Operative Management of Peripheral Nerve Injuries of the Shoulder Girdle
Key Takeaway
Peripheral nerve injuries around the shoulder, including the axillary, suprascapular, and musculocutaneous nerves, require meticulous clinical evaluation. Diagnosis often hinges on differentiating specific muscle weakness, such as isolating biceps function from the brachioradialis. Surgical management ranges from nerve decompression, such as releasing the transverse scapular ligament, to complex nerve grafting or tendon transfers, depending on the injury mechanism and patient age.
Comprehensive Introduction and Patho-Epidemiology
Peripheral nerve injuries around the shoulder girdle present an exceptionally complex diagnostic and therapeutic challenge for the orthopedic surgeon, neurosurgeon, and peripheral nerve specialist. The intricate neurovascular anatomy of the brachial plexus and its terminal branches—specifically the axillary, suprascapular, and musculocutaneous nerves—renders them highly susceptible to a variety of traumatic, traction, and compressive insults. The profound functional deficits resulting from these injuries not only compromise glenohumeral kinematics but also severely diminish the patient's overall upper extremity utility and quality of life. Accurate clinical examination, augmented by sophisticated electrodiagnostic studies and advanced imaging modalities, is paramount in establishing a definitive diagnosis and formulating an optimal treatment algorithm.
The epidemiology of shoulder girdle neuropathies is diverse, encompassing high-energy trauma, sports-related repetitive microtrauma, and iatrogenic injuries. Traction neuropathies are frequently observed in the context of high-velocity motor vehicle collisions or severe contact sports injuries, where the shoulder is forcefully depressed while the cervical spine is laterally flexed to the contralateral side. Conversely, compressive neuropathies, such as Quadrilateral Space Syndrome or suprascapular nerve entrapment at the spinoglenoid notch, are more insidious, often presenting in overhead athletes such as baseball pitchers, volleyball players, and swimmers. Furthermore, the rising volume of complex open and arthroscopic shoulder reconstructions, including the Latarjet procedure, reverse total shoulder arthroplasty, and massive rotator cuff repairs, has led to a parallel increase in iatrogenic nerve injuries.
Understanding the patho-epidemiology requires a firm grasp of nerve injury classifications, primarily the Seddon and Sunderland systems. Neuropraxic injuries, characterized by focal demyelination without axonal disruption, typically recover spontaneously within weeks to months. However, axonotmetic injuries (where the axon is disrupted but the endoneurial tubes remain intact) and neurotmetic injuries (complete transection of the nerve and its connective tissue framework) necessitate a highly strategic approach. In the context of the shoulder girdle, the proximity of the injury to the target motor endplates is a critical prognostic factor. Because regenerating axons grow at a rate of approximately 1 mm per day (or 1 inch per month), proximal injuries to the brachial plexus or its immediate terminal branches face a race against time before irreversible motor endplate degeneration occurs, typically within 12 to 18 months.
This comprehensive guide details the surgical anatomy, pathomechanics, clinical evaluation, and operative management of these critical nerve injuries. It is designed to provide evidence-based, highly technical protocols for orthopedic residents, upper extremity fellows, and practicing consultants who are tasked with navigating the formidable challenges of shoulder girdle nerve reconstruction and salvage.
Detailed Surgical Anatomy and Biomechanics
A profound, three-dimensional understanding of the surgical anatomy and biomechanics of the axillary, suprascapular, and musculocutaneous nerves is the foundation of safe and effective operative intervention. The shoulder girdle is a crowded anatomic crossroad, where terminal nerve branches must navigate through narrow fibro-osseous tunnels, muscular fascial planes, and dynamic joint spaces.
The Axillary Nerve
The axillary nerve is a major terminal branch of the posterior cord of the brachial plexus, carrying fibers primarily from the C5 and C6 nerve roots. It provides critical motor innervation to the deltoid (anterior, middle, and posterior heads) and the teres minor muscles. Additionally, it supplies sensory innervation to the lateral shoulder—classically described as the "regimental badge" area—via the superior lateral cutaneous nerve of the arm.
After branching from the posterior cord anterior to the subscapularis muscle, the axillary nerve courses inferiorly and posteriorly to exit the axilla through the quadrilateral space. The boundaries of the quadrilateral space are strictly defined and must be thoroughly understood for both posterior surgical approaches and the decompression of Quadrilateral Space Syndrome (QSS). The boundaries are:
* Superiorly: Teres minor (and the inferior capsule of the glenohumeral joint).
* Inferiorly: Teres major.
* Medially: Long head of the triceps brachii.
* Laterally: Surgical neck of the humerus.
Within this confined space, the axillary nerve is accompanied by the posterior humeral circumflex artery. Upon exiting the quadrilateral space, the nerve lies in direct contact with the surgical neck of the humerus, making it exceptionally vulnerable during proximal humerus fractures. It then divides into anterior and posterior branches. The anterior branch winds horizontally around the surgical neck, deep to the deltoid, supplying the anterior and middle deltoid. The posterior branch supplies the teres minor and posterior deltoid before piercing the deep fascia to terminate as the superior lateral cutaneous nerve. Biomechanically, the loss of axillary nerve function results in a catastrophic failure of shoulder abduction and forward elevation, as the deltoid is the primary prime mover for these actions beyond the initial 15 to 30 degrees initiated by the supraspinatus.
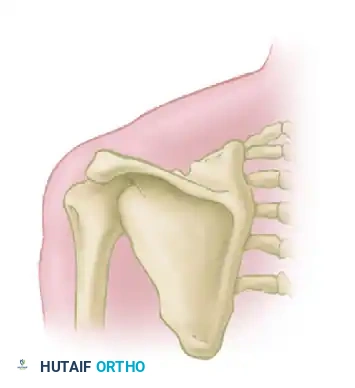
The Suprascapular Nerve
The suprascapular nerve arises directly from the upper trunk of the brachial plexus, carrying fibers from the C5 and C6 roots. It is a mixed motor and sensory nerve, providing indispensable motor supply to the supraspinatus and infraspinatus muscles, as well as sensory branches to the posterior glenohumeral capsule, the acromioclavicular joint, and the subacromial bursa.
The nerve travels obliquely across the posterior triangle of the neck, passing deep to the trapezius and the omohyoid muscle, before reaching the superior border of the scapula. Here, it encounters its first major anatomic choke point: the suprascapular notch. The notch is roofed by the transverse scapular ligament. Entrapment at this site compromises both the supraspinatus (abduction) and the infraspinatus (external rotation). After innervating the supraspinatus, the nerve courses laterally and inferiorly around the base of the scapular spine to enter the infraspinatus fossa through a second choke point: the spinoglenoid notch, covered by the spinoglenoid ligament. Entrapment here—frequently secondary to paralabral cysts associated with superior labrum anterior and posterior (SLAP) tears—results in isolated infraspinatus weakness, manifesting as a profound loss of external rotation power in adduction.
The Musculocutaneous Nerve
The musculocutaneous nerve is the primary terminal branch of the lateral cord of the brachial plexus, carrying fibers from C5, C6, and C7. It provides essential motor innervation to the anterior compartment of the arm, specifically the coracobrachialis, biceps brachii, and brachialis muscles. It continues distally as the lateral antebrachial cutaneous nerve, supplying sensation to the lateral aspect of the forearm.
Surgically, the nerve originates at the inferior border of the pectoralis minor. It classically pierces the coracobrachialis muscle approximately 3 to 8 cm distal to the tip of the coracoid process. This measurement is of paramount importance during the deltopectoral approach, particularly during the Latarjet procedure, where medial retraction of the conjoined tendon places the nerve at significant risk of neuropraxia or structural failure. After piercing the coracobrachialis, the nerve descends obliquely between the biceps brachii and the brachialis, innervating both. It then emerges lateral to the biceps tendon, piercing the deep brachial fascia proximal to the elbow crease to become a purely sensory nerve. Biomechanically, while the musculocutaneous nerve is the primary flexor of the elbow and a strong supinator of the forearm, its isolated loss can sometimes be masked by the compensatory actions of the brachioradialis (radial nerve) and pronator teres (median nerve).
Exhaustive Indications and Contraindications
The decision-making process regarding the operative management of shoulder girdle nerve injuries requires a meticulous synthesis of the injury mechanism, the temporal progression of the deficit, and the patient's functional demands. The overarching goal is to restore functional motor control before irreversible end-organ muscle atrophy occurs. Operative intervention is generally categorized into neurolysis, primary nerve repair (neurorrhaphy), nerve grafting, and nerve or tendon transfers.
| Procedure Category | Primary Indications | Absolute and Relative Contraindications |
|---|---|---|
| Surgical Exploration and Neurolysis | - Closed traction injuries with no clinical/EMG recovery at 3-6 months. - Quadrilateral Space Syndrome refractory to 6 months of conservative care. - Suprascapular nerve entrapment at the notch with progressive atrophy. - Intraoperative identification of nerve tethering without complete transection. |
- Early closed injuries (< 3 months) without serial EMG documentation. - Spontaneous clinical improvement observed on serial exams. - Severe medical comorbidities precluding general anesthesia. |
| Primary Neurorrhaphy (Direct Repair) | - Sharp, clean lacerations (e.g., stab wounds) presenting acutely. - Iatrogenic transection identified intraoperatively. - Ability to achieve tension-free coaptation of nerve ends. |
- Massive crush injuries with extensive zones of contusion. - Delayed presentation where nerve retraction prevents tension-free repair. - Segmental nerve loss requiring grafting. |
| Nerve Grafting (Autograft/Allograft) | - Delayed presentations of complete lacerations with gap formation. - Blast injuries or high-energy trauma with a large zone of injury requiring resection back to healthy fascicles. - Neuroma-in-continuity with no distal conduction, requiring resection. |
- Gap lengths exceeding the biological capacity for regeneration (relative). - Lack of available autograft donor sites (e.g., sural nerve previously harvested). - Poor vascular soft tissue bed over the intended graft site. |
| Nerve Transfers (Neurotization) | - Proximal root avulsions (e.g., C5-C6 avulsion). - Very delayed presentations (> 9-12 months) where proximal grafting would take too long to reach the motor endplate. - High brachial plexus injuries requiring rapid reinnervation of critical targets (e.g., Oberlin transfer for elbow flexion). |
- Advanced muscle atrophy and fatty infiltration (e.g., Goutallier Grade 3/4) of the target muscle. - Lack of a healthy, expendable donor nerve fascicle. - Severe joint contracture or ankylosis of the target joint. |
| Tendon/Muscle Transfers | - Irreversible nerve palsy with complete failure of nerve reconstruction. - Presentation > 18-24 months post-injury with absent motor endplates. - Salvage for failed prior nerve transfers. |
- Stiff, non-yielding joint (requires full passive range of motion prior to transfer). - Inadequate strength of the proposed donor muscle (must be at least Grade 4/5). - Lack of patient compliance for complex postoperative rehabilitation. |
Pre-Operative Planning, Templating, and Patient Positioning
Pre-operative planning for peripheral nerve surgery is arguably as critical as the execution of the procedure itself. The evaluation begins with an exhaustive clinical examination. For the axillary nerve, the surgeon must assess the "regimental badge" sensory area and isolate the deltoid by testing abduction and extension in the plane of the scapula. For the suprascapular nerve, atrophy in the supraspinatus and infraspinatus fossae is often visible; external rotation strength must be tested with the arm adducted to isolate the infraspinatus from the teres minor.
Evaluating the musculocutaneous nerve presents a unique clinical pitfall: masked biceps paralysis. Flexion of the elbow by the brachioradialis (innervated by the radial nerve) may be strong enough to completely mask biceps paralysis. A patient with a transected musculocutaneous nerve can often still flex their elbow against gravity. To accurately examine the musculocutaneous nerve, the clinician must position the patient's forearm in full supination to disadvantage the brachioradialis, ask the patient to flex the elbow against resistance, and physically palpate the biceps muscle belly and its distal tendon to identify specific muscle contractions.
Electrodiagnostic studies, comprising Electromyography (EMG) and Nerve Conduction Studies (NCS), are the cornerstone of pre-operative planning. However, timing is critical. Wallerian degeneration takes up to 3 weeks to manifest electrodiagnostically. Therefore, an EMG performed immediately after injury is of little value. Baseline studies at 3 to 4 weeks will show fibrillation potentials and positive sharp waves in denervated muscles. Serial EMGs at 3 and 6 months are utilized to detect nascent motor unit action potentials (MUAPs), which herald early reinnervation long before clinical strength returns.
Advanced imaging has revolutionized the pre-operative templating of nerve injuries. High-resolution Magnetic Resonance Neurography (MRN) utilizing 3-Tesla scanners with STIR and T2 fat-suppressed sequences can visualize the nerve fascicles, identify neuromas, and assess the degree of target muscle denervation edema and fatty infiltration. In cases of suspected Quadrilateral Space Syndrome, a subclavicular arteriogram or dynamic MR angiography is often indicated. The study is considered positive if occlusion of the posterior humeral circumflex artery occurs with less than 60 degrees of shoulder abduction and external rotation. Diagnostic local anesthetic blocks, accomplished by inserting needles along the posterior border of the deltoid into the quadrilateral space, can also confirm the diagnosis if symptoms are temporarily relieved.
Patient positioning is dictated by the selected surgical approach. For anterior brachial plexus explorations or musculocutaneous nerve repairs, the patient is placed supine with the arm abducted on a hand table. For axillary nerve explorations via a posterior approach, or suprascapular nerve decompressions, the lateral decubitus or prone position is preferred. The operative arm must be draped free to allow intraoperative manipulation, assessment of tension on nerve repairs, and dynamic testing of joint range of motion.
Step-by-Step Surgical Approach and Fixation Technique
Surgical intervention for peripheral nerve injuries demands meticulous soft tissue handling, precise hemostasis, and the utilization of microsurgical techniques. Operating loupes (minimum 3.5x magnification) or an operating microscope are mandatory for epineurial and perineurial dissections.
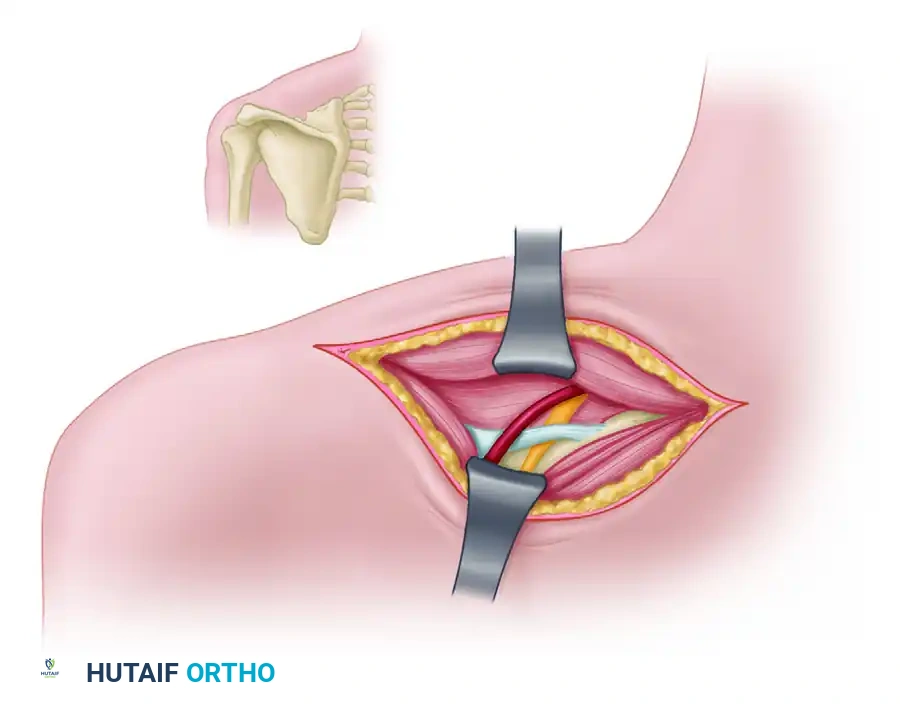
Suprascapular Nerve Decompression at the Notch
When conservative management for suprascapular nerve entrapment at the suprascapular notch fails, surgical decompression via division of the transverse scapular ligament is indicated. This can be performed arthroscopically or via a classic open posterior approach. The open approach remains the gold standard for complex revisions or when direct visualization of a neuroma is required.
Step-by-Step Open Posterior Approach:
1. Positioning and Preparation: The patient is placed in the lateral decubitus or prone position. All bony prominences are meticulously padded. The operative arm is draped free to allow manipulation.
2. Incision: A linear, transverse incision is made parallel to and approximately 2 cm superior to the spine of the scapula, extending over the supraspinatus fossa.
3. Superficial Dissection: The subcutaneous tissues are divided to expose the trapezius muscle fascia. The trapezius muscle fibers are identified. Depending on the patient's anatomy, they can be split in line with their fibers using blunt dissection, or detached from the scapular spine and retracted superiorly to expose the underlying supraspinatus muscle.
4. Deep Exposure: The supraspinatus muscle is carefully mobilized from its fascial envelope and retracted posteriorly and inferiorly using a blunt retractor (e.g., a Richardson or Darrach retractor). This exposes the bony floor of the supraspinatus fossa.
5. Identifying the Notch: Blunt dissection proceeds laterally and superiorly along the superior border of the scapula until the suprascapular notch is palpated. The coracoid process anteriorly serves as a reliable landmark pointing toward the notch.
Surgical Warning: The "Army over Navy" Rule
Meticulous dissection is required at the notch. The suprascapular artery passes above (superior to) the transverse scapular ligament, while the suprascapular nerve passes beneath (inferior to) the ligament through the notch. Iatrogenic injury to the artery can cause severe bleeding that rapidly obscures the surgical field and places the underlying nerve at risk during blind attempts at hemostasis.
- Ligament Release: A blunt right-angle probe or a Freer elevator is carefully passed beneath the transverse scapular ligament to protect the underlying nerve. The ligament is then sharply divided using a scalpel (No. 15 blade) or a 2mm Kerrison rongeur.
- Neurolysis and Inspection: Once the ligament is completely divided, the nerve is inspected under magnification. The nerve should be gently mobilized using vessel loops. Epineurotomy (longitudinal slitting of the epineurium) is rarely required unless severe intrinsic scarring or an hourglass constriction is present. The nerve should be completely free from tethering throughout its excursion during shoulder motion.
- Closure: Hemostasis is achieved. The supraspinatus is allowed to fall back into its anatomic position. If the trapezius was detached, it is meticulously repaired to the scapular spine using heavy non-absorbable sutures (e.g., #2 FiberWire) through transosseous drill holes to prevent postoperative weakness and cosmetic deformity. The skin is closed in a layered fashion.
Axillary Nerve Exploration and Repair
For axillary nerve injuries requiring repair, the surgical approach depends on the zone of injury. Proximal injuries near the posterior cord require a standard deltopectoral approach with extension into the axilla. Distal injuries at the quadrilateral space are best approached posteriorly.
For the posterior approach, an incision is made along the posterior border of the deltoid. The interval between the posterior deltoid and the long head of the triceps is developed. The teres minor (superior) and teres major (inferior) are identified. The axillary nerve and posterior humeral circumflex artery are located exiting the quadrilateral space.
If a neuroma-in-continuity is found, intraoperative nerve stimulation is performed. If no distal muscle action potential is generated, the neuroma is resected back to healthy, pouting fascicles ("mushrooming" appearance). If the resulting gap is less than 1-2 cm and can be closed without tension with the arm in adduction, primary epineurial repair is performed using 8-0 or 9-0 nylon sutures under the microscope. If the gap is larger, autologous sural nerve cable grafts are harvested. The grafts are reversed to prevent axonal loss down sensory branches and are sutured into place using fibrin glue augmentation.
Musculocutaneous Nerve Reconstruction
Injuries to the musculocutaneous nerve are approached via an anterior longitudinal incision over the medial border of the biceps brachii. The interval between the biceps and the neurovascular bundle is developed. The nerve is traced proximally to its origin at the lateral cord and distally as it pierces the coracobrachialis.
In cases of delayed presentation (>12 months) or proximal root avulsions where grafting is not viable, nerve transfers have revolutionized the management of musculocutaneous nerve palsy. The Oberlin transfer involves transferring redundant motor fascicles from the ulnar nerve (typically those supplying the flexor carpi ulnaris) directly to the motor branch of the biceps. Similarly, fascicles from the median nerve (supplying the flexor carpi radialis) can be transferred to the brachialis motor branch (the double fascicular transfer). This places regenerating axons millimeters away from the motor endplates, resulting in rapid and highly reliable restoration of elbow flexion.
Complications, Incidence Rates, and Salvage Management
Surgical management of peripheral nerve injuries is fraught with potential complications. The surgeon must be prepared to manage both intraoperative adverse events and long-term failures of nerve regeneration. The incidence of complications varies widely based on the mechanism of injury, patient age, and the specific reconstructive technique employed.
| Complication | Estimated Incidence | Etiology / Risk Factors | Prevention and Salvage Management |
|---|---|---|---|
| Failure of Reinnervation | 15% - 30% (Higher in grafts > 5cm) | Delay to surgery (>6-9 months), excessive tension on repair, poor vascular bed, advanced age. | Prevention: Tension-free repair, use of appropriate cable grafts, early intervention. Salvage: Tendon transfers (e.g., Latissimus dorsi transfer for failed axillary nerve; Steindler flexorplasty for failed MSK nerve). |
| Neuroma Formation | 5% - 10% | Inadequate resection of the primary injury zone, escaped regenerating axons at the coaptation site. | Prevention: Meticulous microsurgical coaptation, wrapping the repair site in a vascularized fascial flap or nerve conduit. Salvage: Re-exploration, neuroma excision, and secondary grafting or targeted muscle reinnervation (TMR) for pain control. |
| Iatrogenic Vascular Injury | 1% - 3% | Dissection near the suprascapular artery or posterior humeral circumflex artery without adequate visualization. | Prevention: Strict adherence to anatomic landmarks ("Army over Navy"), bipolar electrocautery, careful blunt dissection. Salvage: Immediate direct pressure, proximal and distal vascular control, primary vascular repair or ligation if collateral flow is sufficient. |
| Complex Regional Pain Syndrome (CRPS) | 2% - 5% | Prolonged immobilization, severe initial nerve crush, hyperalgesia. | Prevention: Early mobilization of adjacent joints, adequate postoperative analgesia, early recognition. Salvage: Aggressive physical therapy, neuropathic pain modulators (gabapentin, pregabalin), stellate ganglion blocks. |
| Donor Site Morbidity (Sural Nerve) | 10% - 20% | Harvest of the sural nerve for cable grafting. | Prevention: Careful subcutaneous dissection, avoiding injury to the lesser saphenous vein. Salvage: Patient education regarding expected lateral foot numbness; symptomatic neuromas at the harvest site may require excision and burying into muscle. |
For irreversible axillary nerve palsy where nerve reconstruction has failed or presents too late, salvage procedures are required to restore shoulder abduction and forward elevation. Tendon and muscle transfers for paralysis of the deltoid typically involve transferring the origin of the pedicled latissimus dorsi or the pectoralis major to the proximal humerus or the acromion. These massive transfers require rigorous postoperative rehabilitation and rely heavily on the patient's ability to cortically remap the transferred muscle to perform a new biomechanical function.
Phased Post-Operative Rehabilitation Protocols
Regardless of the specific nerve addressed or the reconstructive technique utilized, postoperative rehabilitation follows a strictly phased, biologically respectful protocol. The rehabilitation program must balance the necessity of protecting the delicate microsurgical nerve repair with the imperative to prevent debilitating joint contractures and muscle atrophy.
Phase I: Protection and Healing (Weeks 0-3)
The primary objective during the initial three weeks is the absolute protection of the nerve coaptation site. Tension across a nerve repair is the single most detrimental factor to axonal regeneration.
* Immobilization: The patient is immobilized in a sling, shoulder immobilizer, or custom orthosis designed to remove tension from the specific repair site. For example, axillary and suprascapular nerve repairs may require a customized abduction orthosis to prevent adduction and internal rotation stretch. Musculocutaneous nerve repairs require the elbow to be immobilized in 90 to 100 degrees of flexion with the forearm supinated.
* Adjacent Joint Motion: Passive range of motion (PROM) and active range of motion (AROM) of adjacent, uninvolved joints (cervical spine, wrist, digits) are instituted immediately to prevent distal stiffness and encourage venous and lymphatic drainage.
* Strict Avoidance: Any movement that places a longitudinal stretch on the repaired nerve is strictly contraindicated.
Phase II: Early Controlled Motion (Weeks 3-6)
As the epineurial healing solidifies, controlled motion is gradually introduced to prevent perineurial adhesions and joint capsular contractures.
* Gradual PROM: The therapist gently introduces PROM to the affected joint within pre-defined safe zones established by the surgeon. For musculocutaneous repairs, elbow extension is increased by 10 to 15 degrees per week.
* Active-Assisted Motion: Initiation of active-assisted range of motion (AAROM) is permitted as tolerated, ensuring no sudden, jerky movements occur.
* Modality Integration: Neuromuscular electrical stimulation (NMES) is frequently utilized during this phase. Applying NMES directly to the denervated target muscles (e.g., the deltoid or biceps) helps maintain muscle bulk and delays irreversible fibrosis while awaiting the slow process of axonal reinnervation.
Phase III: Strengthening and Cortical Remapping (Weeks 6-12+)
Once the repair is deemed biologically stable, the focus shifts to maximizing functional return.
* Active Range of Motion: Progression to full AROM is encouraged.
* Strengthening: Isotonic and isometric strengthening begins only once there is clinical or EMG evidence of motor return. Premature strengthening of denervated muscle is futile and can lead to frustration and tendinopathy of compensatory muscles.
* Cortical Remapping: In cases of nerve transfers (e.g., Oberlin transfer), the patient must learn to fire the donor nerve to activate the recipient muscle. For an Oberlin transfer, the patient is instructed to actively flex their wrist (firing the ulnar nerve) while attempting to flex their elbow. Over time, neuroplasticity allows the brain to bypass the wrist flexion cue, resulting in spontaneous elbow flexion.
Phase IV: Long-Term Monitoring and Maintenance (Months 3-24)
Because nerve regeneration occurs at approximately 1 mm per day, patients must be extensively counseled pre- and post-operatively that maximal functional recovery may take 12 to 24 months.
* Serial Monitoring: Regular clinical follow-up and serial EMG studies at 3, 6, 12, and 18 months are critical. These studies monitor the progress of the advancing Tinel's sign and the development of nascent motor units.
* Decision for Salvage: If serial monitoring demonstrates an arrest in regeneration or failure to reach the target muscle by 12 to 18 months, the rehabilitation team and surgeon must pivot to discussing secondary salvage procedures, such as the tendon transfers detailed previously.
Summary of Landmark Literature and Clinical Guidelines
The operative management of shoulder girdle neuropathies has evolved significantly over the past century, guided by landmark anatomical studies and pioneering microsurgical techniques. A comprehensive understanding of the literature is essential for the modern orthopedic surgeon.
The foundational principles of nerve injury classification and the timing of intervention were established by Seddon (1943) and later refined by Sunderland (1951). Their work dictated the classic paradigm of observing closed nerve injuries for 3 to 6 months before proceeding with exploration, a guideline that remains the standard of care today.
Regarding Quadrilateral Space Syndrome, the seminal work by Cahill and Palmer (1983) defined the clinical presentation and the diagnostic utility of subclavian angiography, cementing the posterior approach for decompression as the definitive treatment for refractory cases. Their findings emphasized that QSS is primarily a dynamic compression issue, heavily reliant on provocative positioning for diagnosis.
The management of suprascapular nerve entrapment was revolutionized by the anatomical studies of Rengachary et al. (1979), who classified the varied morphology of the suprascapular notch and its direct correlation with entrapment risk. More recently, the advent of arthroscopic techniques, pioneered by surgeons such as Lafosse, has provided a minimally invasive alternative to the open posterior approach, demonstrating equivalent decompression efficacy with reduced morbidity to the trapezius insertion.
Perhaps the most dramatic paradigm shift in the management of proximal upper extremity nerve injuries has been the popularization of nerve transfers. The landmark paper by Oberlin et al. (1994) described the transfer of ulnar nerve fascicles to the biceps motor branch, bypassing the need for lengthy, unpredictable nerve grafts in brachial plexus injuries. This technique consistently yields Medical Research Council (MRC) Grade 3 or 4 elbow flexion in over 80% of appropriately selected patients. Subsequent expansions of this concept, such as the double fascicular transfer described by Mackinnon and colleagues, have further optimized outcomes for musculocutaneous nerve restoration, setting a new gold standard
