Tibial-Calcaneal Arthrodesis for Talar Loss, AVN, and Infection: A Masterclass

Key Takeaway
Join us in the OR for a masterclass on tibial-calcaneal arthrodesis, a critical salvage procedure for severe talar bone loss, avascular necrosis, and chronic infection. We'll meticulously cover preoperative planning, comprehensive débridement, antibiotic bead application, precise bone preparation, and the intricate application of circular tensioned wire fixators, ensuring a stable, infection-free fusion and limb salvage.
Comprehensive Introduction and Patho-Epidemiology
The management of severe talar bone loss, complicated by avascular necrosis (AVN) and chronic osteomyelitis, represents one of the most formidable challenges in orthopedic limb salvage. The talus functions as the critical intercalated segment connecting the leg to the foot, transmitting the entire weight of the human body through its complex articular surfaces. When high-energy trauma—such as a severe fracture-dislocation or a crushing injury—disrupts this intricate biomechanical linkage, the consequences are often catastrophic. This is not merely a matter of fusing two adjacent bones; it is a highly complex, multi-staged reconstructive effort aimed at salvaging a functional limb, restoring weight-bearing capacity, and permanently eradicating a virulent, deep-seated infection.
The etiology of this devastating triad—bone loss, AVN, and infection—is almost exclusively rooted in high-energy trauma. Severe talar neck or body fractures, particularly those that are open or associated with complete extrusion of the talus, severely compromise the tenuous blood supply to the bone. When these injuries are compounded by gross contamination or subsequent postoperative surgical site infections following internal fixation, the surgeon is faced with an infected nonunion. In this environment, infection prevents osteogenesis and perpetuates tissue destruction, leading to progressive osteolysis and structural collapse. The presence of necrotic bone acts as a persistent nidus for bacterial biofilm formation, rendering systemic antibiotic therapy largely ineffective without aggressive surgical intervention.
The ramifications of complete talar excision (talectomy), which is frequently necessitated by overwhelming necrosis and infection, are profound. The immediate consequence is a substantial leg length discrepancy, typically ranging from 3 to 4 centimeters, depending on the patient's native anatomy. Furthermore, the loss of the talus eliminates the normal kinematic function of the ankle and subtalar joints, fundamentally altering the biomechanics of the lower extremity. The soft tissue envelope, already compromised by the initial trauma and subsequent surgeries, becomes scarred, tenuous, and contracted. Addressing these compounding issues requires a comprehensive, meticulously planned surgical strategy that prioritizes infection eradication above all else, followed by the establishment of a stable, rigid tibial-calcaneal arthrodesis.
In this masterclass, we will systematically deconstruct the approach to this complex pathology. We will explore the critical surgical anatomy that dictates our operative corridors, the exhaustive preoperative planning required to optimize the host, and the step-by-step execution of a staged tibial-calcaneal arthrodesis. Our ultimate objective is to provide the orthopedic surgeon with a definitive, evidence-based framework for navigating the treacherous waters of hindfoot limb salvage, transforming a chronically infected, non-functional extremity into a stable, plantigrade, and pain-free limb.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of the surgical anatomy of the hindfoot is the absolute prerequisite for executing a successful tibial-calcaneal arthrodesis, particularly in the setting of distorted architecture and scarred tissue planes. The talus is anatomically unique; approximately 60% to 70% of its surface area is covered by hyaline cartilage, leaving highly restricted vascular portals for arterial ingress. It possesses no muscular or tendinous attachments, relying entirely on its ligamentous and capsular connections for its blood supply. This architectural isolation is the primary reason the talus is so exquisitely vulnerable to ischemic necrosis following traumatic dislocation.
The vascularity of the talus is derived from an anastomotic sling formed by the three major arteries of the lower leg. The posterior tibial artery provides the most significant contribution via the artery of the tarsal canal, which supplies the majority of the talar body. The anterior tibial artery contributes via branches from the dorsalis pedis to the talar neck and head. The peroneal artery forms anastomoses in the sinus tarsi. Disruption of the artery of the tarsal canal, which frequently occurs in displaced talar neck fractures (Hawkins Type II-IV), initiates the cascade of avascular necrosis. Understanding this vascular map is critical not only for comprehending the pathogenesis of AVN but also for planning surgical approaches that preserve any remaining vascularity to the adjacent tibial plafond and calcaneus.
When executing the anteromedial approach for talectomy and debridement, the surgeon must navigate a specific neurovascular corridor. The incision is typically placed just medial to the tibialis anterior tendon. In this superficial plane, the great saphenous vein and the saphenous nerve are at risk and must be meticulously identified and retracted medially. Deep to the extensor retinaculum, the anterior tibial neurovascular bundle—comprising the deep peroneal nerve and the anterior tibial artery—lies lateral to the extensor hallucis longus tendon. Retracting the entire anterior compartment musculature laterally protects this critical bundle while providing expansive access to the anterior ankle joint capsule, the medial malleolus, and the talar neck.
Conversely, lateral or transfibular approaches require strict attention to the sural nerve and the peroneal tendons. The sural nerve courses posterior to the lateral malleolus and is highly susceptible to iatrogenic injury during lateral incisions. The peroneal tendons (longus and brevis) must be mobilized and protected. If a transfibular approach is utilized—often necessary for optimal visualization of the posterior facet of the calcaneus and for utilizing the fibula as a biological bone graft—the distal fibula is osteotomized. This approach provides unparalleled access to the lateral aspect of the subtalar joint and the lateral process of the talus, facilitating comprehensive debridement and subsequent preparation of the calcaneal and tibial surfaces for rigid internal fixation.
Exhaustive Indications and Contraindications
The decision to proceed with a tibial-calcaneal arthrodesis in the setting of infection and bone loss is a critical juncture in patient care. It is a limb salvage procedure that must be weighed carefully against the alternative: a primary below-knee amputation (BKA). Patient selection, host optimization, and a realistic discussion of functional expectations are paramount.
| Category | Specific Criteria | Rationale / Clinical Context |
|---|---|---|
| Absolute Indications | Severe Talar AVN with Structural Collapse | Loss of articular congruity and mechanical support necessitates structural bypass via arthrodesis. |
| Chronic, Refractory Talar Osteomyelitis | Infection that has failed suppressive antibiotics and localized debridement requires complete resection of the infected nidus (the talus). | |
| Massive Traumatic Talar Extrusion/Loss | Direct physical absence of the talus requires reconstruction of the intercalated defect to restore weight-bearing. | |
| Relative Indications | Failed Total Ankle Arthroplasty (TAA) with severe bone loss | When revision TAA is impossible due to inadequate bone stock, conversion to a tibiotalocalcaneal or tibiocalcaneal fusion is required. |
| Severe Neuropathic (Charcot) Arthropathy | Extensive fragmentation and instability may require talectomy and rigid realignment to prevent ulceration and amputation. | |
| Absolute Contraindications | Active, Untreated Systemic Sepsis | Systemic stabilization must precede complex, prolonged local reconstructive efforts. |
| Non-Reconstructable Vascular Compromise | An ischemic limb with an ABI < 0.4 or absent flow on angiography that cannot be bypassed will not heal a fusion and requires amputation. | |
| Inadequate Soft Tissue Envelope | If soft tissue coverage cannot be achieved (via local or free flaps) over the hardware and bone, the procedure will fail. | |
| Relative Contraindications | Severe Medical Comorbidities (ASA IV) | High perioperative mortality risk may make a definitive, shorter BKA preferable to a prolonged, multi-staged salvage. |
| Active Smoking / Nicotine Use | Profoundly increases the risk of nonunion and wound breakdown; cessation is mandatory prior to elective reconstruction. | |
| Poor Patient Compliance | The multi-staged nature, prolonged non-weight-bearing, and potential for external fixation require rigorous patient adherence to protocols. |
The physiological status of the host plays a determinative role in the success of this procedure. Utilizing the Cierny-Mader classification system for osteomyelitis, we must differentiate between A-hosts (healthy), B-hosts (systemically or locally compromised), and C-hosts (where the morbidity of treatment outweighs the disease). A significant proportion of these patients are B-hosts due to diabetes, peripheral vascular disease, smoking, or chronic immunosuppression. Optimization of these factors—achieving strict glycemic control (HbA1c < 7.0%), initiating smoking cessation protocols, and maximizing nutritional parameters (albumin, prealbumin)—is not optional; it is a mandatory prerequisite for attempting limb salvage.
Furthermore, the psychological readiness of the patient cannot be overstated. A tibial-calcaneal arthrodesis, particularly when staged for infection, requires months of restricted weight-bearing, multiple trips to the operating room, and a high likelihood of utilizing external fixation or prolonged intravenous antibiotics. The surgeon must engage in exhaustive shared decision-making, clearly outlining that while the goal is limb salvage, the functional outcome will be a shortened, stiff hindfoot. For some patients, particularly those desiring a rapid return to high-demand physical labor, a well-constructed below-knee amputation with a modern prosthesis may offer a superior, more predictable functional result.
Pre-Operative Planning, Templating, and Patient Positioning
Success in complex hindfoot reconstruction is inextricably linked to the meticulousness of preoperative planning. The surgeon must conceptualize the three-dimensional deformity, quantify the exact volume of bone loss, identify the precise microbial pathogens, and formulate a definitive, staged surgical blueprint before the patient ever enters the operating theater.


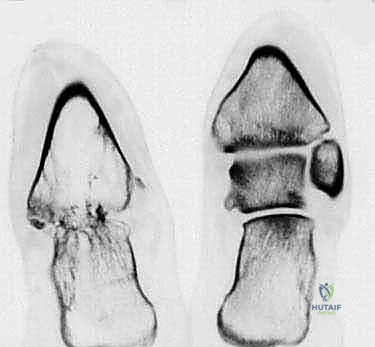
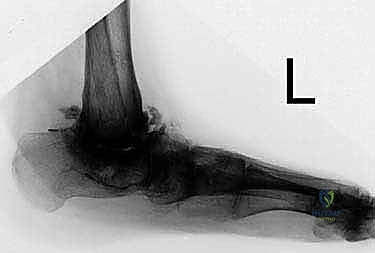
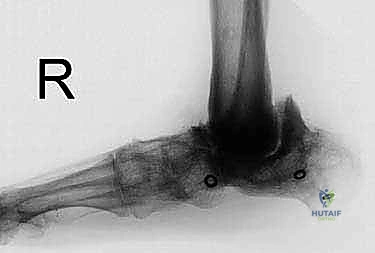
Radiographic evaluation begins with high-quality, weight-bearing (if tolerated) anteroposterior, lateral, and mortise views of the ankle and foot. These initial films provide a macroscopic overview of the structural collapse, the presence of retained hardware, and the general alignment of the mechanical axis. However, plain radiography is insufficient for assessing the true extent of osteolysis and sequestrum formation. A fine-cut Computed Tomography (CT) scan with multi-planar and 3D reconstructions is mandatory. The CT scan allows the surgeon to map the precise boundaries of viable versus necrotic bone within the tibial plafond and the calcaneus, dictating the required depth of resection during the debridement phase.
In the setting of suspected or confirmed chronic infection, identifying the causative organism is the most critical preoperative step. Empiric antibiotic therapy is strongly discouraged as it suppresses bacterial growth and yields false-negative intraoperative cultures. Patients must undergo a strict "antibiotic holiday" for a minimum of two weeks prior to any deep tissue sampling. Preoperative inflammatory markers, including the erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), and a complete blood count (CBC) with differential, are drawn to establish a baseline. If a joint effusion or fluid collection is present, fluoroscopically or ultrasound-guided aspiration is performed to obtain fluid for aerobic, anaerobic, fungal, and mycobacterial cultures. If a draining sinus tract is present, superficial swabs are notoriously unreliable; deep operative cultures are required.
Patient positioning and operating room setup must facilitate both extensive surgical exposure and unimpeded fluoroscopic imaging. The patient is positioned supine on a radiolucent operating table. A bump is placed under the ipsilateral hip to correct the natural external rotation of the lower extremity, bringing the patella and the foot into a true anteroposterior alignment. A proximal thigh tourniquet is applied to ensure a bloodless field during the critical debridement phase, though it must be deflated periodically to assess bone viability via the "paprika sign" (punctate bleeding). The entire limb is prepped and draped free from the mid-thigh distally. The C-arm fluoroscopy unit is brought in from the contralateral side, positioned to allow seamless transitions between AP, lateral, and axial views of the hindfoot without requiring the surgeon to reposition the leg awkwardly.
Step-by-Step Surgical Approach and Fixation Technique
The surgical management of an infected, necrotic talus is universally approached as a staged procedure. Stage one is dedicated entirely to the radical eradication of infection and the stabilization of the soft tissue envelope. Stage two, performed only after definitive clinical and serological clearance of the infection, focuses on skeletal reconstruction and arthrodesis.
Stage 1: Radical Débridement and Dead Space Management
The primary objective of the first stage is to convert a contaminated, necrotic wound into a clean, viable surgical bed. Following exsanguination and tourniquet inflation, the surgical approach is executed. For complete talectomy, an anteromedial approach is frequently utilized, extending from the distal tibial shaft down to the navicular, staying medial to the tibialis anterior tendon.
Deep dissection proceeds directly to the ankle joint capsule. All inflamed, hypertrophic synovium and fibrotic scar tissue are aggressively excised. Before any bone is removed, multiple deep tissue samples (at least 3 to 5 distinct specimens) are harvested using clean instruments and sent for exhaustive microbiological and histopathological analysis.
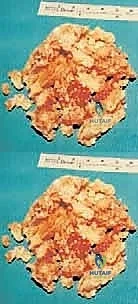
The excision of the necrotic talus must be methodical. Rather than attempting to extract the talus en bloc, which requires excessive soft tissue stripping and risks neurovascular injury, the talus is fragmented in situ. Using a combination of 1/4-inch osteotomes, heavy rongeurs, and a high-speed burr, the avascular bone is removed piecemeal.
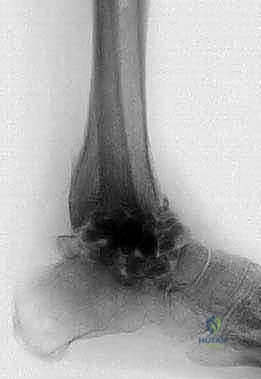
Once the macroscopic talus is removed, attention turns to the adjacent articular surfaces. The cartilage of the tibial plafond and the superior articular facets of the calcaneus are completely resected using an oscillating saw or osteotomes. The subchondral bone is sequentially debrided until healthy, bleeding cortical and cancellous bone is encountered. The tourniquet must be temporarily deflated during this step to accurately assess vascularity; bone that does not exhibit punctate bleeding is non-viable and must be excised, regardless of the resulting defect size.
Following radical debridement, the resultant massive dead space must be managed. The gold standard is the placement of an antibiotic-impregnated polymethylmethacrylate (PMMA) cement spacer. The cement is typically loaded with high doses of heat-stable, broad-spectrum antibiotics, such as Vancomycin and Tobramycin (e.g., 3-4 grams of Vancomycin and 3.6 grams of Tobramycin per 40-gram bag of cement). The cement is molded into the defect, adapting to the contours of the resected tibia and calcaneus. This spacer serves a dual purpose: it delivers massive local concentrations of antibiotics directly to the infected bed, and it acts via the Masquelet principle to induce a highly vascularized pseudosynovial membrane that will later facilitate bone grafting or fusion. The wound is then meticulously closed over a suction drain, or, if soft tissue coverage is inadequate, a negative pressure wound therapy (NPWT) device is applied.
Stage 2: Definitive Tibial-Calcaneal Arthrodesis
Stage two is undertaken only when systemic inflammatory markers (ESR, CRP) have normalized, the soft tissue envelope is completely healed, and a multidisciplinary infectious disease team has cleared the patient. This typically occurs 6 to 12 weeks after the index procedure.
The previous incision is utilized to access the joint space. The induced membrane is carefully incised, and the PMMA spacer is extracted. The membrane itself is preserved, as it is rich in osteoprogenitor cells and vascularity. The bony surfaces of the distal tibia and the superior calcaneus are freshened with a high-speed burr or osteotomes to ensure a highly biologically active bed for fusion.
At this juncture, the surgeon must address the critical issue of leg length discrepancy. The absence of the talus leaves a 3 to 4 cm void. The surgeon has two primary reconstructive options: acute shortening with direct tibial-calcaneal apposition, or the interposition of a structural bulk allograft (such as a femoral head) to maintain leg length. In the setting of previous severe infection, acute shortening is heavily favored. It eliminates the need for massive avascular allografts, which carry a high risk of reinfection and nonunion, and it dramatically reduces tension on the compromised soft tissue envelope, facilitating primary wound closure. The foot is translated posteriorly to align the mechanical axis of the tibia with the weight-bearing axis of the calcaneus, and the surfaces are intimately apposed.


Fixation is the cornerstone of the reconstructive phase. The gold standard for a direct tibial-calcaneal arthrodesis is a rigid intramedullary (IM) tibiotalocalcaneal (TTC) nail, adapted for a talus-deficient scenario. A guide wire is passed from the plantar aspect of the heel, through the calcaneus, and centrally into the tibial medullary canal. Sequential reaming is performed. The IM nail is then inserted and locked both proximally in the tibia and distally in the calcaneus. Modern nails offer internal compression mechanisms, which are critical for maximizing bone-to-bone contact and enhancing the biomechanical environment for osteogenesis.
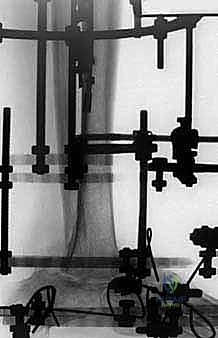

If the medullary canal is obliterated or if active infection precludes intramedullary devices, alternative fixation strategies must be employed. Rigid locking plate constructs, applied laterally or anteriorly, can provide excellent stability. In cases of extremely poor bone quality or highly tenuous soft tissues, fine-wire circular external fixation (the Ilizarov method) is an incredibly powerful tool. It allows for rigid multi-planar stabilization, the ability to dynamically compress the arthrodesis site postoperatively, and completely avoids the placement of internal hardware in a previously infected bed. Regardless of the fixation method, autologous bone graft (often harvested from the proximal tibia or iliac crest) or orthobiologics (such as Demineralized Bone Matrix or Bone Morphogenetic Proteins) are packed around the arthrodesis site to maximize the biological potential for fusion.
Complications, Incidence Rates, and Salvage Management
The complication profile for a staged tibial-calcaneal arthrodesis following infection and talar loss is substantial. Surgeons must be aggressively proactive in identifying and managing these adverse events.
| Complication | Estimated Incidence | Etiology & Pathomechanics | Salvage / Management Strategy |
|---|---|---|---|
| Nonunion / Delayed Union | 15% - 30% | Inadequate debridement, poor rigid fixation, smoking, persistent micro-motion, avascular bone ends. | Revision rigid fixation (exchange nailing or plating), aggressive autologous bone grafting (RIA from femur), application of circular external fixation, use of rhBMP-2. |
| Recurrent Deep Infection | 10% - 25% | Retained necrotic bone, biofilm persistence on hardware, inadequate systemic antibiotic duration, compromised host immunity. | Hardware removal, radical re-debridement, placement of new antibiotic spacers, prolonged IV antibiotics. If refractory, definitive below-knee amputation. |
| Symptomatic Leg Length Discrepancy | 80% - 100% (if acutely shortened) | Intentional acute shortening to close dead space and achieve direct bone apposition. | Custom shoe lifts and orthotics. If >4cm and intolerable, consideration of proximal tibial distraction osteogenesis (rarely indicated in this demographic). |
| Adjacent Joint Arthritis | 40% - 60% (long-term) | Altered hindfoot kinematics and increased mechanical stress transferred to the midfoot (naviculocuneiform, tarsometatarsal joints). | Conservative management with rocker-bottom shoes and rigid AFOs. If debilitating, extension of the fusion mass (pantalar or midfoot arthrodesis). |
| Wound Dehiscence / Flap Failure | 10% - 20% | Poor vascular supply, excessive tension on the skin during closure, smoking, uncontrolled edema. | Immediate aggressive wound care, NPWT, consultation with plastic surgery for local rotational flaps or free tissue transfer (e.g., Anterolateral Thigh flap). |
| Stress Fractures | 5% - 10% | Stress risers at the proximal end of the intramedullary nail or distal to the plate in osteopenic bone. | Prolonged immobilization, protected weight-bearing. May require revision to a longer intramedullary nail spanning the fracture. |

The most devastating complication is the recurrence of deep osteomyelitis. Despite meticulous staged protocols, bacteria can harbor in microscopic canaliculi or form persistent biofilms. If recurrence occurs after definitive fixation, the surgeon must rapidly differentiate between a superficial wound issue and deep hardware infection. Deep infections generally mandate hardware explantation, repeat radical debridement, and a return to stage one management.
Nonunion is another major hurdle, given the inherently poor biological environment. Radiographic evaluation using CT scans at 4 to 6 months postoperatively is the most accurate method to assess bridging trabecular bone. If a nonunion is identified and is aseptic, revision surgery is indicated. This typically involves optimizing the mechanical stability (e.g., revising a plate to an IM nail, or adding a plate to an existing nail construct) and radically enhancing the biology through the use of Reamer-Irrigator-Aspirator (RIA) bone graft from the femur, combined with osteoinductive agents like Bone Morphogenetic Protein-2 (rhBMP-2).
Ultimately, if the limb remains chronically painful, infected, or non-functional despite multiple reconstructive attempts, a definitive below-knee amputation is the ultimate salvage procedure. It is imperative to recognize when the physiological and psychological toll of repeated surgeries outweighs the benefit of limb preservation. A well-healed, functional BKA often provides a superior quality of life compared to a chronically infected, painful, and non-weight-bearing salvaged limb.
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation following a tibial-calcaneal arthrodesis is a marathon, not a sprint. The protocol must be strictly adhered to, as premature weight-bearing in a compromised biological environment guarantees mechanical failure and nonunion.
Phase I: Immediate Postoperative Period (Weeks 0-4)
The primary goals in this phase are wound healing, edema control, and strict protection of the arthrodesis site. The patient is placed in a well-padded, short-leg plaster or fiberglass splint in the operating room. They are strictly non-weight-bearing (NWB) on the operative extremity. Elevation of the limb above the level of the heart is mandatory for 23 hours a day to mitigate the massive swelling associated with hindfoot reconstruction. Deep vein thrombosis (DVT) prophylaxis is initiated immediately and continued for at least 4-6 weeks, given the prolonged immobility. Sutures are typically removed between 3 to 4 weeks, only after unequivocal evidence of primary wound healing.
**Phase II
