Scapulothoracic Bursitis: Unmasking a Mimic of Refractory Lateral Epicondylitis

Key Takeaway
Scapulothoracic bursitis diagnosis often involves a comprehensive physical exam, revealing tenderness, crepitus, and scapular dyskinesis, particularly after conservative treatments for conditions like lateral epicondylitis fail. MRI is crucial, demonstrating fluid and soft tissue thickening within the bursa, confirming the true origin of persistent pain in the scapulothoracic region.
A 48-year-old carpenter presents with persistent lateral elbow pain, unresponsive to 6 months of conservative management for lateral epicondylitis. He reports a remote shoulder trauma and a "grinding" sensation at the medial scapular border. On examination, you observe a "hitch" in his scapulohumeral rhythm and Type II scapular dyskinesis. How do you approach this case, and what is your leading differential?
Candidate: I suspect the primary pathology is not the elbow, but rather scapulothoracic bursitis or snapping scapula syndrome causing secondary distal kinetic chain overload. I would perform a thorough clinical exam focusing on scapular stability, specifically the Scapular Assistance Test (SAT) and Kibler’s lateral slide test. I'd order radiographs of the scapula and, if negative for bony lesions, an MRI to evaluate for bursal inflammation or other soft tissue pathology.
Candidates often fixate on the lateral elbow, suggesting repeat steroid injections, MRI of the elbow, or even surgical exploration of the epicondyle. Failing to recognize the proximal scapular "kinetic chain" pathology will lead to a failure of this station.
The candidate must demonstrate a "kinetic chain" mindset. They should frame the lateral epicondylitis as a distal manifestation of proximal scapular dyskinesis. Key points: 1. Confirm diagnosis via diagnostic bursal injection. 2. Rule out cervical radiculopathy. 3. Use 3D CT to assess for osseous structural impingement (Luschka's tubercle). 4. Emphasize that surgical intervention is only a final resort after structured rehabilitation of the scapular stabilizers (serratus/lower trap).
You have decided to proceed with arthroscopic scapulothoracic decompression. Describe the relevant surgical anatomy you must navigate to avoid iatrogenic injury. Please refer to the anatomy below.
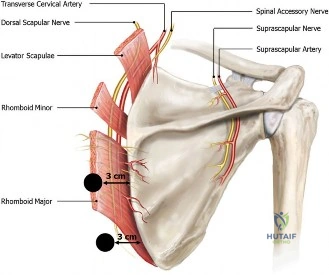
Candidate: The critical structures are the neurovascular bundles. Specifically, the dorsal scapular nerve and artery run along the medial border of the scapula, deep to the rhomboids. I must keep my portals at least 3cm medial to the scapular border to avoid this bundle. Furthermore, I must be cognizant of the long thoracic nerve on the lateral chest wall and avoid deep or medial trocar penetration to prevent pneumothorax.
Neglecting to mention the dorsal scapular nerve, or suggesting an approach that risks pleural penetration by using a medial-to-lateral trajectory without identifying the safe portals defined by Bell et al.
The candidate should structure the answer by layers: 1. Superficial (trapezius), 2. Intermediate (rhomboids/levator scapulae), and 3. Deep (serratus/subscapularis). They should explicitly state the importance of patient positioning ("chicken wing" to clear the scapula from the thoracic wall) and emphasize that portals must be placed 3-4cm medial to the scapular border to protect the dorsal scapular neurovascular bundle.
Look at this imaging. What is the clinical significance of these findings, and how does it influence your surgical plan?
Candidate: The image shows evidence of potential structural impingement or bursal space narrowing. If this is a CT reconstruction, I am looking for the "hooked" superomedial angle (Luschka's tubercle). If it is an MRI, I am looking for bursal fluid (T2 high signal). My surgical plan involves a partial scapulectomy of the superomedial angle if an osseous prominence is confirmed, alongside a thorough arthroscopic bursectomy.
Assuming surgery is purely for soft-tissue "cleaning." Failing to address the underlying osseous morphology (the "hook") means the bursitis will likely recur even after soft-tissue resection.
The candidate should explain that the diagnostic workup distinguishes between "soft tissue" snapping (treated with bursectomy) and "osseous" snapping (requiring partial scapulectomy). They should mention that 3D CT is the Gold Standard for quantifying the superomedial angle's morphology and that the goal of surgery is to recreate a clearance between the scapula and the rib cage to allow smooth gliding.
