Surgeons' Guide: Unlock TKA Accuracy with a Navigation System Screenshot

Key Takeaway
For anyone wondering about Surgeons' Guide: Unlock TKA Accuracy with a Navigation System Screenshot, Computer-assisted total knee arthroplasty (CA-TKA) improves implant positioning and limb alignment using real-time computer navigation. This technology offers dynamic intraoperative feedback on bone cuts and soft tissue balancing, leading to better long-term results and fewer complications. A **navigation system screenshot** visually aids surgeons in making precise adjustments, enhancing implant longevity and reducing the need for revision surgery.
Comprehensive Introduction and Patho-Epidemiology
Computer-assisted total knee arthroplasty (CA-TKA) represents a paradigm shift in orthopedic surgery, utilizing advanced spatial tracking technology to provide surgeons with real-time, dynamic intraoperative feedback. The fundamental goal of total knee arthroplasty (TKA) is the alleviation of pain and the restoration of function through the precise reconstruction of joint biomechanics. Accurate component positioning and the restoration of a neutral mechanical axis are universally recognized as the most critical determinants of long-term implant survivorship. Historically, conventional manual instrumentation has relied on extramedullary and intramedullary alignment guides, which are subject to inherent inaccuracies due to variations in patient anatomy, intramedullary bowing, and surgeon visual estimation. It has been extensively documented in orthopedic literature that alignment errors as small as 3 degrees from the neutral mechanical axis significantly alter load distribution across the polyethylene bearing surface, exponentially increasing the risk of accelerated wear, osteolysis, and aseptic loosening.
The patho-epidemiology of knee osteoarthritis reveals a shifting demographic landscape that further necessitates the precision offered by CA-TKA. As the global population ages and the prevalence of obesity rises, the volume of primary TKA procedures is projected to grow exponentially. Furthermore, the indications for TKA have expanded to include younger, highly active patients who place greater biomechanical demands on their prostheses. In this younger cohort, the expectation of a perfectly functioning, forgotten joint places an immense burden on the surgeon to eliminate mechanical outliers. Conventional instrumentation typically yields a mechanical axis outlier rate (defined as >3 degrees of deviation) of 20% to 30%. In stark contrast, navigation systems have consistently demonstrated the ability to reduce this outlier rate to less than 5%, effectively standardizing the surgical outcome regardless of the underlying anatomic complexity.
The evolution of navigation systems has transitioned from cumbersome, early-generation image-based systems (requiring preoperative CT or MRI) to sophisticated imageless (kinematic) systems. Modern imageless navigation systems utilize infrared cameras and light-emitting diodes (LEDs) or passive reflective spheres attached to rigid bodies fixed to the patient’s femur and tibia. This technology functions to map the patient’s unique intraoperative anatomy, creating a personalized, three-dimensional virtual model of the knee. By providing dynamic intraoperative feedback regarding the orientation of bone cuts, soft tissue balancing, component positioning, limb alignment, and knee range of motion with the trial components in place, the surgeon is empowered to make micro-adjustments before any irreversible bone resection occurs. Ultimately, the navigation system acts as a highly advanced informational tool; it does not replace the surgeon's clinical judgment, but rather augments it, ensuring that the execution of the surgical plan is flawlessly translated to the patient's anatomy.

Detailed Surgical Anatomy and Biomechanics
The success of a navigated TKA is entirely dependent on the surgeon's intimate understanding of knee anatomy across the coronal, sagittal, and horizontal (axial) planes, as the computer software relies on the accurate manual digitization of these anatomic landmarks. In the coronal plane, the surgical principle for proper alignment is to restore the mechanical axis to neutral by placing the femoral and tibial components orthogonal to the mechanical axis of the limb. The mechanical axis of the lower extremity is defined precisely as a line connecting the center of the femoral head to the center of the ankle joint (the center of the talar dome). The anatomic axis of the femur, conversely, is described as the intersection of lines drawn parallel to the long axis of the femoral diaphysis, typically creating a valgus angle of 5 to 7 degrees relative to the mechanical axis. In standard intramedullary techniques, the anatomic axis is utilized as a surrogate guide to estimate the mechanical axis, introducing potential error in patients with excessive femoral bowing. In navigation-assisted techniques, the center of the femoral head is calculated kinematically through circumduction of the hip, allowing the software to determine the true mechanical axis independently of diaphyseal deformities.
When evaluating the sagittal plane, kinematic considerations are paramount because the vast majority of the knee's range of motion occurs within this arc. The degree of posterior slope of the proximal tibia is the primary indicator of proper sagittal alignment and is critical for maintaining flexion gap kinematics, optimizing patellofemoral tracking, and preventing anterior impingement. The mechanical axis of the tibia in the sagittal plane can be determined using multiple reference points. One widely accepted method connects the midpoint of the tibial plateau to the midpoint of the talus. An alternative method connects the midpoints of the medial tibial plateau and the tibial plafond. Navigation systems allow the surgeon to digitize the anterior cortex of the tibia to establish a reference line, ensuring that the planned tibial resection matches the patient's native posterior slope, which typically ranges from 3 to 7 degrees depending on the specific implant design philosophy (cruciate-retaining versus posterior-stabilized).
Rotational alignment of the implanted components is arguably the most challenging aspect of TKA and is of the utmost importance for successful outcomes. Malrotation of the femoral or tibial components is a primary driver of poor patellar tracking, anterior knee pain, stiffness, and early failure. The reference axis for femoral rotational alignment remains a topic of academic debate, with the surgical epicondylar axis (SEA), the anteroposterior axis (Whiteside’s line), and the posterior condylar axis (PCA) all serving as potential references. Each of these axes possesses inherent flaws; for instance, the PCA is unreliable in the setting of severe posterior condylar hypoplasia or valgus wear. In CA-TKA, the reference for femoral rotation is often a calculated average rotational axis derived from the digitized transepicondylar and Whiteside lines, cross-referenced against the posterior condyles. For the rotational axis of the tibia, the medial third of the tibial tuberosity, as advocated by Insall, remains the gold standard. Navigation systems require the precise digitization of these landmarks to establish a reliable rotational profile, highlighting that the output of the computer is only as accurate as the input provided by the surgeon.

Exhaustive Indications and Contraindications
The application of computer navigation in total knee arthroplasty is broadly applicable to primary, complex primary, and revision scenarios. However, specific clinical scenarios exist where CA-TKA is not merely an optional adjunct, but rather the standard of care required to achieve an acceptable outcome. The primary indication for utilizing a navigation system is the presence of extra-articular deformity. Patients with malunions of the femoral or tibial diaphysis secondary to previous trauma present a unique challenge, as standard intramedullary rods cannot be passed, or if passed, will result in an erroneous mechanical axis. Navigation bypasses the diaphysis entirely by referencing the center of the hip and ankle, allowing for perfectly orthogonal intra-articular resections despite profound extra-articular bowing. Similarly, patients with retained hardware (such as long intramedullary nails or plates from prior fracture fixation) that obstruct the medullary canal are ideal candidates for imageless navigation.
Another compelling indication for CA-TKA is severe obesity. In morbidly obese patients, identifying external anatomic landmarks and accurately judging the overall limb alignment visually or with standard extramedullary guides is notoriously difficult. The thick adipose tissue obscures the center of the ankle and the anterior superior iliac spine, leading to a high rate of malalignment in manual TKA. By securely fixing rigid tracker bodies to the bone and utilizing kinematic registration, the navigation system removes the soft tissue envelope as a confounding variable. Furthermore, young, high-demand patients who require maximal implant longevity benefit significantly from the precision of navigation, as minimizing micromotion and polyethylene wear through perfect alignment is critical for avoiding early revision in this demographic.
Despite its vast utility, CA-TKA is not without contraindications. Absolute contraindications are relatively rare but include active local or systemic infection, which precludes any elective arthroplasty. Relative contraindications revolve primarily around the ability to safely place and utilize the tracking pins. Severe osteoporosis or metabolic bone disease poses a significant risk for pin-tract fractures or tracker loosening during the procedure. If the rigid bodies shift even a millimeter during the surgery, the entire coordinate system is compromised, leading to disastrous bone cuts if unrecognized. Additionally, a severely stiff knee or a knee with profound flexion contracture that cannot be mobilized may prevent the kinematic registration of the hip center, as the surgeon must be able to circumduct the hip and flex the knee to allow the software to calculate the joint centers.
Indications and Contraindications Summary Table
| Category | Specific Clinical Condition | Rationale / Surgical Consideration |
|---|---|---|
| Strong Indications | Extra-articular Deformity (Malunion) | Bypasses the deformed diaphysis; calculates true mechanical axis kinematically. |
| Strong Indications | Retained Hardware (IM Nails, Plates) | Eliminates the need for intramedullary canal violation and rod placement. |
| Strong Indications | Morbid Obesity (BMI > 40) | Soft tissue envelope obscures visual landmarks; navigation relies on fixed bone trackers. |
| Relative Indications | Young, High-Demand Patients | Maximizes implant survivorship by ensuring <3 degree mechanical axis deviation. |
| Relative Contraindications | Severe Osteopenia / Osteoporosis | High risk of tracker pin-site fracture or intraoperative tracker loosening/migration. |
| Relative Contraindications | Severe Arthrofibrosis / Ankylosis | Inability to perform kinematic circumduction required for hip center registration. |
| Absolute Contraindications | Active Joint Infection | Standard contraindication for any elective total joint arthroplasty. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the cornerstone of any successful surgical intervention. The most critical initial step is the clinical determination that the patient has exhausted all conservative management options and definitively requires a TKA. Preoperative radiographic evaluation must include a standing anteroposterior (AP) view, a true lateral view, and a skyline (Merchant) view of the patella. While a long-leg standing AP radiograph (hip-to-ankle) is the gold standard for assessing the overall mechanical axis and planning manual TKA, it is often considered unnecessary when utilizing a kinematic navigation system. Because the navigation system accurately determines the mechanical axis of the limb intraoperatively—even in the presence of severe previous deformity secondary to trauma—the reliance on full-length preoperative imaging is reduced. However, obtaining long-leg films remains an excellent academic practice to anticipate the degree of correction required and to identify any subtle extra-articular bowing.
In standard manual techniques, preoperative templating on digital radiographs is utilized to anticipate approximate component sizing, offset, and the presence of bone defects that necessitate augments or stems. In the navigation-assisted technique, while preoperative digital templating is still performed to ensure appropriate inventory is available, the true "templating" occurs intraoperatively. Intraoperative templating is achieved through the meticulous digitization of different anatomic areas. By mapping the articular surface, the software calculates the exact dimensions of the distal femur and proximal tibia, recommending component sizes that optimize cortical coverage while avoiding overhang. Furthermore, the preoperative range of motion and soft tissue laxity are assessed dynamically by the navigation system before any incisions are made to the capsule, providing a highly accurate baseline that helps the surgeon plan the sequence of releases and the target for the final balanced gaps.
Patient positioning, anesthesia, venous thromboembolism prophylaxis, and medical clearance protocols mirror those of standard TKA techniques. The patient is placed supine on the operating table. A tourniquet is applied snugly to the upper thigh as far proximally as practical. In very obese patients, adipose tissue may be pulled distally from beneath the tourniquet, causing it to bulge from the distal edge; careful application prevents migration and ensures the tourniquet remains proximal to the surgical field. A transverse bar or a specialized foot-holder is placed on the table at a level just distal to the joint line. When the knee is fully flexed, the foot engages the bar, maintaining the flexed position without requiring continuous manual support from an assistant.
Crucially, the physical setup of the operating room must be optimized for the navigation equipment. The optical camera (the "eye" of the navigation system) must be positioned opposite the surgeon, typically on the contralateral side of the patient, to ensure an uninterrupted line of sight. Before starting patient registration, the camera must be brought perfectly in line with the knee joint so that all tracker arrays and pointing tools can communicate seamlessly. All trackers must be initialized, and the pointer tip calibrated to sub-millimeter accuracy before the skin incision is made.

FIG 1: The navigation system optical camera should be placed opposite the surgeon to ensure continuous instrument visibility and uninterrupted line of sight during real-time tracking.
Step-by-Step Surgical Approach and Fixation Technique
Incision, Exposure, and Tracker Placement
All standard and minimally invasive approaches for the exposure of the knee joint can be applied and supported with the navigation system. The most commonly utilized skin incision for primary TKA is an anterior midline incision, followed by a standard median parapatellar arthrotomy. The incision is ideally made with the knee in deep flexion to allow the subcutaneous tissue to fall sideways, naturally aiding in exposure. The skin incision must be of adequate length to avoid excessive tension during retraction, which can lead to marginal skin necrosis and devastating postoperative wound complications. Once the joint is exposed, the immediate next step—unique to CA-TKA—is the rigid fixation of the tracker arrays to the femur and tibia. Two bicortical pins are typically placed in the distal femoral diaphysis, outside the joint capsule, and two in the proximal tibial diaphysis. It is imperative that these pins are placed securely to prevent any micro-motion, yet carefully positioned to avoid creating stress risers in the diaphyseal bone.
Kinematic Registration and Landmark Digitization
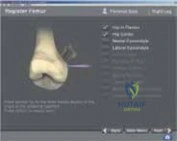
Following tracker placement, the critical phase of registration begins. The software must build a virtual coordinate system of the patient's leg. The center of the femoral head is determined kinematically; the surgeon moves the hip through a series of circumduction maneuvers while the camera tracks the femoral array, allowing the software to mathematically calculate the exact center of rotation. Next, the surgeon utilizes the calibrated pointer to digitize specific anatomic landmarks: the medial and lateral malleoli to determine the ankle center, the medial and lateral epicondyles to establish the surgical epicondylar axis, Whiteside’s line, the center of the knee, and the tibial anteroposterior axis. The accuracy of this digitization cannot be overstated. If a mistake in digitization occurs, the calculated axes will be flawed. The software often includes internal validation checks; if a digitized point falls outside of expected anatomic norms, the system will halt progression, prompting the surgeon to re-register the landmark.
Dynamic Gap Assessment and Bone Resection
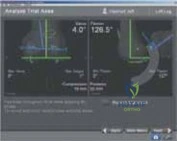
Once registration is complete, the navigation system provides a real-time display of the limb's mechanical alignment, flexion/extension contractures, and varus/valgus deformity. The surgeon then takes the knee through a full range of motion while applying varus and valgus stress to map the soft tissue envelope. This allows for the precise calculation of the native joint gaps before any bone is resected. Utilizing the navigated cutting blocks, the surgeon adjusts the distal femoral and proximal tibial resections. The cutting blocks are tracked in real-time, allowing the surgeon to dial in the exact depth of resection (e.g., 9mm from the prominent condyle) and the exact coronal and sagittal alignment (e.g., 0 degrees of varus/valgus, 3 degrees of posterior slope) down to half-degree and half-millimeter increments. After the blocks are pinned, a verification tool is often used to confirm the block hasn't shifted before the saw is applied.
Trialing and Final Implant Fixation
After the bone cuts are executed and any necessary soft tissue releases are performed, trial components are inserted. This is where the dynamic intraoperative feedback of the navigation system truly shines. With the trials in place, the knee is again taken through a full range of motion. The screen displays the final mechanical axis, the stability of the flexion and extension gaps, and the patellofemoral tracking kinematics. If the gaps are asymmetric or the mechanical axis deviates from neutral, the surgeon has the objective data required to make targeted adjustments—such as a 1mm recut or a specific ligamentous release—prior to opening the final implants. Once perfect kinematic and static alignment is confirmed on the monitor, the final components are cemented into place. The navigation system can be used one final time after cement polymerization to document the ultimate reconstructed mechanical axis for the operative record.

Complications, Incidence Rates, and Salvage Management
While computer-assisted TKA drastically reduces the rate of mechanical malalignment, it introduces a unique set of technology-specific complications that the orthopedic surgeon must be prepared to manage. The most concerning complication directly attributable to the navigation system is the occurrence of pin-tract fractures. The insertion of 4mm or 5mm bicortical threaded pins into the diaphyseal bone of the femur and tibia creates a localized stress riser. In osteoporotic bone, or if the pins are placed too close together or multiple passes are made, the torsional forces of weight-bearing can lead to a postoperative diaphyseal fracture. The incidence of pin-tract fractures is reported in the literature to be between 0.1% and 0.5%. Management typically requires formal open reduction and internal fixation (ORIF) with a locking plate, or in severe cases, revision to a long-stemmed diaphyseal-engaging prosthesis.
Another significant complication is tracker loosening or migration during the procedure. If the tracker array is bumped by a retractor or the surgeon's body, or if the bone is soft, the array may shift. Because the computer assumes the array is rigidly fixed to the bone, any movement alters the entire coordinate system. If the surgeon fails to recognize this shift and proceeds with the bone cuts based on the corrupted data, catastrophic malalignment will occur. The incidence of recognized tracker loosening is approximately 1% to 2%. The salvage management for this complication is immediate re-registration of the entire limb. Surgeons must remain vigilant and utilize the software's internal verification tools frequently throughout the case to confirm tracker stability.
Furthermore, line-of-sight interruptions and software glitches can significantly increase the operative time. The infrared camera requires a completely unobstructed view of the tracker spheres. Surgical personnel, overhead lights, or passing instruments can block this view, freezing the system. While not a direct physiological complication, increased operative time (typically 10 to 15 minutes longer than manual TKA) is associated with a theoretically higher risk of infection and tourniquet-related ischemia. Pin-site infections are another rare but documented complication, occurring in less than 0.5% of cases. These are typically superficial and respond well to oral antibiotics, but deep infections communicating with the joint space require aggressive surgical debridement.
Complications and Management Table
| Complication Type | Estimated Incidence | Etiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Pin-Tract Fracture | 0.1% - 0.5% | Stress risers from tracker pins; Osteoporosis; Multiple drill passes. | ORIF with locking plates; Revision to long-stemmed implants. |
| Tracker Migration | 1.0% - 2.0% | Poor pin purchase; Iatrogenic bumping of the array during exposure. | Immediate halt of procedure; Complete re-registration of all landmarks. |
| Pin-Site Infection | < 0.5% | Thermal necrosis during drilling; Inadequate skin closure over pin sites. | Local wound care; Oral antibiotics; Rarely requires deep I&D. |
| Registration Error | Variable | Inaccurate manual digitization of landmarks (e.g., epicondyles). | Software validation warnings; Re-digitization of specific anatomic points. |
| Increased OR Time | Universal (+10-15 mins) | Line-of-sight blockages; Software calibration; Learning curve. | Meticulous OR setup; Team training; Efficient instrument passing. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation following a computer-navigated TKA generally follows the same rigorous, phased protocols as conventional TKA. However, anecdotally and in some emerging literature, patients undergoing perfectly balanced, navigated TKAs may experience slightly less early postoperative inflammatory pain due to the minimization of soft tissue trauma and the avoidance of over-tensioned ligaments. The ultimate goal of the rehabilitation protocol is the rapid restoration of functional mobility, the prevention of thromboembolic events, and the return to independent activities of daily living.
Phase 1: Acute Recovery and Early Mobility (Weeks 0-2)
The immediate postoperative phase focuses on pain control, edema management, and the prevention of deep vein thrombosis (DVT). Venous thromboembolism prophylaxis is initiated per institutional guidelines, typically utilizing aspirin, low-molecular-weight heparin, or direct oral anticoagulants. Physical therapy begins on postoperative day zero. The primary objectives in this phase are achieving full active and passive extension (0 degrees) to prevent flexion contractures, and initiating early flexion (aiming for 90 degrees by the end of week two). Weight-bearing as tolerated (WBAT) with an assistive device (walker or crutches) is encouraged immediately. The patient is instructed on isometric quadriceps sets, straight leg raises, and ankle pumps.
Phase 2: Strength and Gait Normalization (Weeks 2-6)
As the acute surgical pain and swelling subside, the focus shifts to progressive resistance training and the weaning of assistive devices. The goal is to achieve a functional range of motion, typically 0 to 110 degrees or greater. Closed kinetic chain exercises, such as mini-squats, leg presses, and stationary cycling, are introduced to rebuild quadriceps and hamstring strength without placing excessive shear stress on the healing arthrotomy. Gait training becomes paramount; the physical therapist works closely with the patient to eliminate compensatory movement patterns, such as a Trendelenburg gait or a stiff-knee gait, ensuring the patient utilizes the perfectly aligned mechanical axis achieved during surgery.
Phase 3: Advanced Function and Return to Activity (Weeks 6-12+)
The final phase of rehabilitation transitions the patient from basic mobility to higher-level functional activities. Proprioceptive and balance training are incorporated, utilizing unstable surfaces like foam pads or BOSU balls. Advanced strengthening continues, with a focus on endurance and power. Patients are typically cleared to return to low-impact recreational activities, such as swimming, golf, and doubles tennis, between 8 and 12 weeks postoperatively. The surgeon must emphasize to the patient that while the navigation system has provided a mechanically optimal construct, the ultimate success and "feel" of the joint rely heavily on the patient's dedication to this final phase of neuromuscular rehabilitation.

Summary of Landmark Literature and Clinical Guidelines
The integration of computer navigation into orthopedic surgery has been accompanied by a robust body of scientific literature evaluating its efficacy, safety, and long-term impact on survivorship. The consensus among landmark studies is unequivocally clear regarding radiographic outcomes: CA-TKA significantly improves the accuracy of component positioning and limb alignment compared to conventional manual techniques. A seminal meta-analysis by Mason et al. demonstrated that navigation reduces the risk of mechanical axis malalignment (>3 degrees of deviation) by over 80%. This reduction in outliers is the primary metric by which the success of navigation is judged, as it standardizes the surgical outcome across varying levels of surgeon experience and patient complexity.
Clinical outcome scores, however, have historically been a subject of intense debate. Early short-term studies often failed to show a statistically significant difference in Knee Society Scores (KSS) or Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) scores between navigated and conventional cohorts at one or two years postoperatively. This led to skepticism regarding the cost-benefit ratio of the expensive technology. However, as longitudinal data has matured, the clinical benefits have become more apparent. Studies by Choong et al. correlated accurate mechanical alignment achieved via navigation with significantly improved functional outcomes and quality of life metrics at intermediate follow-up.
Furthermore, large national joint registry data (such as the Australian Orthopaedic Association National Joint Replacement Registry) has begun to demonstrate a divergence in survivorship curves favoring computer-navigated TKA in specific demographics, particularly in younger patients (<65 years old). In this high-demand cohort, the incidence of revision for aseptic loosening is significantly lower in the navigated group at 10 and 15 years. Current clinical guidelines from major orthopedic societies acknowledge that while conventional TKA remains a highly successful procedure, computer-assisted navigation is a validated, highly effective tool for optimizing alignment, particularly in cases involving complex extra-articular deformity, retained hardware, or morbid obesity. As technology continues to evolve toward robotics and augmented reality, the foundational principles of kinematic registration and real-time intraoperative feedback established by CA-TKA will remain the bedrock of precision arthroplasty.
Clinical & Radiographic Imaging Archive