Tibiotalocalcaneal Arthrodesis: Lateral Blade Plate Technique Masterclass

Key Takeaway
This masterclass guides fellows through tibiotalocalcaneal arthrodesis using a lateral blade plate. We'll meticulously cover comprehensive anatomy, preoperative planning, and granular, real-time intraoperative execution. Learn precise dissection, joint preparation, blade plate insertion, and screw fixation, emphasizing critical pearls and pitfalls. Postoperative care and complication management are also detailed for optimal patient outcomes.
Comprehensive Introduction and Patho-Epidemiology
Tibiotalocalcaneal (TTC) arthrodesis is a formidable, salvage-level reconstructive procedure designed to address end-stage, debilitating pathology involving both the tibiotalar (ankle) and talocalcaneal (subtalar) joints. This complex intervention is typically reserved for patients who have exhausted all non-operative modalities and present with profound pain, severe deformity, and functional incapacitation. The underlying etiologies necessitating a TTC fusion are broad but generally converge on the catastrophic loss of articular cartilage and structural integrity of the hindfoot. Common precursors include severe post-traumatic osteoarthritis following pilon or talus fractures, advanced avascular necrosis (AVN) of the talar body, severe rheumatoid arthritis, and the devastating structural collapse associated with Charcot neuroarthropathy.
The pathophysiology of pan-hindfoot arthritis is characterized by a progressive, relentless cascade of joint destruction. Once the articular congruity of either the ankle or subtalar joint is compromised, altered biomechanical forces inevitably accelerate wear in the adjacent articulations. For instance, an isolated ankle fusion alters the kinematics of the hindfoot, frequently leading to accelerated subtalar arthrosis. Conversely, primary talar AVN can lead to the collapse of the talar dome, simultaneously destroying both the tibial plafond articulation and the subtalar facets. As the cartilage degrades, patients develop significant malalignment—often a severe varus or valgus thrust—which further exacerbates the abnormal load distribution, creating a vicious cycle of pain, instability, and progressive deformity that renders normal ambulation impossible.
Nonoperative management strategies, while initially useful, ultimately fail to alter the natural history of this progressive disease. Modalities such as rigid ankle-foot orthoses (AFOs), patellar tendon-bearing braces, or custom Charcot Restraint Orthotic Walkers (CROW) can provide temporary symptomatic relief by limiting joint excursion and offloading the affected areas. However, these devices are cumbersome, often lead to skin breakdown in dysvascular patients, and cannot correct fixed bony deformities. When a patient's deformity becomes unbraceable, or when the pain becomes refractory to maximal conservative therapy, surgical intervention transitions from an elective consideration to an absolute necessity to prevent further functional decline and potential limb loss.
The primary surgical objective of a TTC arthrodesis is the creation of a stable, plantigrade, and pain-free foot that is optimally aligned for the biomechanics of ambulation. Achieving this requires meticulous joint preparation, robust deformity correction, and rigid internal fixation. The lateral blade plate technique, which we will detail in this masterclass, represents a highly effective, time-tested method for achieving these goals. By utilizing a fixed-angle device applied to the lateral aspect of the hindfoot, the surgeon can provide exceptional biomechanical stability, compress the arthrodesis sites effectively, and resist the powerful deforming forces of the lower extremity musculature, thereby maximizing the probability of a successful, durable osseous union.
Detailed Surgical Anatomy and Biomechanics
A profound, three-dimensional understanding of hindfoot anatomy and biomechanics is the cornerstone of a successful TTC arthrodesis. The osteology of this region is uniquely complex. The tibiotalar joint is a highly congruent mortise, relying on the precise fit of the trapezoidal talar body within the distal tibia and fibula. The subtalar joint, with its anterior, middle, and posterior facets, dictates the complex inversion and eversion mechanics of the hindfoot. The talus itself is an anatomical anomaly; it is entirely devoid of muscular or tendinous insertions, and approximately 70% of its surface area is covered by articular cartilage. This leaves a severely limited footprint for vascular ingress, making the talus notoriously vulnerable to ischemic insults.
The vascular anatomy of the talus demands specific respect during any hindfoot reconstruction. The primary blood supply to the talar body is retrograde, entering through the talar neck via the artery of the tarsal canal (a branch of the posterior tibial artery) and the artery of the sinus tarsi. When a patient presents with post-traumatic arthritis following a displaced talar neck fracture, this tenuous blood supply has often been disrupted, leading to avascular necrosis of the body. In these scenarios, the talus becomes a necrotic, sclerotic spacer rather than a biologically active participant in the fusion process. Recognizing this compromised vascularity is critical, as it dictates the necessity for aggressive debridement of dead bone, the liberal use of osteoinductive bone grafts, and the requirement for exceptionally rigid fixation to bridge the mechanically inferior talar segment.
Navigating the lateral hindfoot requires meticulous identification and protection of critical neurovascular structures. The superficial peroneal nerve (SPN) is the primary structure at risk during the proximal extent of the extensile lateral approach. The SPN typically pierces the crural fascia approximately 10 to 12 centimeters proximal to the distal tip of the lateral malleolus. It then courses anteriorly and distally over the extensor retinaculum. Iatrogenic injury to the SPN can result in painful neuromas and debilitating numbness over the dorsum of the foot. Distally, the sural nerve is encountered. Formed by contributions from the tibial and common peroneal nerves, it courses posterior and lateral to the Achilles tendon, typically lying about 1 centimeter distal to the tip of the fibula before continuing along the lateral border of the foot. Retraction in this area must be gentle to avoid traction neurapraxia.
Biomechanically, the lateral blade plate functions as a remarkably powerful fixed-angle construct. When applied to the lateral aspect of the tibia, talus, and calcaneus, it acts as a tension band against the typical varus deforming forces exerted by the patient's weight and the pull of the posterior tibial tendon. Unlike intramedullary nails, which rely on the relatively poor bone stock of the calcaneal tuberosity for distal purchase, the blade plate engages the dense, trabecular bone of the calcaneal body directly beneath the posterior facet. Furthermore, the lateral application allows for the direct visualization of the fusion sites during compression. By utilizing an articulated tension device on the tibial shaft, massive compressive forces can be generated across both the subtalar and tibiotalar joints simultaneously, maximizing the bone-on-bone contact essential for primary osseous healing.
Exhaustive Indications and Contraindications
The decision to proceed with a TTC arthrodesis using a lateral blade plate must be predicated on a rigorous evaluation of the patient's pathology, overall medical health, and functional demands. The ideal candidate is a patient with severe, symptomatic arthritis of both the ankle and subtalar joints who has failed exhaustive conservative management. Post-traumatic arthritis remains the most common indication, particularly following high-energy pilon fractures or severe talus fractures that have resulted in secondary AVN and structural collapse. Charcot neuroarthropathy, particularly when involving the hindfoot and ankle with impending or actual skin compromise, is another critical indication where the robust fixation of a blade plate can salvage a limb destined for amputation.
Patient optimization prior to surgical intervention cannot be overstated. Orthopedic surgeons must act as vigilant perioperative physicians. Smoking cessation is an absolute, non-negotiable prerequisite in my practice. The literature unequivocally demonstrates that nicotine induces profound peripheral vasoconstriction and inhibits osteogenesis, leading to a staggering 14-fold increase in nonunion rates in hindfoot fusions. I require a minimum of six weeks of documented smoking cessation, often verified by serum cotinine levels, prior to scheduling. Furthermore, diabetic patients must have their glycemic control strictly optimized, ideally aiming for a Hemoglobin A1c of less than 7.5%, to mitigate the exponentially higher risks of deep surgical site infections and impaired wound healing.
Patients suffering from systemic inflammatory arthropathies, such as rheumatoid arthritis, require careful coordination with their rheumatologist. Disease-modifying antirheumatic drugs (DMARDs) and biologic agents, while excellent for controlling systemic disease, profoundly suppress the immune system and impair the inflammatory phase of bone healing. These medications must be strategically held perioperatively, typically for at least two weeks before and after surgery, depending on the specific half-life of the agent. Additionally, any clinical suspicion of active infection—whether from a previous surgical site or an overlying chronic ulceration in a Charcot patient—mandates a comprehensive infectious disease workup, including inflammatory markers (ESR, CRP), advanced imaging (MRI or tagged white blood cell scans), and potentially a preoperative image-guided bone biopsy.
Indications and Contraindications Matrix
| Category | Absolute | Relative |
|---|---|---|
| Indications | Refractory pain from pan-hindfoot arthritis | Failed isolated ankle arthrodesis with subtalar progression |
| Unbraceable severe hindfoot deformity | Rheumatoid arthritis with severe hindfoot collapse | |
| Charcot neuroarthropathy with impending ulceration | Avascular necrosis of the talus with joint collapse | |
| Paralytic deformities (e.g., severe polio, drop foot) | Chronic, unbraceable instability of the hindfoot | |
| Contraindications | Active, untreated deep infection (osteomyelitis) | Active tobacco use (requires cessation) |
| Severe peripheral arterial disease (inadequate perfusion) | Poorly controlled Diabetes Mellitus (HbA1c > 8.0%) | |
| Medically unstable for prolonged anesthesia | Severe osteopenia/osteoporosis (compromises fixation) | |
| Lack of soft tissue coverage (requires flap first) | Patient non-compliance with non-weight-bearing protocols |
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the blueprint for a successful surgical execution. The evaluation begins with standard, weight-bearing plain radiographs, including anteroposterior (AP), lateral, and mortise views of the ankle, as well as AP, lateral, and oblique views of the foot. These initial images allow us to assess the global alignment of the hindfoot, the degree of joint space narrowing, and the presence of osteophytes or subchondral cysts. On the lateral view, we specifically analyze the talocalcaneal angle and the talo-first metatarsal angle (Meary's angle) to quantify the extent of the deformity.


Advanced imaging is practically mandatory for a complex TTC arthrodesis. A fine-cut Computed Tomography (CT) scan with multi-planar reconstructions provides an invaluable, three-dimensional assessment of the bony architecture. The CT scan allows us to precisely map out areas of avascular necrosis, quantify the volume of bone loss (which dictates our bone grafting strategy), and evaluate the structural integrity of the calcaneus, which must accept the blade of our plate. If there is any clinical ambiguity regarding active infection or the viability of the surrounding soft tissue envelope, a Magnetic Resonance Imaging (MRI) scan with intravenous contrast is indicated.
Templating is a critical step that should never be bypassed. Using digital or acetate templates overlaying the lateral radiograph, we determine the optimal trajectory for the blade into the calcaneus and select the appropriate plate size. The standard implant is a 95-degree condylar blade plate. The blade length is typically 40mm to ensure adequate purchase in the dense bone of the calcaneal body without breaching the medial cortex, which risks injury to the posterior tibial neurovascular bundle. The side plate length is chosen based on the necessary proximal tibial fixation; typically, a 5 to 8-hole plate is required to achieve at least six cortices of robust fixation proximal to the tibiotalar joint.
In the operating theater, the patient is positioned supine on a radiolucent table. A generous bump is placed beneath the ipsilateral buttock to internally rotate the lower extremity, bringing the lateral aspect of the ankle into a directly superior, highly accessible orientation. A well-padded pneumatic tourniquet is applied to the proximal thigh to ensure a bloodless surgical field, which is vital for identifying neurovascular structures and assessing the adequacy of cartilage debridement. The fluoroscopy unit (C-arm) is positioned on the contralateral side of the table. It must be draped and maneuvered prior to prepping to ensure that perfect AP, lateral, and mortise views of the ankle and hindfoot can be obtained effortlessly without having to physically reposition the patient's leg during the critical phases of alignment and hardware insertion.
Step-by-Step Surgical Approach and Fixation Technique
The Extensile Lateral Approach and Fibular Osteotomy
The procedure commences with an extensile, curvilinear lateral incision, often referred to as a modified Kocher approach. The incision spans approximately 15 to 20 centimeters, beginning proximally over the mid-shaft of the fibula, extending distally along the posterior margin of the fibula, and then curving gently anteriorly towards the base of the fourth metatarsal.

As the incision is deepened through the subcutaneous tissues, paramount attention is directed toward identifying and protecting the superficial peroneal nerve proximally and the sural nerve distally. The deep fascia is incised in line with the skin incision. To expose the subtalar joint, the origin of the extensor digitorum brevis (EDB) muscle is meticulously elevated from the lateral calcaneus and reflected anteriorly.
A critical component of this exposure is the management of the distal fibula. The fibula acts as a lateral strut; leaving it in place severely impedes access to the tibiotalar and subtalar joints and prevents the correction of severe valgus deformities. Therefore, a fibular osteotomy is performed using an oscillating saw approximately 6 to 10 centimeters proximal to the tip of the lateral malleolus. The distal fibular segment is carefully dissected free from its ligamentous attachments and excised.

This resected fibula is not discarded; it is a premium source of autogenous, cortico-cancellous bone graft. On the back table, the fibula is stripped of soft tissue and morselized using a bone mill or a small acetabular reamer, creating a rich osteoinductive and osteoconductive slurry that will later be packed into the fusion sites.
Meticulous Joint Preparation
With the fibula removed and the peroneal tendons safely retracted posteriorly, the surgeon has panoramic access to the lateral aspect of the ankle and hindfoot. The joint capsules of both the tibiotalar and subtalar joints are sharply incised. A lamina spreader or a dedicated joint distractor is inserted to pry the joint spaces open. The absolute key to a successful arthrodesis is the complete, uncompromising eradication of all articular cartilage down to bleeding subchondral bone.


Using a combination of sharp curettes, flexible osteotomes, and a high-speed burr, the cartilage is systematically stripped from the tibial plafond, the talar dome, and the anterior, middle, and posterior facets of the subtalar joint. When utilizing a burr, copious, continuous cold saline irrigation is mandatory to prevent thermal necrosis of the underlying bone, which would create a zone of dead tissue that severely impedes osseous bridging. Once the subchondral plate is exposed, it is "feathered" or fish-scaled with an osteotome, and multiple small drill holes (2.0mm) are made approximately 3 millimeters apart to penetrate the subchondral bone, allowing marrow elements and osteoprogenitor cells to migrate into the fusion bed.
Deformity Correction and Blade Plate Insertion
Once the joints are prepared, the foot is manipulated into the optimal position for fusion: neutral dorsiflexion (0 degrees), approximately 5 degrees of hindfoot valgus, and 5 to 10 degrees of external rotation to match the contralateral limb. Achieving this plantigrade position is non-negotiable. Provisional fixation is achieved using multiple stout Steinmann pins driven across the subtalar and tibiotalar joints. Fluoroscopy is utilized to confirm perfect alignment in all planes.


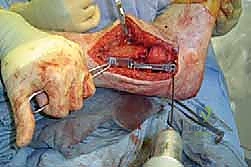
Attention then turns to the lateral blade plate. The entry point for the seating chisel is identified on the lateral aspect of the calcaneus, typically 1 to 2 centimeters inferior to the posterior facet. The seating chisel is driven across the calcaneus, parallel to the plantar aspect of the foot and perpendicular to the lateral wall of the calcaneus, ensuring it does not breach the medial cortex. The chisel is removed, and the pre-selected 95-degree condylar blade plate is impacted into the prepared slot. The side plate should lie flush against the lateral aspect of the talus and the lateral tibial shaft.
Compression and Final Fixation
With the blade securely seated in the calcaneus, the true biomechanical advantage of this construct is deployed: dynamic compression. An articulated tension device is secured to the tibial shaft proximal to the plate. The device is hooked into the proximal hole of the blade plate. As the tension device is tightened, it pulls the plate—and consequently the calcaneus and talus—proximally, generating massive, uniform compressive forces across both the subtalar and tibiotalar arthrodesis sites.

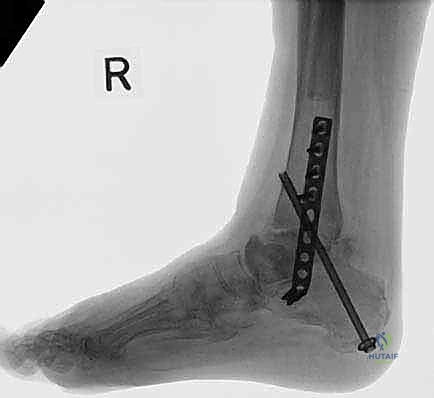
While maximal compression is maintained, the plate is secured to the tibia using heavy cortical screws (typically 4.5mm). Additionally, one or two screws are placed through the plate directly into the talar body to capture the intermediate segment and prevent rotation. For supplementary rotational stability, an independent "home run" screw (6.5mm or 7.3mm cannulated) is often driven from the posterior-inferior calcaneus, across the subtalar joint, and up into the anterior tibial metaphysis.
Final fluoroscopic images are obtained to verify hardware placement, joint compression, and overall alignment. The previously harvested and morselized autograft from the fibula is densely packed into any remaining voids around the fusion sites. The soft tissues are then closed in layers over a suction drain, paying meticulous attention to a tension-free closure of the skin to prevent marginal necrosis.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, TTC arthrodesis remains a procedure with a formidable complication profile, largely due to the compromised nature of the patient population and the inherent biological challenges of fusing two major weight-bearing joints simultaneously. The most dreaded, and unfortunately most common, complication is aseptic nonunion. The incidence of nonunion in the literature varies widely, ranging from 10% in optimized patients to upwards of 40% in high-risk cohorts, particularly those with a history of smoking, uncontrolled diabetes, or pre-existing avascular necrosis of the talus.
When a nonunion occurs, it typically presents with persistent, localized pain upon weight-bearing, swelling, and progressive hardware failure (e.g., broken screws or plate fracture). Diagnosis is confirmed via CT scan, which will demonstrate a lack of bridging trabecular bone across the arthrodesis site. Management of a symptomatic nonunion necessitates a revision surgery. This involves a complete takedown of the previous fusion site, aggressive debridement of all fibrous tissue and sclerotic bone, the re-establishment of bleeding bone beds, and the application of a new, often more robust, fixation construct. In revision scenarios, the liberal use of structural allografts or highly osteoinductive orthobiologics, such as recombinant human Bone Morphogenetic Protein-2 (rhBMP-2) or demineralized bone matrix (DBM), is strongly advocated to stimulate the stalled biological response.
Deep surgical site infection is another catastrophic complication, occurring in approximately 5% to 10% of cases, with a significantly higher incidence in the diabetic and Charcot populations. Acute infections present with erythema, fluctuance, wound dehiscence, and purulent drainage. Management requires emergent surgical intervention for thorough irrigation and excisional debridement. If the hardware remains stable and the infection is recognized early, the implants may be retained while the patient undergoes a prolonged course (typically 6 weeks) of culture-directed intravenous antibiotics. However, chronic or recalcitrant infections, particularly those associated with loose hardware or frank osteomyelitis, demand complete hardware removal, placement of an antibiotic-impregnated cement spacer, and consideration of definitive salvage procedures, which may ultimately include a below-knee amputation if the limb becomes unsalvageable.
Complications and Management Matrix
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| **A |
