Posterior Deltoid-to-Triceps Transfer: Comprehensive Surgical Guide
Key Takeaway
The posterior deltoid-to-triceps transfer, pioneered by Moberg, is a critical reconstructive procedure designed to restore active elbow extension in patients with tetraplegia. By transferring the posterior deltoid to the triceps insertion, surgeons can re-establish the biomechanical linkage necessary for overhead reach, wheelchair transfers, and pressure relief. This guide details the surgical approach, graft interposition techniques, and rigorous postoperative protocols required for optimal functional outcomes.
Comprehensive Introduction and Patho-Epidemiology
The restoration of active elbow extension represents a watershed intervention in the reconstructive armamentarium for patients with cervical spinal cord injuries, specifically those presenting with C5 or C6 tetraplegia. In the hierarchical loss of upper extremity motor function following a mid-cervical spinal cord injury, the triceps brachii (primarily innervated by the C7 nerve root) is uniformly paralyzed, whereas the deltoid muscle (innervated by the C5 nerve root via the axillary nerve) routinely retains robust, functional contractility. The profound biomechanical deficit resulting from the absence of active elbow extension cannot be overstated; it severely truncates the spatial volume of reach, effectively tethering the patient's functional envelope to a small radius adjacent to the torso. Furthermore, it compromises the patient's ability to perform independent wheelchair transfers, precludes effective weight-shifting maneuvers required for ischial pressure relief, and dramatically escalates the lifelong risk of developing devastating decubitus ulcers.
The epidemiological landscape of spinal cord injuries underscores the critical need for this procedure. Cervical lesions account for over half of all spinal cord injuries, with C5 and C6 representing the most frequently injured neurological levels. These patients often possess intact shoulder control and elbow flexion (via the biceps and brachialis) but are left functionally severely impaired by the unopposed flexion moment at the elbow. Historically, these patients were relegated to a life of complete dependence for mobility and transfers. The advent of upper extremity tendon transfers, pioneered in this specific domain by Erik Moberg in the 1970s, initiated a paradigm shift in tetraplegia management. Moberg recognized that the posterior third of the deltoid could be anatomically decoupled from its humeral insertion and rerouted to serve as a surrogate elbow extensor, fundamentally altering the functional trajectory of these patients.
Since Moberg's original descriptions, the posterior deltoid-to-triceps transfer has undergone significant iterative refinements by prominent upper extremity surgeons, including Hentz, Lacey, and Zancolli. These modifications have primarily focused on optimizing the biomechanical linkage between the donor muscle and the recipient tendon, addressing the frequent requirement for interpositional grafts, and refining postoperative rehabilitation protocols to minimize the catastrophic complication of transfer rupture. Today, this procedure is universally recognized as arguably one of the most profoundly life-altering reconstructive surgeries available to the tetraplegic population, consistently yielding high rates of patient satisfaction and measurable improvements in functional independence measures (FIM).
Beyond the direct restoration of reach and transfer capability, the reconstruction of elbow extension is often a mandatory prerequisite for subsequent, more distal reconstructive procedures. A fundamental tenet of tendon transfer surgery dictates that a joint must be stabilized against antagonistic forces before a transfer crossing that joint can function effectively. For instance, if a surgeon plans to transfer the brachioradialis to the extensor carpi radialis brevis (ECRB) to restore active wrist extension, the elbow must first possess active extension. Without an intact or reconstructed triceps to stabilize the elbow, the contraction of the transferred brachioradialis will simply flex the elbow rather than extending the wrist, rendering the distal transfer functionally impotent. Thus, the posterior deltoid-to-triceps transfer often serves as the foundational cornerstone upon which comprehensive upper extremity reconstruction in the tetraplegic patient is built.
Detailed Surgical Anatomy and Biomechanics
A profound, three-dimensional understanding of the posterior shoulder girdle and brachium is an absolute prerequisite for the safe and effective execution of the posterior deltoid-to-triceps transfer. The deltoid muscle is a massive, multipennate structure traditionally divided into three distinct anatomical and functional segments: the anterior (clavicular), middle (acromial), and posterior (spinal) heads. The posterior deltoid, which serves as the donor muscle for this transfer, originates from the lower lip of the posterior border of the spine of the scapula. Its fibers course inferolaterally to converge with the other segments, inserting via a thick, fibrous aponeurosis into the deltoid tuberosity on the lateral aspect of the mid-humerus. The posterior deltoid acts primarily as an extensor and external rotator of the humerus at the glenohumeral joint. In the tetraplegic patient, harvesting the posterior third of the deltoid does not significantly compromise shoulder stability or function, provided the anterior and middle heads remain intact to facilitate shoulder abduction and forward flexion.
The neurovascular supply to the deltoid is the most critical anatomical consideration during the harvest phase of the procedure. The axillary nerve (comprising fibers from C5 and C6) branches from the posterior cord of the brachial plexus, passes through the quadrangular space accompanied by the posterior circumflex humeral artery, and courses circumferentially around the surgical neck of the humerus. It enters the deltoid muscle on its deep (epimysial) surface. Crucially, the neurovascular bundle enters the posterior deltoid approximately 5 to 7 centimeters distal to the posterolateral corner of the acromion. This anatomical landmark defines the "danger zone" of the proximal dissection. When splitting the posterior third of the deltoid from the middle third, the surgeon must meticulously identify this neurovascular hilum. Any proximal dissection extending beyond this hilum risks catastrophic iatrogenic denervation of the transfer, rendering the procedure completely ineffective and further devastating the patient's already compromised upper extremity function.
The recipient anatomy involves the triceps brachii, a three-headed muscle (long, lateral, and medial heads) that converges into a broad, dense aponeurosis inserting onto the proximal surface of the olecranon process of the ulna. In the C5/C6 tetraplegic patient, the triceps muscle belly is profoundly atrophied and fibrotic due to lower motor neuron denervation or upper motor neuron disuse. However, the triceps aponeurosis and its robust insertion into the olecranon remain structurally intact and serve as an excellent anchoring point for the distal fixation of the transfer. The biomechanical goal of the surgery is to establish a direct, linear line of pull from the posterior scapular spine to the olecranon, effectively bypassing the paralyzed triceps muscle belly while utilizing its distal tendinous footprint.
Biomechanically, the posterior deltoid is uniquely suited for this transfer due to its substantial physiological cross-sectional area and excellent excursion capabilities. A successful tendon transfer requires the donor muscle to possess sufficient excursion (amplitude of contraction) to move the joint through its functional range of motion, and sufficient force generation to overcome both gravity and soft tissue resistance. The posterior deltoid possesses an excursion of approximately 5 to 7 centimeters, which closely matches the physiological requirement for full elbow extension. Furthermore, by routing the transfer directly over the posterior aspect of the humerus, the surgeon maximizes the moment arm of the new extensor mechanism relative to the axis of rotation of the elbow joint. This optimized moment arm is critical for generating the torque required for the patient to lift their body weight during independent wheelchair transfers.
Exhaustive Indications and Contraindications
The decision to proceed with a posterior deltoid-to-triceps transfer requires meticulous patient selection, balancing profound anatomical deficits with the patient's psychological resilience and rehabilitative potential. The ideal surgical candidate is a patient with a stable C5 or C6 spinal cord injury who presents with a complete or near-complete loss of active elbow extension (Medical Research Council [MRC] Grade 0 or 1 triceps strength). Concurrently, the patient must possess a robust, fully innervated posterior deltoid muscle, demonstrating MRC Grade 4 or 5 strength. This is a critical biomechanical prerequisite; because a muscle typically loses approximately one full grade of strength following transposition due to altered resting length and vector mechanics, a donor muscle starting at Grade 3 will predictably fail to provide clinically useful extension against gravity postoperatively.
Furthermore, the physical examination must confirm a perfectly supple elbow joint. The presence of a fixed flexion contracture of the elbow is an absolute contraindication to isolated tendon transfer. The transferred deltoid, even under optimal conditions, cannot overcome established capsular or ligamentous contractures. If a flexion contracture is present, it must be aggressively addressed preoperatively through serial casting, dynamic splinting, or, if recalcitrant, concurrent surgical anterior capsular release. Additionally, the surgeon must evaluate the synergistic and antagonistic musculature of the upper extremity. As previously noted, if a brachioradialis-to-ECRB transfer is planned for wrist extension, the brachioradialis itself must possess at least Grade 4 strength, evaluated by palpating the muscle belly against resisted elbow flexion with the forearm in neutral rotation.
Psychological and social factors are equally paramount in the determination of surgical candidacy. The postoperative rehabilitation protocol following a deltoid-to-triceps transfer is notoriously arduous, requiring months of strict compliance, prolonged immobilization, and a temporary but significant reduction in the patient's baseline functional independence. Patients must possess the cognitive capacity to understand these limitations and the psychological fortitude to endure the protracted recovery. A robust social support system is mandatory, as the patient will require maximal assistance for daily activities, transfers, and pressure relief during the initial 12-week postoperative period when weight-bearing through the operated extremity is strictly prohibited.
Contraindications must be rigorously respected to prevent surgical failure and the exacerbation of disability. Severe, medically refractory spasticity in the elbow flexors (biceps/brachialis) represents a profound contraindication, as the transferred deltoid will be rapidly overpowered and stretched out by the spastic antagonists. In such cases, optimization with oral antispasmodics, targeted botulinum toxin injections, or surgical lengthening of the flexor tendons must precede any consideration of extensor reconstruction. Similarly, severe heterotopic ossification (HO) bridging the elbow joint, a known complication following severe CNS trauma, must be fully mature and surgically excised prior to tendon transfer.
Indications and Contraindications Matrix
| Parameter | Favorable Indications (Proceed with Surgery) | Absolute/Relative Contraindications (Do Not Proceed) |
|---|---|---|
| Neurological Level | Stable C5 or C6 Tetraplegia | Progressive neurological disease; High cervical (C1-C4) |
| Donor Muscle Strength | Posterior Deltoid MRC Grade 4 or 5 | Posterior Deltoid MRC Grade < 4 |
| Recipient Muscle Status | Triceps MRC Grade 0 or 1 | Triceps MRC Grade > 2 (Consider conservative rehab) |
| Joint Mobility | Full, unrestricted passive ROM of elbow | Fixed flexion contracture > 15 degrees |
| Spasticity | Modified Ashworth Scale 0 to 1 | Modified Ashworth Scale > 2 in elbow flexors |
| Cognitive/Social | Highly motivated, excellent support system | Poor compliance, lack of caregiver support |
| Local Tissue Health | Supple skin, absent pressure sores | Active decubitus ulcers, severe heterotopic ossification |
Pre-Operative Planning, Templating, and Patient Positioning
Preoperative planning for the posterior deltoid-to-triceps transfer is distinct from traditional orthopedic bony procedures; it relies heavily on meticulous clinical examination rather than radiographic templating. The cornerstone of preparation is a rigorous manual muscle testing (MMT) session, mapped meticulously to document the exact motor grade of every functional muscle unit in the upper extremity. This mapping dictates not only the viability of the deltoid transfer but also the sequencing of concurrent or future reconstructive procedures (e.g., Zancolli biceps rerouting, brachioradialis transfers, or intrinsic hand reconstructions). While standard orthogonal radiographs of the elbow and shoulder are obtained to rule out occult fractures, joint subluxations, or heterotopic ossification, advanced imaging such as MRI or high-resolution ultrasound is occasionally utilized in borderline cases to assess the cross-sectional area and fatty infiltration of the donor posterior deltoid.
A critical component of preoperative planning involves the selection of the interpositional graft, should direct coaptation of the deltoid to the triceps aponeurosis prove impossible due to inadequate length. The surgeon must consent the patient for potential donor sites, discussing the specific morbidities associated with each. The fascia lata is frequently preferred due to its broad, robust sheet-like structure, which allows for a multi-point, tension-dispersing weave into both the deltoid and the triceps. Alternatively, tubularized tendon grafts such as the tibialis anterior or the extensor hallucis longus (EHL) may be selected. The choice of graft dictates the necessity for secondary surgical prep sites and fundamentally alters the intraoperative workflow.
Patient positioning is a highly orchestrated process designed to maximize surgical exposure while rigorously protecting the insensate patient from iatrogenic positioning injuries. The patient is placed in the lateral decubitus position, with the operative extremity facing upward. This position provides simultaneous, unhindered access to the posterior shoulder, the entire brachium, and the posterior elbow. An axillary roll is meticulously placed to protect the dependent brachial plexus, and all bony prominences (greater trochanter, fibular head, lateral malleolus) are aggressively padded with gel mats and foam. Given the patient's insensate status and inherent vulnerability to pressure necrosis, the positioning phase often takes as long as the initial surgical dissection.
The operative arm is draped free to allow for full, unrestricted manipulation of the shoulder and elbow throughout the procedure. This mobility is essential for accurately assessing the tension of the transfer during the final fixation phase. A sterile pneumatic tourniquet is routinely applied high on the proximal arm; however, it is frequently left un-inflated unless brisk, uncontrollable bleeding is encountered. The proximal extent of the deltoid dissection often crosses the distal edge of the tourniquet, making its inflation impractical for the entirety of the case. The surgical team must rely on meticulous hemostasis using bipolar electrocautery and precise anatomical dissection to maintain a clear operative field.
Step-by-Step Surgical Approach and Fixation Technique
Incision and Deltoid Harvest
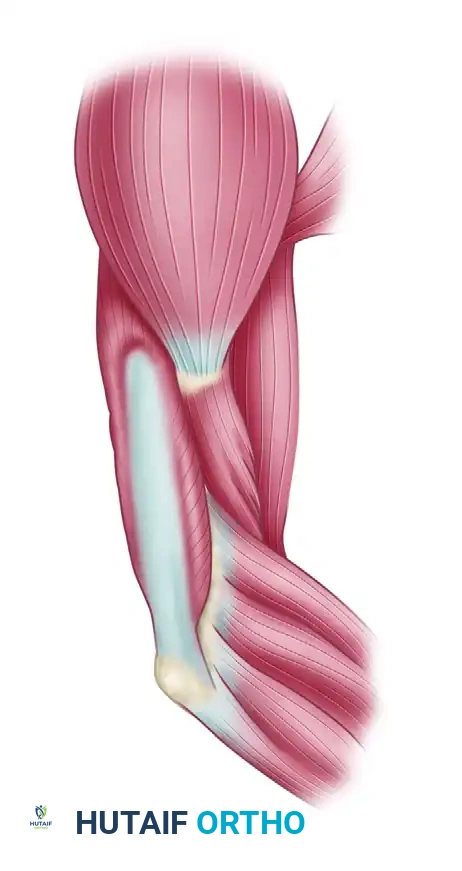
The procedure commences with a 10- to 13-centimeter longitudinal incision centered over the posterior border of the deltoid muscle. The incision extends distally to the palpable insertion of the muscle at the deltoid tuberosity of the lateral humerus. The surgeon meticulously raises thick fasciocutaneous flaps, preserving the subdermal vascular plexus to prevent marginal skin necrosis, a disastrous complication in the tetraplegic patient. The deep fascia over the deltoid is incised, exposing the robust muscle belly of the posterior third.
Using a combination of sharp dissection and a periosteal elevator, the insertion of the posterior deltoid is elevated from the humerus. It is an absolute surgical imperative to harvest a thick, continuous strip of the periosteal insertion along with the tendinous tissue. This periosteal sleeve provides the critical structural integrity necessary to hold the heavy, non-absorbable sutures used in the subsequent weave. Harvesting pure muscle belly without this tendinous/periosteal extension will inevitably result in suture pull-out and catastrophic failure of the transfer under load.
Figure 1: The posterior border of the deltoid muscle belly is isolated. The surgeon must preserve as much of the tendinous and periosteal insertion as possible to facilitate secure distal fixation.
Once the distal insertion is liberated, the mobilized posterior third of the deltoid is placed under gentle distal traction. The surgeon begins to longitudinally split the muscle fibers, separating the posterior third from the middle third in a distal-to-proximal direction. This is the most dangerous phase of the dissection. The surgeon must continuously palpate and visually inspect the deep (epimysial) surface of the muscle. The dissection must halt immediately upon the identification of the axillary nerve and the posterior circumflex humeral vessels, which typically enter the deep surface of the muscle 5 to 7 centimeters distal to the acromion. Violation of this neurovascular hilum results in irreversible denervation.
Triceps and Olecranon Exposure
Attention is then directed to the elbow. A separate, gently curved longitudinal incision is made over the posterior aspect of the distal humerus and proximal ulna. To avoid placing a surgical scar directly over the weight-bearing bony prominence of the olecranon—which could lead to painful neuromas or skin breakdown during wheelchair use—the incision is biased slightly medial or lateral to the midline. The subcutaneous tissues are divided to expose the broad, glistening expanse of the distal triceps aponeurosis and its firm insertion into the olecranon. In these patients, the underlying triceps muscle belly is universally atrophied, pale, and fibrotic, starkly contrasting with the healthy, vascularized donor deltoid muscle.
Graft Interposition and Tendon Weave
The surgeon must now bridge the gap between the mobilized posterior deltoid and the triceps aponeurosis. If the patient possesses exceptional anatomical length, a direct transfer (Scenario A) may be possible. However, in the vast majority of cases, an interpositional graft (Scenario B) is required to achieve a tension-free, mechanically sound repair.
If a tubularized tendon graft (such as the tibialis anterior) is utilized, a classic Pulvertaft weave is employed. The graft is laced through the distal end of the posterior deltoid proximally, utilizing multiple perpendicular passes to maximize the surface area for biological healing. The distal end of the graft is similarly woven into the robust triceps aponeurosis.
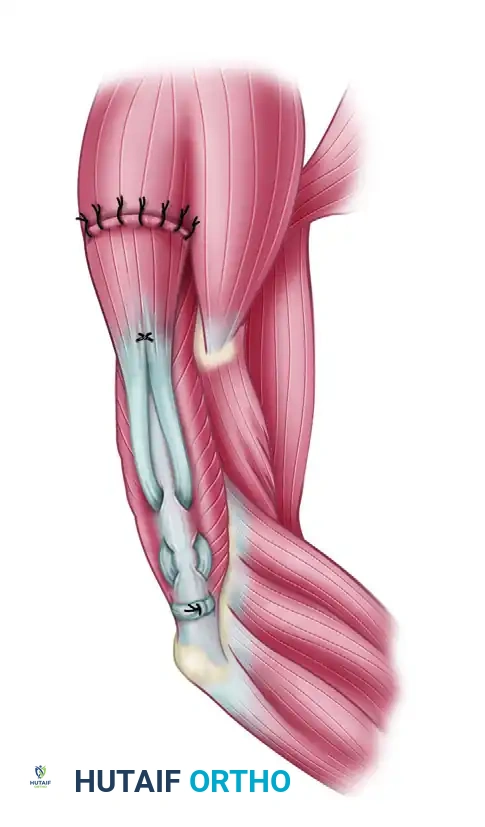
Figure 2: Tendon grafts are laced into the distal end of the posterior deltoid muscle belly proximally and woven into the triceps aponeurosis distally using a Pulvertaft weave technique.
Alternatively, if a fascia lata graft is selected, its broad, sheet-like morphology allows the surgeon to wrap the distal deltoid in a fascial sleeve, securing it with multiple mattress sutures. Distally, the broad fascial sheet is splayed over the triceps aponeurosis, allowing for excellent distribution of tension across the atrophied recipient bed.
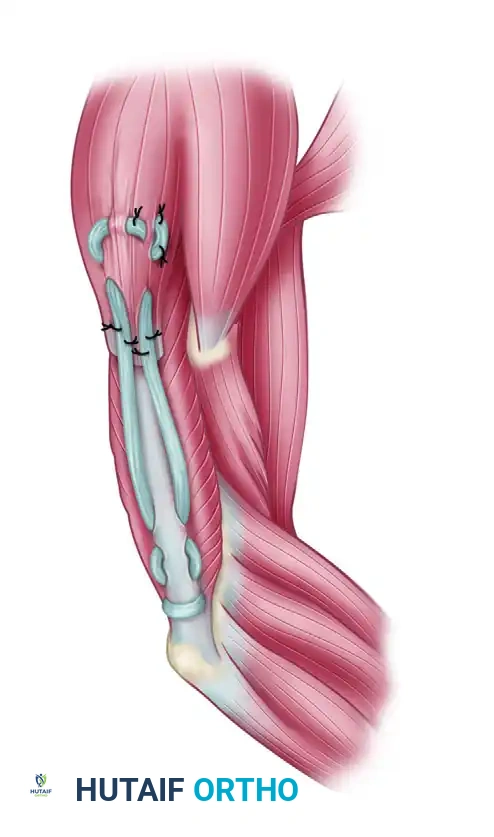
Figure 3: Fascia lata can be used instead of tubular tendon grafts. The broad fascial sheet allows for excellent distribution of tension across the atrophied triceps aponeurosis.
In cases where the triceps aponeurosis is deemed too tenuous to support a robust weave, or if maximum mechanical rigidity is desired, the graft can be routed directly into the olecranon via transosseous drill holes. This bone-to-tendon healing construct provides exceptional ultimate tensile strength, though it requires meticulous protection during the initial 6-week healing phase.
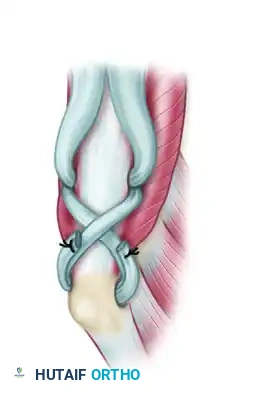
Figure 4: Direct insertion into the olecranon through a transosseous bone tunnel can also be performed with either type of graft, providing rigid bone-to-tendon healing.
Tensioning and Fixation
Setting the optimal tension of the transfer is an art form requiring extensive surgical experience. The arm is positioned with the shoulder in neutral and the elbow extended. The graft is pulled distally to eliminate all slack. The surgeon then assesses the tension by passively flexing the elbow. The "Goldilocks" tension is achieved when full passive elbow flexion can still be obtained on the operating table, but it requires palpable, elastic resistance from the newly constructed extensor mechanism. If the elbow easily falls into flexion, the transfer is under-tensioned and will result in a debilitating extensor lag. Conversely, if the elbow cannot be passively flexed beyond 90 degrees without extreme force, the transfer is over-tensioned, inevitably leading to a permanent flexion contracture.
Once the ideal tension is established, the weave is rigidly secured using multiple passes of heavy, non-absorbable braided suture (e.g., #0 or #2-0 FiberWire or Ethibond). As a final, critical step, small stainless steel surgical clips or radiopaque markers are sutured to the graft and the recipient tendon precisely at the junction sites. These markers serve as an invaluable postoperative diagnostic tool; if a transfer rupture is suspected during rehabilitation, a simple radiograph will reveal separation of the markers, confirming structural failure.
Adjunctive Procedures: Zancolli Biceps Rerouting
In a significant subset of C5/C6 tetraplegic patients, the preservation of the C5-innervated biceps brachii, coupled with the paralysis of the C6/C7-innervated pronator teres, results in a devastating, fixed supination deformity of the forearm. This deformity prevents the patient from placing their palm flat on a surface, severely hindering wheelchair propulsion, keyboard use, and independent feeding. When present, this deformity must be addressed concurrently utilizing the Zancolli procedure.
The Zancolli technique involves exposing the distal biceps tendon at its insertion on the radial tuberosity via an anterior antecubital approach.
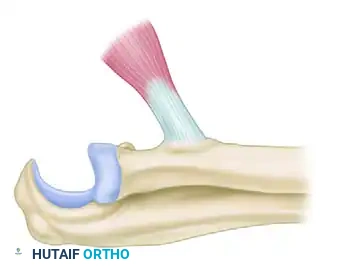
Figure 5: Exposure of the distal biceps tendon at its insertion on the radial tuberosity. The tendon is prepared for detachment.
The tendon is sharply detached from the bone, taking extreme care to protect the adjacent posterior interosseous nerve (PIN) and the brachial artery.
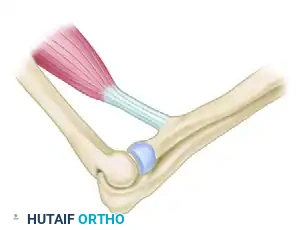
Figure 6: The biceps tendon is detached from the radial tuberosity. Care must be taken to protect the posterior interosseous nerve during deep dissection.
The detached tendon is then physically rerouted around the radial neck. This profound anatomical alteration changes the biomechanical vector of the muscle.
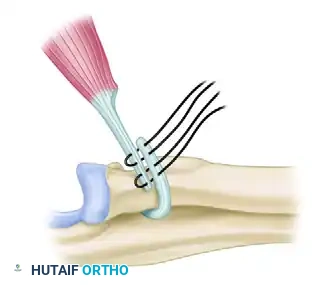
Figure 7: The tendon is rerouted around the radial neck. This alters the vector of pull, converting the muscle into a pronator of the forearm.
By approaching the radius from the opposite direction, the biceps is converted from a primary supinator into an active pronator, while simultaneously preserving its critical function as an elbow flexor. The tendon is then rigidly reattached to the radius using suture anchors or transosseous tunnels. If a severe, chronic contracture is present, an extensive release of the interosseous membrane may be required to permit passive pronation prior to tendon fixation.
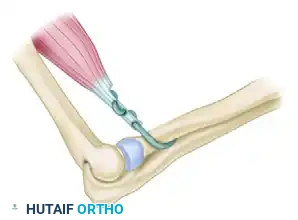
Figure 8: The rerouted biceps tendon is reattached to the radius. Release of the interosseous membrane may be required if severe, chronic contracture prevents passive pronation.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, the posterior deltoid-to-triceps transfer is fraught with potential complications, primarily due to the massive biomechanical forces the reconstructed tendon must eventually endure and the inherent vulnerabilities of the tetraplegic patient population. The most devastating complication is the acute rupture of the transfer. This typically occurs not from a failure of the suture material, but from the graft pulling through the atrophic recipient tissue or from a catastrophic failure of patient compliance (e.g., an accidental early weight-bearing event during a wheelchair transfer). Ruptures are clinically suspected when a patient presents with a sudden, complete loss of previously achieved active extension, often accompanied by a palpable defect. Radiographic evaluation of the intraoperatively placed metallic markers provides definitive confirmation.
Extensor lag and flexion contractures represent the two sides of the tensioning error spectrum. An extensor lag occurs when the transfer is under-tensioned intraoperatively, or when the interpositional graft undergoes gradual, plastic deformation (stretching) during the biological remodeling phase. While a mild lag (10-15 degrees) is often well-tolerated and functional, a severe lag negates the purpose of the surgery. Conversely, a flexion contracture results from profound over-tensioning or, more commonly, a failure of the patient to strictly adhere to the postoperative night-splinting protocol. A severe flexion contracture severely impairs reach and may require secondary surgical release.
Iatrogenic neurological injury, specifically to the axillary nerve during the proximal deltoid dissection, is a rare but catastrophic event. Denervation of the posterior deltoid not only guarantees the failure of the triceps reconstruction but also further weakens the patient's already compromised shoulder girdle, potentially rendering them entirely dependent for all ADLs. Strict adherence to the 5-7 cm "danger zone" rule is the only reliable method of prevention. Infection and wound breakdown are also significant concerns, given the poor vascular tone and insensate skin of the SCI patient. Meticulous soft tissue handling and the avoidance of incisions directly over bony prominences are critical mitigating strategies.
Complications and Salvage Strategies Table
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Transfer Rupture | 5% - 10% | Premature weight-bearing, aggressive passive flexion, poor tissue quality | Urgent surgical exploration, revision grafting, extended immobilization |
| Extensor Lag (>20°) | 15% - 25% | Under-tensioning, graft stretching, inadequate rehab | Intensive active ROM therapy; rarely requires surgical plication |
| Flexion Contracture | 10% - 20% | Over-tensioning, failure of night splinting compliance | Aggressive dynamic splinting, serial casting; surgical release if >30° |
| Axillary Nerve Injury | < 1% | Proximal dissection beyond neurovascular hilum | Irreversible. Consider alternative salvage transfers (e.g., Biceps-to-Triceps) if feasible |
| Wound Dehiscence/Infection | 3% - 5% | Inc |
