Tendon Transfer for Chronic Mallet Finger and Extensor Mechanism Reconstruction
Key Takeaway
Chronic mallet finger deformities often require complex surgical intervention when conservative management fails. The Milford tendon transfer utilizes a mobilized lateral band routed through a flexor sheath pulley to restore distal interphalangeal joint extension while preventing proximal interphalangeal joint hyperextension. This comprehensive guide details the biomechanics, step-by-step surgical technique, and postoperative rehabilitation protocols essential for optimizing functional outcomes in extensor mechanism reconstructions.
INTRODUCTION TO CHRONIC MALLET FINGER DEFORMITY
The management of a chronic, neglected, or "old" mallet finger deformity presents a formidable challenge to the orthopedic hand surgeon. While acute mallet fingers (Zone I extensor tendon injuries) are typically managed successfully with strict continuous splinting, chronic lesions often demonstrate fixed biomechanical imbalances. The disruption of the terminal extensor tendon at its insertion on the distal phalanx leads to an unopposed flexion force at the distal interphalangeal (DIP) joint by the flexor digitorum profundus (FDP).
Over time, the proximal retraction of the extensor mechanism alters the delicate kinematic balance of the digit. The central slip transmits excessive extension force to the middle phalanx, while the transverse retinacular ligaments stretch, allowing the lateral bands to subluxate dorsally. This pathological cascade frequently culminates in a secondary swan-neck deformity—characterized by proximal interphalangeal (PIP) joint hyperextension and DIP joint flexion.
When conservative measures fail, or when the deformity becomes rigid and interferes with hand function, surgical reconstruction is indicated. The Milford tendon transfer is a highly effective, biomechanically sound procedure designed to correct this specific imbalance by utilizing a lateral band to create a dynamic tenodesis effect.
BIOMECHANICS AND PATHOANATOMY
To successfully execute the Milford tendon transfer, the surgeon must possess an intimate understanding of the digital extensor apparatus.
The extensor mechanism is a complex aponeurotic expansion. The extrinsic extensor tendon (extensor digitorum communis) trifurcates over the proximal phalanx. The central slip inserts onto the dorsal base of the middle phalanx, extending the PIP joint. The lateral slips join with the intrinsic tendons (lumbricals and interossei) to form the lateral bands. These bands converge distally to form the terminal tendon, which inserts onto the dorsal base of the distal phalanx to extend the DIP joint.
In a chronic mallet finger:
1. Terminal Tendon Incompetence: The primary pathology is the elongation or rupture of the terminal tendon.
2. Extensor Mechanism Retraction: The entire extensor apparatus shifts proximally.
3. Volar Plate Laxity: The increased extension force at the PIP joint gradually attenuates the volar plate.
4. Lateral Band Dorsal Migration: The lateral bands displace dorsally to the axis of rotation of the PIP joint, exacerbating PIP hyperextension.
💡 Clinical Pearl: The Tenodesis Principle
The Milford procedure relies on the tenodesis effect. By routing a detached lateral band volar to the PIP joint's axis of rotation and securing it dorsally, the transfer acts as a checkrein against PIP hyperextension while simultaneously transmitting extension forces to the DIP joint when the finger is actively extended.
PREOPERATIVE EVALUATION AND INDICATIONS
Indications for Surgery
- Chronic mallet deformity (>12 weeks old) refractory to a compliant trial of conservative splinting.
- Development of a flexible or semi-flexible secondary swan-neck deformity.
- Significant functional impairment or cosmetic dissatisfaction.
- Adequate passive range of motion (PROM) at both the PIP and DIP joints.
Contraindications
- Fixed, rigid joint contractures (requires preliminary joint release or arthrodesis).
- Severe osteoarthritis of the DIP or PIP joints.
- Inadequate soft tissue coverage or severe scarring that precludes tendon gliding.
- Non-compliant patients unable to adhere to strict postoperative rehabilitation.
SURGICAL TECHNIQUE: MILFORD TENDON TRANSFER
The Milford technique is an elegant reconstructive option that repurposes one of the lateral bands to restore the oblique retinacular ligament's function, correcting both the DIP flexion lag and the PIP hyperextension.
1. Patient Positioning and Anesthesia
- Anesthesia: Regional block (axillary or supraclavicular brachial plexus block) or wide-awake local anesthesia no tourniquet (WALANT). WALANT is highly advantageous as it allows for intraoperative active movement to assess the tension of the transfer.
- Positioning: Supine with the operative arm extended on a radiolucent hand table.
- Tourniquet: If not using WALANT, a well-padded upper arm tourniquet is applied and inflated to 250 mm Hg after exsanguination.
2. Incision and Exposure
- Make a mid-axial or slightly dorsal-lateral longitudinal incision on the least scarred side of the affected digit. The incision should extend from the metacarpophalangeal (MCP) joint to the DIP joint.
- Elevate full-thickness skin flaps, taking meticulous care to preserve the dorsal sensory branches of the digital nerves and the delicate epitenon overlying the extensor mechanism.
- Expose the entire lateral band, the extensor hood, and the flexor tendon sheath at the level of the PIP joint.
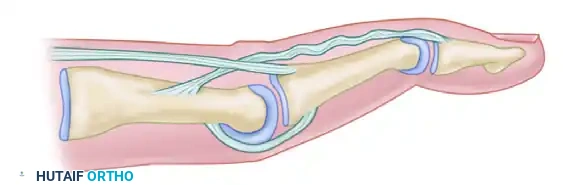
3. Lateral Band Mobilization
- Identify the lateral band on the exposed side.
- Detach the lateral band proximally, just beyond the metacarpophalangeal (MCP) joint.
- Carefully dissect the lateral band free from the central slip and the transverse retinacular ligaments, mobilizing it entirely from proximal to distal.
- CRITICAL STEP: Do not detach the lateral band from its distal insertion at the terminal tendon on the distal phalanx. The distal attachment must remain pristine to transmit the corrective force.
4. Creation of the Flexor Sheath Pulley
- Retract the neurovascular bundle volarly to expose the fibrous flexor tendon sheath at the level of the PIP joint.
- Create a small, robust pulley by making two parallel longitudinal incisions in the flexor tendon sheath opposite the PIP joint (typically utilizing the A3 or the proximal aspect of the C2 pulley).
- Ensure the underlying flexor tendons (FDS and FDP) are not inadvertently scored during this step.
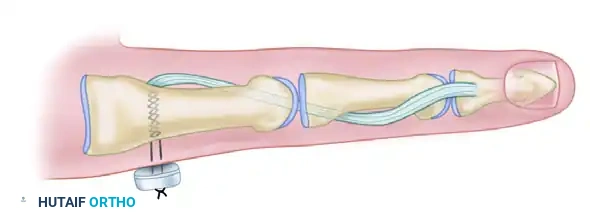
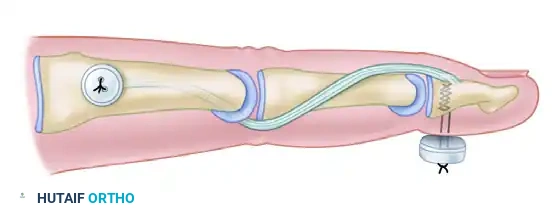
5. Tendon Routing and Tensioning
- Pass the mobilized, free proximal end of the lateral band from distal to proximal through the newly created flexor sheath pulley.
- Bring the proximal end of the lateral band dorsally, positioning it to be sutured back onto the extensor hood. It should be placed slightly dorsal to its original anatomical position on the lateral side of the extensor mechanism.
⚠️ Surgical Warning: Setting the Tension
Correct tensioning of this transfer is the most critical determinant of success. The tension must be set such that it holds the PIP joint in slight flexion (approximately 20 to 30 degrees) while the DIP joint is held in full, 0-degree extension. If the tension is too loose, the mallet deformity will recur; if too tight, a severe PIP flexion contracture will develop.
6. Fixation and Closure
- Once the correct tension is achieved, suture the lateral band to the extensor hood using a non-absorbable 4-0 or 5-0 braided polyester or nylon suture. Use a weaving technique or a modified Kessler stitch for secure fixation.
- Transarticular Fixation: To protect the delicate repair from early mechanical failure, drive a 0.045-inch (1.14 mm) Kirschner wire (K-wire) obliquely across the PIP joint. The joint must be pinned in the slightly flexed position (20-30 degrees) established during tensioning.
- Note: Some surgeons also choose to pin the DIP joint in full extension, though the primary text emphasizes PIP protection.
- Deflate the tourniquet, achieve meticulous hemostasis, and irrigate the wound.
- Close the skin with interrupted 5-0 nylon sutures.
- Apply a non-adherent dressing, followed by a conforming, compressive dressing. Support the finger, hand, and wrist with a volar plaster splint placed over adequate padding to ensure postoperative comfort and absolute protection of the repair.
POSTOPERATIVE REHABILITATION PROTOCOL
The postoperative management following a Milford tendon transfer requires a delicate balance between protecting the repair and preventing debilitating joint stiffness.
- Days 0 to 14: The patient remains in the initial bulky postoperative splint. Elevation and strict immobilization are maintained. At 10 to 14 days, the splint is removed in the clinic, and the skin sutures are extracted. A new, custom-molded thermoplastic volar splint is fabricated, maintaining the PIP in slight flexion and the DIP in extension.
- Weeks 3 to 4: The transarticular K-wire is removed in the clinic. This marks the beginning of the protected mobilization phase.
- Weeks 4 to 8: Between exercise periods, the finger must be strictly protected with the volar removable splint. The splint should be worn continuously at night and during the day, removed only for specific, therapist-directed active range of motion (AROM) exercises. Exercises focus on gentle active flexion and extension, avoiding any passive stretching that could elongate the transfer.
- Week 8 and Beyond: Wearing of the protective splint can be gradually discontinued. Progressive strengthening and gradual improvement in motion are encouraged. Full maturation of the tendon transfer and final range of motion may take up to 6 months.
SWAN-NECK DEFORMITY AND SORL RECONSTRUCTION
While the Milford procedure addresses a chronic mallet finger that is evolving into a swan-neck deformity, established swan-neck deformities with severe volar plate laxity may require a dedicated Spiral Oblique Retinacular Ligament (SORL) reconstruction.
Pathoanatomy of Swan-Neck Deformity
The pathological condition of a swan-neck deformity involves the hyperextension of the PIP joint combined with an extensor lag (flexion) at the DIP joint. This is fundamentally driven by a combination of:
1. Laxity or rupture of the volar plate at the PIP joint.
2. Dorsal subluxation of the lateral bands.
3. Imbalance of the extensor mechanism.
Palmaris Longus Tenodesis (SORL Reconstruction)
To correct the imbalance at both the PIP and DIP joints simultaneously, a free tendon graft—most commonly the palmaris longus—can be utilized to reconstruct the oblique retinacular ligament.
In this technique, the palmaris longus graft is routed to provide a dynamic tenodesis. The graft is secured distally to the terminal extensor tendon, routed volarly along the middle phalanx, passed volar to the PIP joint axis (acting as a volar plate checkrein to prevent hyperextension), and secured proximally to the proximal phalanx or flexor sheath. As the finger extends, the graft tightens, pulling the DIP joint into extension while simultaneously preventing the PIP joint from hyperextending.
EXTENSOR TENDON ZONES AND REPAIR STRATEGIES
Understanding the specific anatomical zones of the extensor mechanism is paramount, as the morphology of the tendon dictates the surgical repair strategy.
Zone II: The Middle Phalanx
Zone II encompasses the area over the middle phalanx. In this region, the extensor mechanism transitions from the lateral bands into the flat, conjoined terminal tendon.
Surgical Challenges in Zone II:
The flat, thin nature of the tendon in this area severely limits the suture configurations that can be utilized. Bulky core sutures will impede gliding beneath the skin and may cause necrosis of the delicate tendon ends.
Suture Techniques for Zone II:
* Lateral tendons lacerated proximal to their insertion can be sutured with a simple figure-of-eight mattress stitch or a roll stitch. These provide adequate apposition for thin, flat tendons.
* For slightly thicker tendon segments where greater tensile strength is required, the Kleinert modification of the Bunnell suture or modified Kessler sutures are biomechanically stronger than a simple figure-of-eight or mattress suture.
* The Silfverskiöld Cross Stitch: A continuous peripheral suture reinforced with a Silfverskiöld cross stitch provides a highly robust repair. This technique distributes the tension evenly across the flat tendon interface, minimizing the risk of suture pull-through while maintaining a low profile to prevent adhesions to the overlying dermis.
Zone III: The Proximal Interphalangeal Joint
Zone III is the area directly overlying the proximal interphalangeal (PIP) joint. This zone houses the critical insertion of the central slip onto the base of the middle phalanx.
Pathology in Zone III:
Rupture or acute transection of the extensor mechanism in Zone III primarily involves the central slip. If left untreated, the lateral bands will eventually subluxate volarly, dropping below the axis of rotation of the PIP joint. They then become flexors of the PIP joint while continuing to extend the DIP joint, resulting in the classic Boutonniere deformity.
Surgical repair in Zone III requires meticulous reattachment of the central slip to the middle phalanx base, often utilizing bone anchors or transosseous sutures if the avulsion is flush with the bone, followed by pinning of the PIP joint in full extension to allow the central slip to heal without tension.
COMPLICATIONS AND PITFALLS
Surgeons performing tendon transfers for chronic mallet fingers must be vigilant regarding potential complications:
- Loss of Reduction/Recurrence: Usually due to inadequate tensioning of the lateral band during the transfer, or premature removal of the transarticular K-wire. Strict adherence to the 3-4 week pinning protocol is mandatory.
- PIP Joint Stiffness: Over-tensioning the transfer or prolonged immobilization beyond 4 weeks can lead to a fixed PIP flexion contracture. The K-wire must secure the PIP in no more than 20-30 degrees of flexion.
- Pin Tract Infection: The transarticular K-wire is a conduit for bacteria. Meticulous pin site care and early oral antibiotics for superficial erythema are required.
- Skin Necrosis: The dorsal skin over the PIP and DIP joints is exceptionally thin. Undermining must be performed in the correct plane (above the epitenon) to preserve the subdermal vascular plexus.
CONCLUSION
The correction of an old, chronic mallet finger deformity requires a sophisticated understanding of digital biomechanics. The Milford tendon transfer provides a reliable, dynamic solution by repurposing the lateral band to act as a tenodesis, restoring DIP extension and preventing secondary swan-neck deformities. By adhering to strict surgical principles—meticulous tissue handling, precise tensioning, secure transarticular fixation, and a rigid postoperative rehabilitation protocol—the orthopedic surgeon can restore both form and function to the compromised digit.
You Might Also Like
