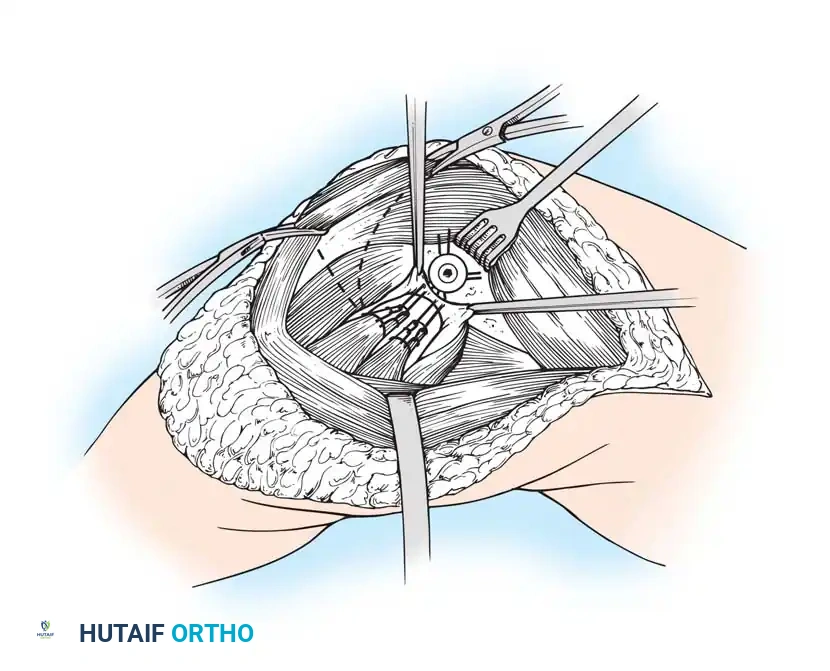
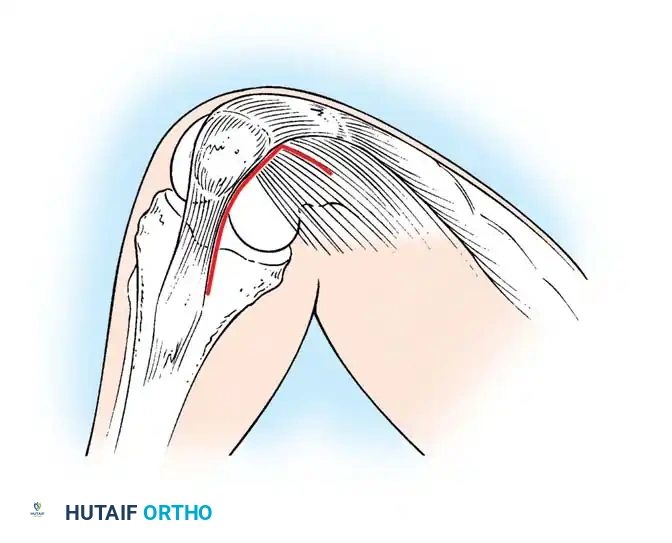
The Medial Parapatellar Retinacular Approach
The standard and most versatile retinacular incision in TKA is the medial parapatellar approach. It provides extensile exposure and is suitable for nearly all primary and revision scenarios.
- Make the skin incision with the knee in flexion. This allows the subcutaneous tissue to fall medially and laterally, naturally improving exposure.
- If a preexisting anterior scar is present in a usable position, incorporate it. If multiple previous incisions exist, choose the most lateral usable incision. The blood supply to the skin of the anterior knee predominantly arises from the medial side; violating this principle risks catastrophic skin necrosis.
- Ensure the skin incision is long enough to avoid excessive tension during retraction.
- Keep the medial skin flap as thick as possible by maintaining dissection just superficial to the extensor mechanism.
- Extend the retinacular incision proximally along the length of the quadriceps tendon, leaving a 3- to 4-mm cuff of tendon on the vastus medialis to facilitate robust closure.
- Continue the incision around the medial border of the patella, extending 3 to 4 cm onto the anteromedial surface of the tibia, parallel to the medial border of the patellar tendon.
- Expose the medial side of the knee by subperiosteally elevating the anteromedial capsule and the deep medial collateral ligament (MCL) off the tibia, extending to the posteromedial corner of the knee.
- Extend the knee and evert the patella. This allows for a routine release of the lateral patellofemoral plicae. In obese patients, if eversion is difficult, develop the lateral subcutaneous flap further so the patella can be everted underneath this tissue without avulsing the patellar tendon.
⚠️ Surgical Warning: Patellar Tendon Avulsion
During all maneuvers that place tension on the extensor mechanism—especially knee flexion and patellar retraction—pay careful attention to the patellar tendon attachment at the tibial tubercle. Avulsion of the patellar tendon is a devastating complication that is notoriously difficult to repair.
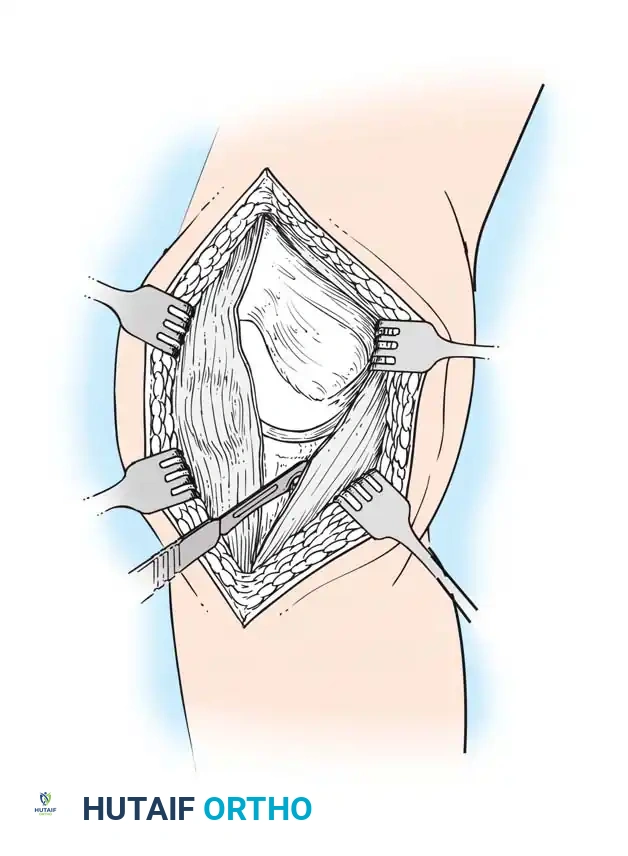
The Subvastus ("Southern") Approach
In an effort to reduce patellofemoral complications and expedite the return of quadriceps function, alternative methods of exposure have been developed. The subvastus approach avoids violating the extensor mechanism entirely.
- The same anterior midline skin incision is used.
- The proximal retinacular incision is performed by incising the superficial fascia overlying the vastus medialis.
- Bluntly mobilize the distal medial border of the vastus medialis posteriorly to the medial intermuscular septum.
- Lift the origin of the vastus medialis off the medial intermuscular septum to approximately 10 cm proximal to the adductor tubercle, staying distal to the aperture for the femoral vessels.
- Incise the synovium and dislocate the entire extensor mechanism laterally.
Advocates of the subvastus approach note that leaving the extensor mechanism intact results in a more rapid return of quadriceps strength, preserves the vascularity to the patella (specifically the supreme genicular artery), decreases postoperative pain, and reduces the need for lateral retinacular release. However, exposure can be severely limited in obese patients, highly muscular individuals, or those with previous knee surgeries.
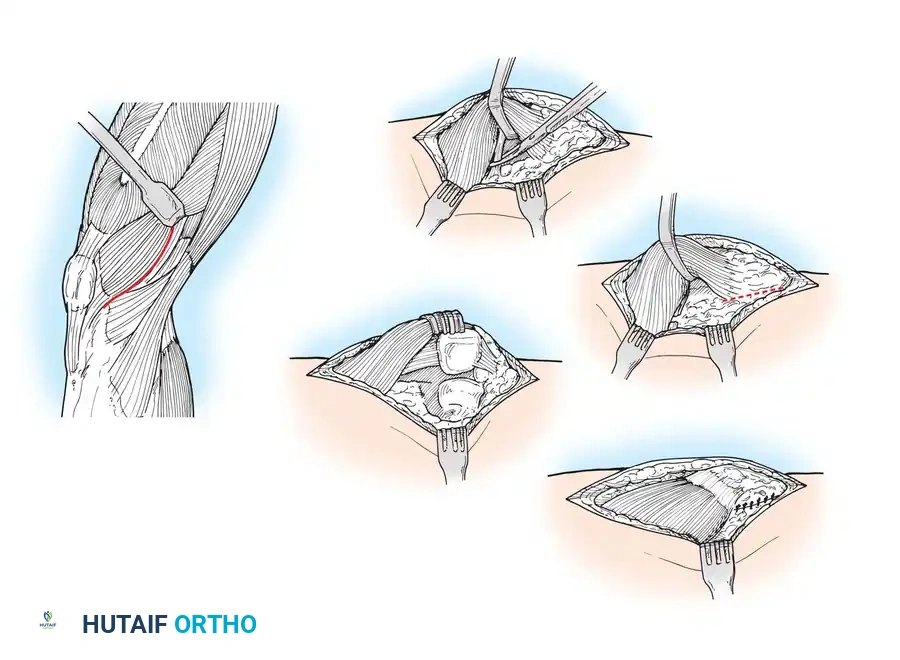
The Midvastus Approach
The midvastus approach serves as a compromise between the extensile nature of the medial parapatellar and the quadriceps-sparing nature of the subvastus approach.
- The vastus medialis muscle is split in line with its fibers rather than subluxated laterally in its entirety.
- The split begins at the superomedial border of the patella and extends proximally and medially toward the intermuscular septum.
- A safe zone of 4.5 cm of the vastus medialis can be sharply split from the patellar margin; further blunt dissection can be performed if necessary to avoid denervating the muscle.
This approach preserves the supreme genicular artery and the quadriceps tendon. Relative contraindications include severe obesity, previous upper tibial osteotomy, and preoperative flexion of less than 80 degrees. Careful hemostasis is mandatory, as postoperative hematomas are more frequently described with muscle-splitting approaches.
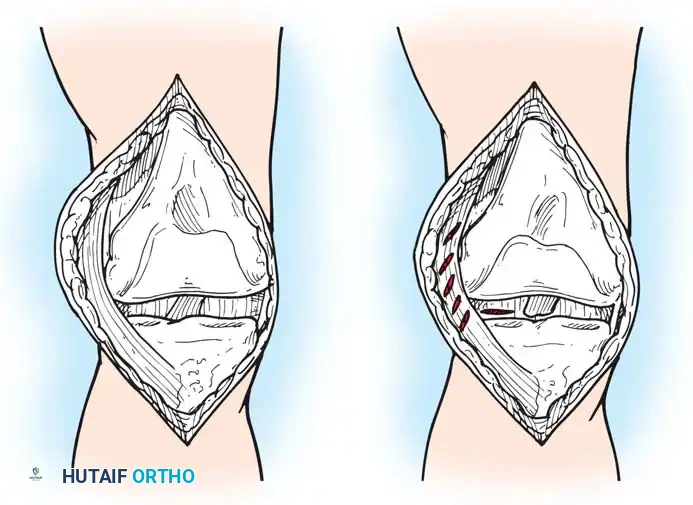
Initial Joint Preparation and Soft Tissue Management
Once the joint is exposed, systematic preparation of the intra-articular structures is required before bone resection. The goal is to clear the joint of obstructing pathology to allow for accurate placement of cutting guides.
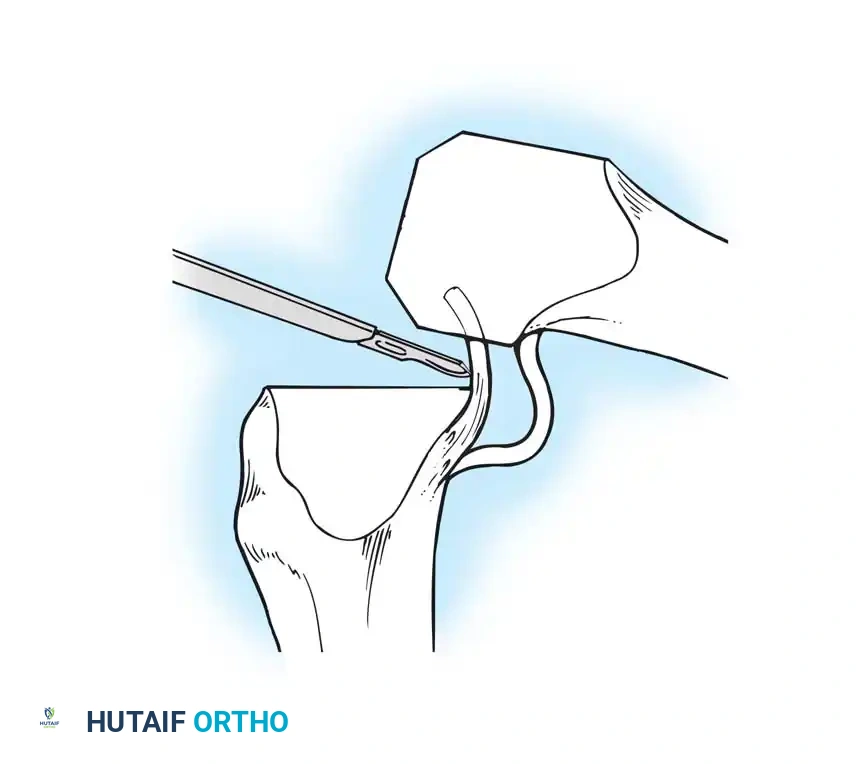
- Flex the knee and excise the anterior cruciate ligament (ACL) and the anterior horns of the medial and lateral menisci.
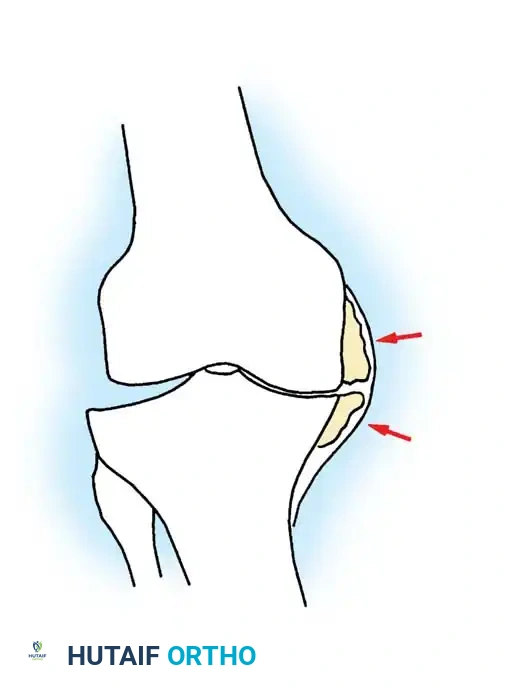
- Remove any prominent osteophytes (especially in the intercondylar notch and medial/lateral gutters) that may lead to component malposition, impinge on soft tissues, or create artificial soft-tissue tension.
- The posterior horns of the menisci are often easier to excise after the initial femoral and tibial bone cuts have been made.
- If a Posterior Cruciate Ligament (PCL)-substituting (Posterior Stabilized, PS) prosthesis is planned, the PCL can be resected now or removed later during the intercondylar box cut.
- With both PCL-substituting and PCL-retaining procedures, subluxate and externally rotate the tibia. External rotation relaxes the extensor mechanism, decreases the risk of patellar tendon avulsion, and dramatically improves exposure of the lateral compartment.
- Expose the lateral tibial plateau by partially excising the infrapatellar fat pad and carefully placing a levering-type retractor adjacent to the lateral tibial plateau.

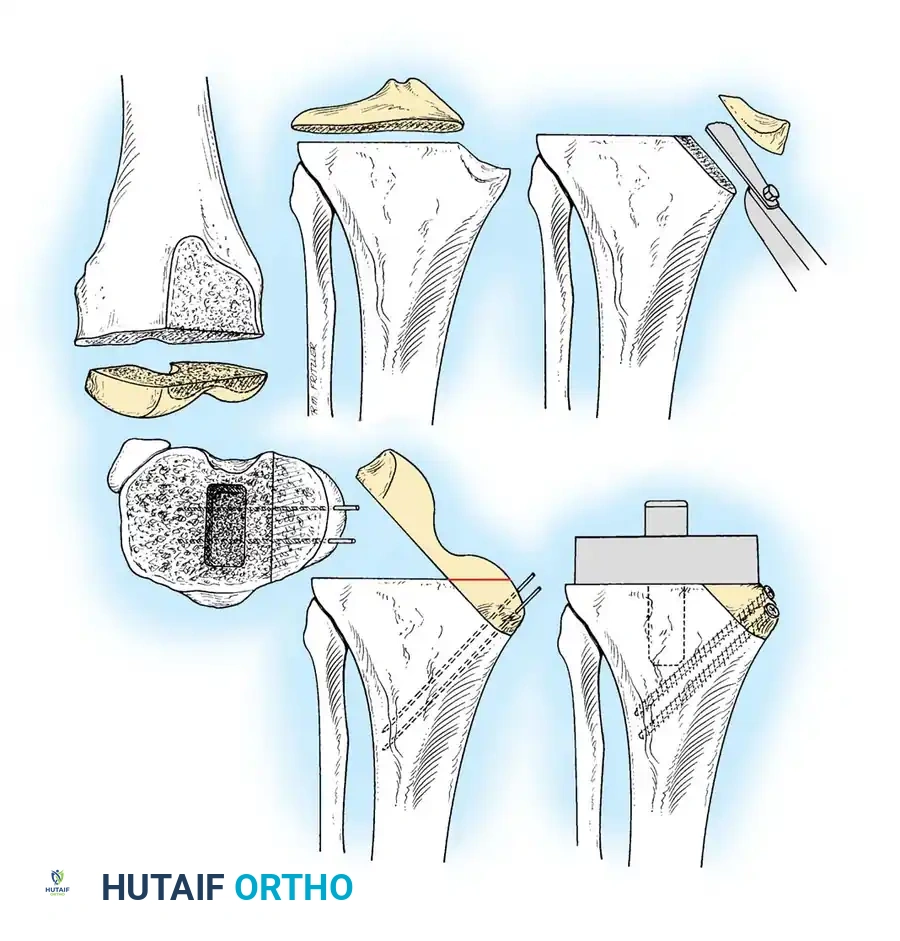
Principles of Bone Preparation
Bone surface preparation is governed by four non-negotiable principles:
1. Appropriate sizing of the individual components to prevent overstuffing or under-coverage.
2. Alignment of the components to restore the neutral mechanical axis (or desired kinematic target).
3. Recreation of equally balanced, rectangular soft-tissue gaps in both flexion and extension.
4. Optimization of patellofemoral tracking through meticulous rotational alignment.
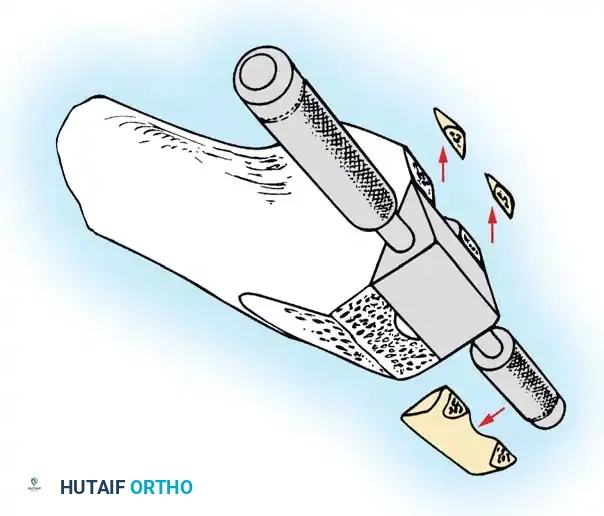
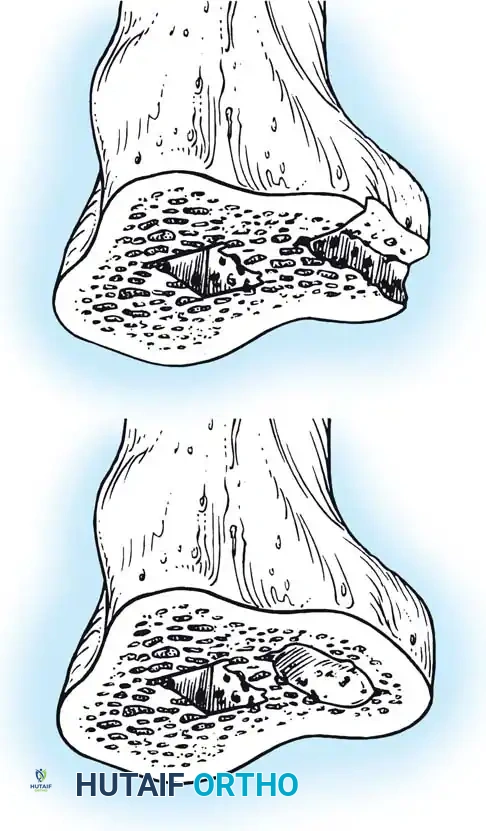
Distal Femoral Resection
The distal femoral cut sets the extension gap and determines the coronal alignment of the femoral component.
- Make the distal femoral cut at a valgus angle (usually 5 to 7 degrees) perpendicular to the predetermined mechanical axis of the femur. This is typically achieved using an intramedullary alignment guide introduced just anterior to the origin of the PCL.
- The thickness of the bone removed should generally equal the thickness of the distal flange of the femoral component (typically 9 to 10 mm), adjusting for cartilage wear.
- If a significant preoperative flexion contracture is present, removing an additional 2 to 3 mm of distal femoral bone will widen the extension gap, aiding in contracture correction without affecting the flexion gap.
Femoral Rotational Alignment
The anterior and posterior femoral cuts determine the rotation of the femoral component and the shape of the flexion gap. This is arguably the most critical step in TKA, as malrotation is poorly tolerated.
* Excessive external rotation widens the flexion gap medially, potentially resulting in medial flexion instability and a tight lateral compartment.
* Internal rotation of the femoral component is a primary cause of lateral patellar tilt, patellofemoral instability, anterior knee pain, and early failure.
Femoral component rotation can be determined using several anatomical and kinematic reference axes:
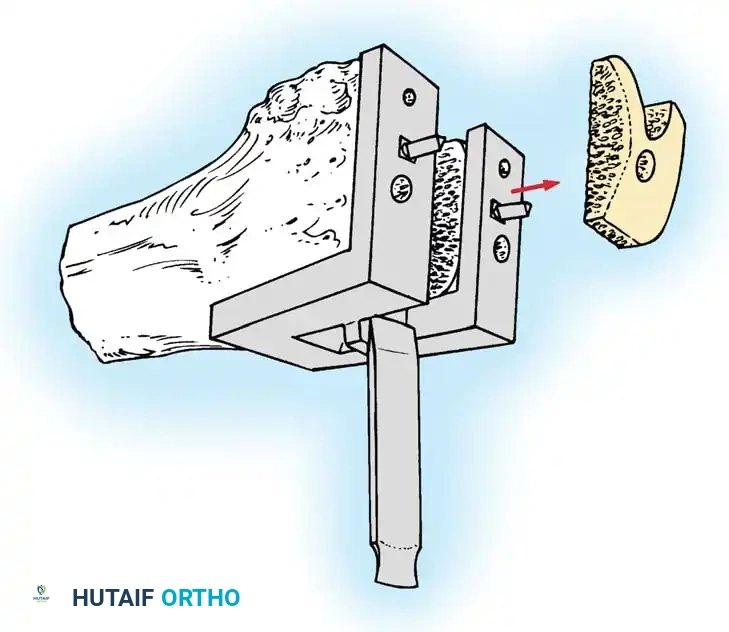
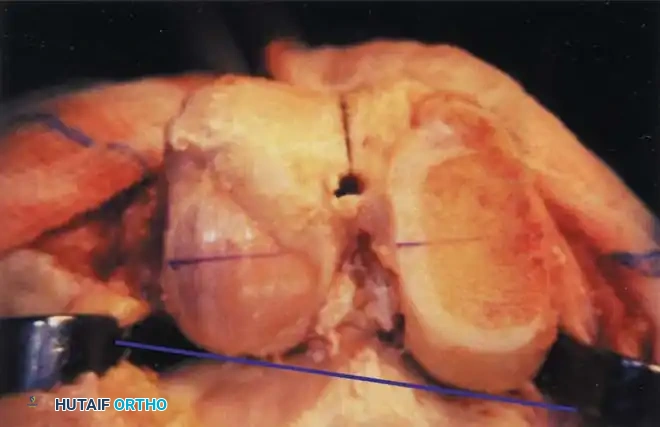
- The Surgical Transepicondylar Axis (TEA): Make the posterior femoral cut parallel to a line drawn between the prominence of the lateral epicondyle and the sulcus of the medial epicondyle. This represents the functional axis of knee flexion.
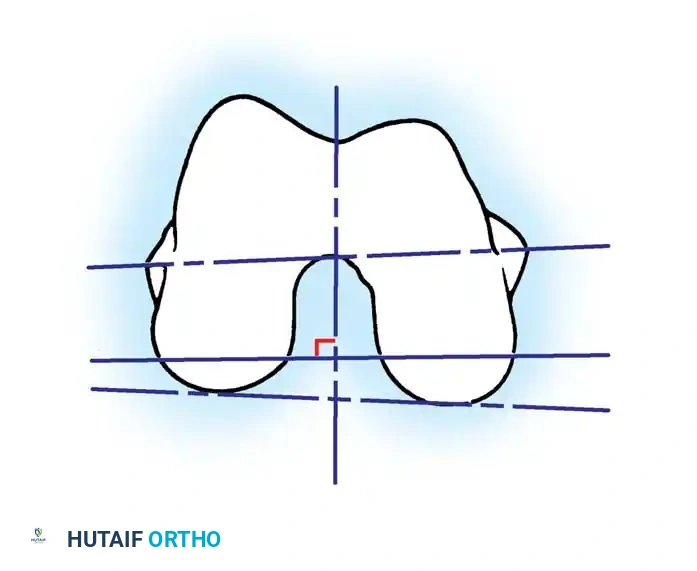
- The Anteroposterior (AP) Axis (Whiteside's Line): Draw a line from the deepest part of the trochlear groove to the center of the intercondylar notch. The posterior femoral cut is made perpendicular to this axis.
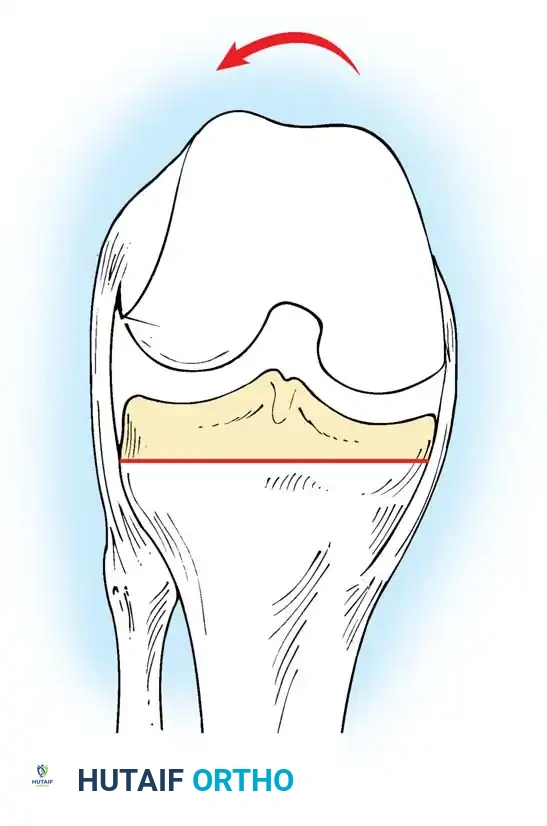
- The Posterior Condylar Axis (PCA): When referencing the posterior condyles, the cut is typically made in 3 degrees of external rotation relative to a line connecting the most posterior aspects of the medial and lateral condyles.
⚠️ Pitfall: The Hypoplastic Lateral Condyle
In the valgus knee, the lateral femoral condyle is frequently hypoplastic. Relying solely on the posterior condylar axis in a valgus knee will lead to an internally rotated femoral component. In these cases, the TEA or AP axis must be prioritized to prevent catastrophic patellofemoral maltracking.
- The Gap Technique: Using the cut surface of the proximal tibia, the posterior femoral cut is made parallel to the proximal tibial cut after the soft tissues have been balanced in extension.
Caution must be exercised when using the gap technique; reliance on ligaments that have stretched or contracted to nonanatomical lengths can lead to severe femoral component malrotation. The master surgeon cross-references multiple axes to ensure perfect rotational alignment.
Anterior vs. Posterior Referencing
Regardless of the rotational alignment method, the sizing of the femoral component dictates the flexion space.
* Posterior Referencing: Instruments measure from the posterior condyles. This method accurately recreates the original posterior condylar offset, optimizing the flexion gap. However, if the femur is between sizes, sizing up can overstuff the patellofemoral joint, while sizing down risks notching the anterior femoral cortex, creating a stress riser for periprosthetic fracture.
* Anterior Referencing: Instruments measure from the anterior cortex. This method reliably places the anterior flange flush against the bone, virtually eliminating the risk of anterior notching. However, sizing down may increase the flexion gap (leading to instability), while sizing up may tighten the flexion gap.