Advanced Operative Management of Shoulder and Elbow Pathology

Key Takeaway
Mastering shoulder and elbow pathology requires a profound understanding of biomechanics, precise clinical examination, and evidence-based surgical intervention. This comprehensive guide details the anatomical foundations, provocative testing, and step-by-step operative techniques for rotator cuff tears, impingement syndromes, and elbow tendinopathies. Designed for orthopedic residents and consultants, it provides critical surgical pearls and postoperative protocols to optimize patient outcomes and joint stability.
Comprehensive Introduction and Patho-Epidemiology
The diagnosis and operative management of shoulder and elbow pathology demand a rigorous understanding of pathoanatomy, advanced physical examination methodologies, and high-resolution radiographic imaging. Knowledge of the normal anatomy and biomechanics of the upper extremity provides the essential foundation for the evaluation and surgical treatment of these complex joint disorders. Over the past three decades, the transition from open surgical approaches to advanced arthroscopic and minimally invasive techniques has revolutionized the management of upper extremity pathology, drastically reducing perioperative morbidity while demanding a steeper technical learning curve from the orthopedic surgeon.
Shoulder and elbow disorders represent a massive epidemiological burden in both the general population and the high-demand athletic cohort. Rotator cuff disease alone is one of the most prevalent musculoskeletal conditions, with histological evidence of degeneration beginning as early as the third decade of life. Cadaveric and high-resolution magnetic resonance imaging (MRI) studies have demonstrated that the prevalence of full-thickness rotator cuff tears increases exponentially with age, affecting over 25% of individuals in their sixties and exceeding 50% in those over the age of eighty. Despite this high prevalence, a significant proportion of these tears remain asymptomatic, highlighting the complex interplay between structural failure, kinematic compensation, and nociceptive pain pathways that the treating surgeon must navigate.
In the younger, athletic population, glenohumeral instability and elbow ligamentous injuries predominate. Anterior shoulder instability occurs with an incidence of approximately 1.5 to 1.7 per 1,000 person-years, with recurrence rates approaching 90% in patients under the age of twenty who are managed non-operatively. Similarly, the overhead throwing athlete places supraphysiologic valgus stress across the medial elbow, precipitating microtraumatic failure of the ulnar collateral ligament (UCL). The exponential rise in UCL reconstructions over the past two decades underscores the necessity for a profound understanding of elbow biomechanics and the precise execution of reconstructive techniques.
The contemporary orthopedic surgeon must approach these pathologies not merely as isolated structural defects, but as disruptions in a complex, dynamic biomechanical chain. The successful operative management of these disorders requires a nuanced appreciation of the systemic factors influencing tissue healing, the biomechanical forces acting across the joint, and the precise anatomical footprint restoration required to optimize functional outcomes. This chapter provides an exhaustive, highly technical analysis of the advanced operative management of shoulder and elbow pathology, serving as a definitive reference for the orthopedic surgeon.
Detailed Surgical Anatomy and Biomechanics
Glenohumeral Articular Geometry and the Stability-Mobility Paradox
The shoulder joint complex is composed of four distinct articulations—the sternoclavicular, acromioclavicular, glenohumeral, and scapulothoracic joints—that function synergistically to allow smooth, coordinated upper extremity kinematics. Together, they afford the shoulder the greatest range of motion of any joint in the human body. Normal function relies on a delicate, dynamic balance between mobility and stability, often referred to as the stability-mobility paradox. Mobility is facilitated by the “large ball–small socket” osseous architecture and the voluminous, redundant glenohumeral joint capsule, which remains lax until the extremes of motion are reached. The bony anatomy contributes minimally to intrinsic stability, often compared biomechanically to a "golf ball on a tee."

The glenoid is circumferentially augmented by the labrum, a dense fibrocartilaginous ring that increases the depth of the socket by 50% around the humeral head, significantly enhancing stability through the concavity-compression mechanism. The glenoid articular surface and the labrum combine to create a concavity that is approximately 9 mm deep in the superoinferior plane and 5 mm deep in the anteroposterior plane. Saha demonstrated that the addition of the glenoid labrum increases the effective glenoid articular surface to 75% of the humeral head vertically and 57% horizontally. Furthermore, biomechanical testing by Karzel et al. on cadaveric specimens revealed that the labrum critically dictates the distribution of contact stresses when a compressive load is applied at 90 degrees of abduction; loss of the labrum drastically increases focal articular contact pressures, predisposing the joint to early chondrolysis.
The osseous version of the glenoid also plays a critical role in stability. Normal glenoid version is typically retroverted by 1 to 2 degrees relative to the scapular body, though variations up to 7 degrees are considered within normal physiological limits. Dysplastic alterations in glenoid version, such as excessive retroversion seen in posterior instability or primary glenohumeral osteoarthritis (Walch B2/B3 morphology), drastically alter the joint reaction forces. The surgeon must meticulously evaluate these geometric parameters using 3D computed tomography (CT) to accurately plan corrective osteotomies, bone grafting, or arthroplasty component positioning.
Static and Dynamic Capsuloligamentous Constraints
Because osseous constraint is minimal, stability is primarily conferred by the surrounding capsuloligamentous structures and dynamic musculature. The ligamentous constraints act as the primary static stabilizers at the extremes of motion. The Superior Glenohumeral Ligament (SGHL) serves as the primary restraint to inferior humeral subluxation at 0 degrees of abduction. According to O’Brien et al., it is also the primary stabilizer against anterior and posterior stress at 0 degrees. The Middle Glenohumeral Ligament (MGHL) limits external rotation when the arm is in the lower and middle ranges of abduction but provides negligible restraint at 90 degrees of abduction. It exhibits significant anatomical variability, occasionally presenting as a thickened, cord-like structure (Buford complex) with an absent anterosuperior labrum—a critical normal variant that must not be erroneously "repaired" during arthroscopy.

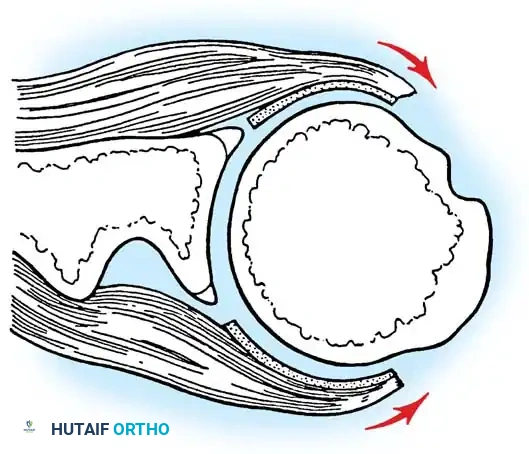
The Inferior Glenohumeral Ligament (IGHL) Complex is the most critical static stabilizer of the shoulder. O’Brien et al. described this as a "hammock-type" structure composed of a thick anterior band, a distinct posterior band, and a thinner intervening axillary pouch. During external rotation in the abducted position, the hammock slides anteriorly and superiorly, tightening the anterior band while the posterior band fans out. The IGHL is the primary stabilizer against anterior and posterior translation when the shoulder is abducted to 45 degrees or more. Pathological elongation or avulsion of the anterior band from the glenoid (Bankart lesion) or the humerus (HAGL lesion) critically compromises this hammock mechanism, leading to recurrent anterior instability.
Dynamic stability is achieved through the coordinated firing of the intrinsic and extrinsic shoulder musculature. These muscular constraints provide stability through three primary mechanisms: dynamic scapular positioning, capsular tensioning, and force couples. Extrinsic muscles position the scapula to maintain the glenoid directly opposite the humeral head during motion; Rowe likened this to a “ball on a seal’s nose.” Concomitant muscle contraction increases the stiffness and torsional rigidity of the ligaments, as rotator cuff and biceps activation actively stiffen the capsule. Finally, as described by Inman, Saunders, and Abbott, intrinsic and extrinsic muscles act as "force couples," directing compressive joint reaction forces concentrically into the glenoid to maintain dynamic stability throughout the arc of motion.
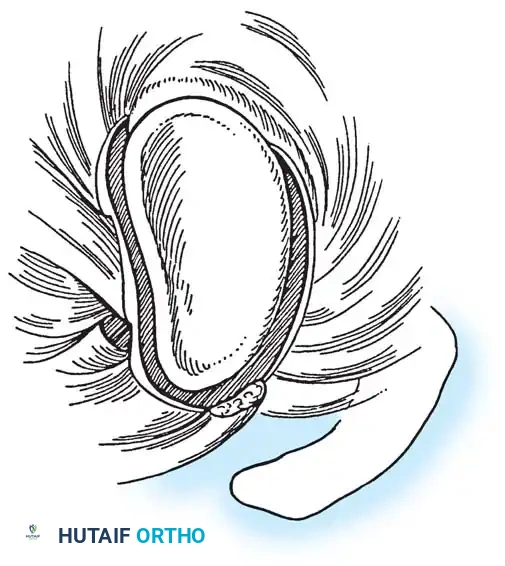
Histological Architecture and the Rotator Cuff Footprint
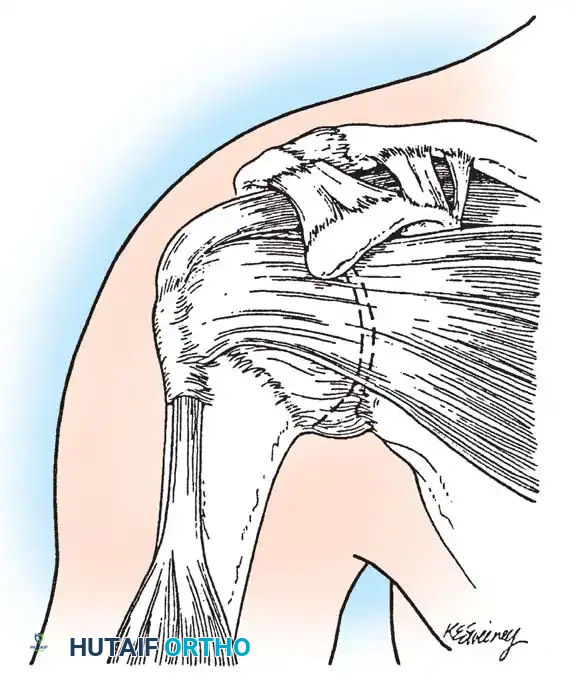
Clark and Harryman detailed the gross and histological anatomy of the rotator cuff, identifying a confluent sheet of tendinous insertions, articular capsule, and ligaments. The supraspinatus and infraspinatus tendons fuse 15 mm proximal to their insertion, functioning as a continuous biomechanical unit rather than isolated structures. Histologically, the supraspinatus and infraspinatus tendons consist of five distinct layers. Layer 1 (1 mm thick) is the superficial layer containing large arterioles and fibers from the coracohumeral ligament. Layer 2 (3–5 mm thick) forms the direct tendinous insertion into the tuberosities, composed of densely packed, parallel collagen bundles. Layer 3 (3 mm thick) consists of smaller collagen bundles forming an interdigitating meshwork at 45-degree angles. Layer 4 contains loose connective tissue, and Layer 5 (2 mm thick) is the true shoulder capsule, an interwoven collagen sheet extending from the labrum to the humerus.
The insertion site at the greater tuberosity is termed the "footprint." Dugas et al. mapped this footprint, noting mean medial-to-lateral insertion widths of 12.7 mm (supraspinatus), 13.4 mm (infraspinatus), 11.4 mm (teres minor), and 17.9 mm (subscapularis). The articular surface-to-tendon insertion distance is less than 1 mm along the anterior 2.1 cm of the supraspinatus-infraspinatus insertion, making this zone highly susceptible to articular-sided partial tears due to intrinsic shear stresses and tensile mismatch between the articular and bursal layers. Understanding this footprint is paramount for modern arthroscopic repair techniques, which aim to maximize the surface area of tendon-to-bone contact to optimize biological healing.
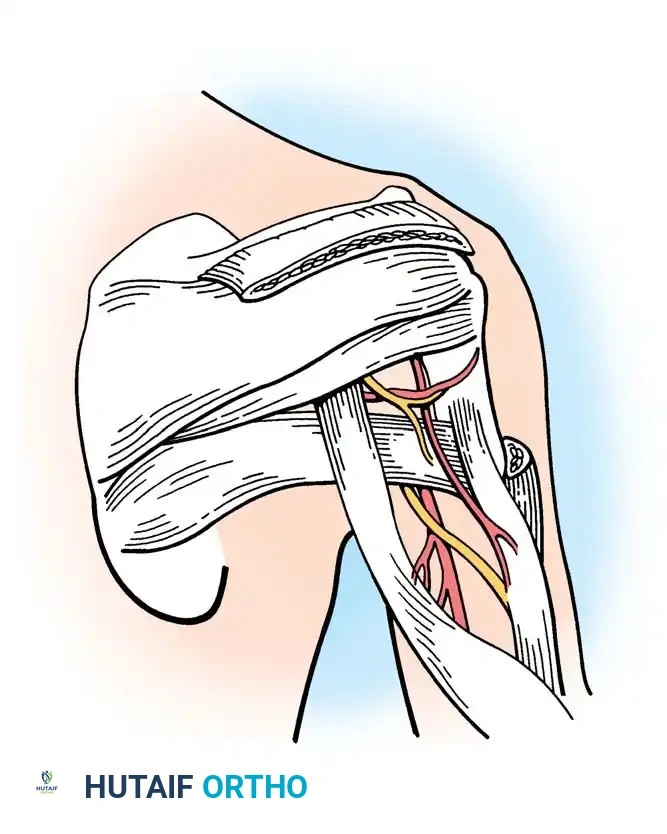
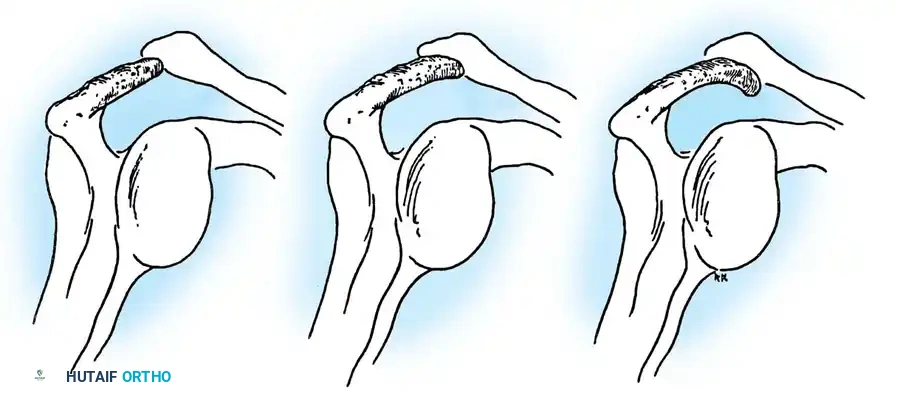
The vascularity of the rotator cuff also plays a pivotal role in its pathoanatomy. The "critical zone" of the supraspinatus tendon, located approximately 1 cm proximal to its insertion, has historically been described as a watershed area of relative hypovascularity. While recent microvascular studies have challenged the absolute avascularity of this region, it remains clear that age-related microvascular attenuation combined with repetitive mechanical impingement beneath the coracoacromial arch precipitates tendon degeneration. The coracoacromial arch forms the rigid roof over the subacromial space; any morphological variant (e.g., Type III hooked acromion) or acquired osteophytosis here critically narrows the space, precipitating mechanical impingement of the underlying bursa and rotator cuff.
Elbow Osseous and Ligamentous Anatomy
The elbow is a highly constrained, complex hinge joint comprising three distinct articulations: the ulnohumeral, radiocapitellar, and proximal radioulnar joints. The osseous architecture provides the primary restraint to varus and valgus stress at extremes of extension, while the ligamentous structures provide the primary restraint at intermediate flexion angles. The ulnohumeral joint is characterized by the highly congruent articulation between the trochlea and the greater sigmoid notch of the ulna. The anterior translation of the distal humerus (approximately 30 degrees) and the corresponding posterior angulation of the proximal ulna allow for maximal flexion before bony impingement occurs.

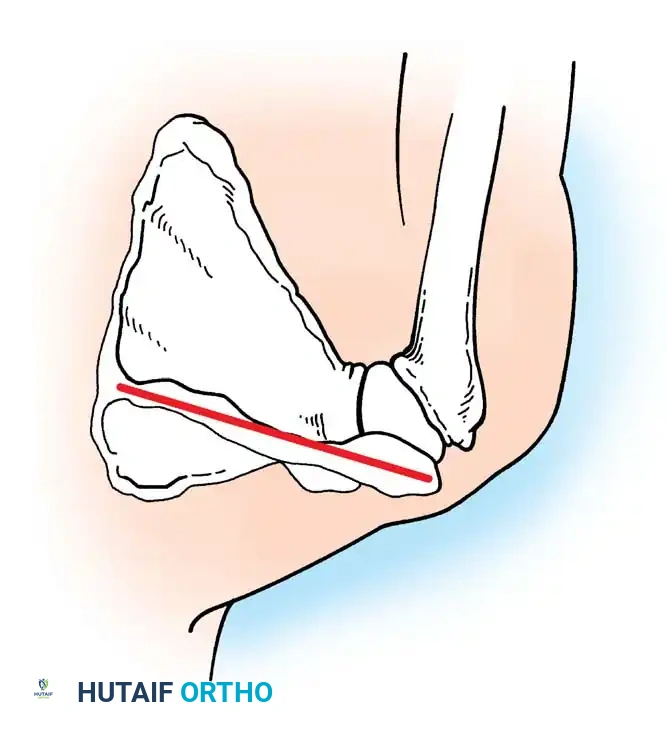
The medial collateral ligament (MCL) complex is the primary restraint to valgus stress. It is composed of the anterior bundle (AMCL), posterior bundle (PMCL), and transverse ligament. The AMCL is the most critical biomechanical structure, originating from the anteroinferior surface of the medial epicondyle and inserting onto the sublime tubercle of the anteromedial coronoid facet. The AMCL is further subdivided into anterior and posterior bands, which exhibit reciprocal tensioning throughout the arc of flexion. The anterior band is taut in extension, while the posterior band becomes taut in deeper flexion. Precise anatomical knowledge of the AMCL footprint is non-negotiable when performing UCL reconstruction in overhead athletes.
The lateral collateral ligament (LCL) complex provides the primary restraint to varus and posterolateral rotatory instability (PLRI). It consists of the lateral radial collateral ligament, the annular ligament, the accessory collateral ligament, and the lateral ulnar collateral ligament (LUCL). The LUCL originates from the lateral epicondyle, blending with the annular ligament, and inserts onto the supinator crest of the ulna. It acts as a critical sling supporting the radial head. Insufficiency of the LUCL, often iatrogenic following overly aggressive lateral epicondylitis debridement or traumatic dislocation, leads to PLRI, characterized by the radial head subluxating posteriorly relative to the capitellum during supination and extension.
Exhaustive Indications and Contraindications
Operative Indications for Glenohumeral Pathology
The decision to proceed with operative intervention in the shoulder demands a rigorous synthesis of the patient's physiological age, functional demands, structural pathology, and response to conservative modalities. For rotator cuff disease, operative intervention is strongly indicated for acute, traumatic full-thickness tears in active individuals, as early repair (within 6 weeks) yields superior biomechanical healing and functional outcomes compared to delayed intervention. In the setting of chronic, degenerative full-thickness tears, surgery is indicated following the failure of 3 to 6 months of comprehensive conservative management, which includes targeted physical therapy focusing on periscapular stabilization, non-steroidal anti-inflammatory drugs (NSAIDs), and judicious subacromial corticosteroid injections.

Massive, retracted rotator cuff tears (>5 cm) present a distinct clinical challenge. Operative repair is indicated provided that irreversible fatty infiltration (Goutallier stage 3 or 4) and severe muscle atrophy (tangent sign positive) have not yet occurred. In patients with pseudoparalysis secondary to massive, irreparable tears, alternative reconstructive options such as superior capsular reconstruction (SCR), lower trapezius tendon transfer, or reverse total shoulder arthroplasty (rTSA) become the indicated procedures, depending on the status of the glenohumeral articular cartilage and the integrity of the deltoid and subscapularis.
For glenohumeral instability, operative stabilization is indicated for recurrent anterior, posterior, or multidirectional instability that fails conservative management. In the young, high-demand collision athlete (e.g., rugby, American football) presenting with a first-time traumatic anterior dislocation, early arthroscopic Bankart repair is increasingly indicated to mitigate the unacceptably high risk of recurrence and subsequent bipolar bone loss. When critical glenoid bone loss exceeds 15-20% of the inferior glenoid diameter, or when an engaging Hill-Sachs lesion is present (off-track lesion), isolated soft-tissue repair is contraindicated, and osseous augmentation via the Latarjet procedure or distal tibial allograft is strictly indicated.
Operative Indications for Elbow Pathology
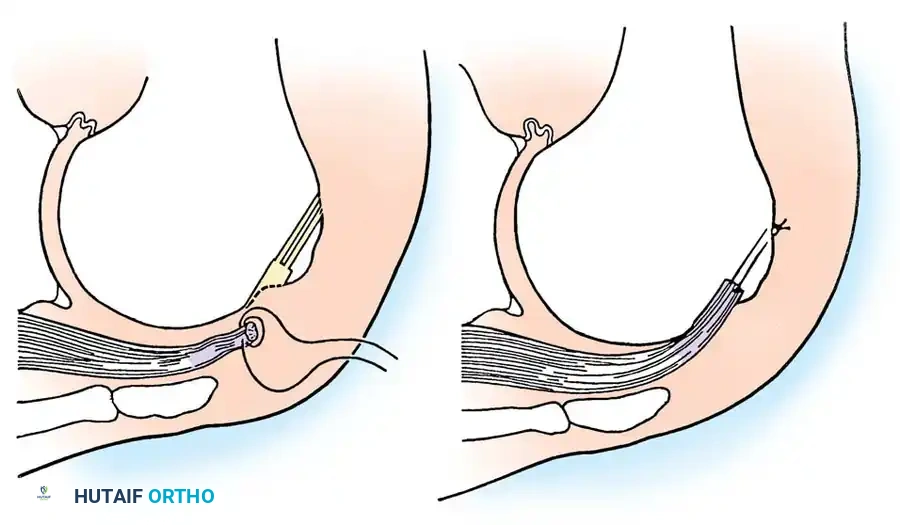
Operative indications for elbow pathology are similarly dictated by the interplay of structural damage and functional demand. In the overhead throwing athlete, surgical reconstruction of the UCL is indicated for symptomatic, MRI-confirmed, full-thickness or high-grade partial tears of the anterior bundle that fail a minimum of 3 months of conservative management (including cessation of throwing, flexor-pronator mass strengthening, and potentially biologic adjuncts like Platelet-Rich Plasma). Acute repair with internal bracing may be indicated in select cases of acute, proximal or distal avulsion injuries in younger athletes, though reconstruction remains the gold standard for mid-substance chronic attenuation.
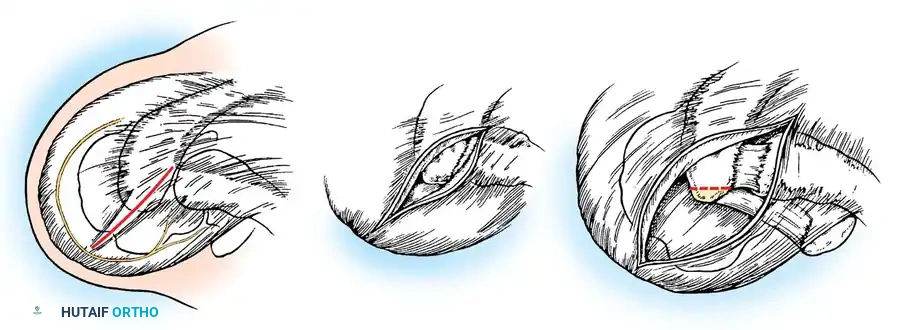
Operative intervention for lateral epicondylitis (tennis elbow) is reserved for recalcitrant cases failing 6 to 12 months of exhaustive non-operative therapy. The surgical indication is the excision of the angiofibroblastic degenerative tissue within the extensor carpi radialis brevis (ECRB) origin, with decortication of the lateral epicondyle to stimulate a healing response. Care must be taken to avoid violating the underlying LUCL to prevent iatrogenic posterolateral rotatory instability.
For post-traumatic elbow stiffness, operative arthrolysis (open or arthroscopic) is indicated when the patient's functional arc of motion is less than 30 to 130 degrees of flexion, and static progressive splinting has plateaued for at least 6 months. The presence of heterotopic ossification (HO) requires a delay in surgical excision until the bone is metabolically mature, typically indicated by normal serum alkaline phosphatase levels and sharply demarcated margins on radiographic imaging, to minimize the risk of catastrophic recurrence.
Absolute and Relative Contraindications
Absolute contraindications for operative management of shoulder and elbow pathology include active local or systemic infection, profound medical comorbidities rendering anesthesia unacceptably high-risk, and the presence of a neuropathic joint (Charcot arthropathy). In the shoulder, a paralyzed deltoid (axillary nerve palsy) is an absolute contraindication for reverse total shoulder arthroplasty, as the deltoid is the primary motor unit required for elevation in the absence of a functioning rotator cuff.
Relative contraindications require careful preoperative optimization and shared decision-making. Active smoking is a profound relative contraindication for rotator cuff repair and ligamentous reconstruction, as nicotine drastically impairs microvascular angiogenesis, significantly increasing the risk of structural failure and non-union at the tendon-bone interface. Severe, unmanaged psychiatric illness or documented non-compliance with postoperative rehabilitation protocols are also strong relative contraindications, as the success of these procedures relies heavily on strict adherence to phased, protective mobilization.
| Pathology / Procedure | Primary Operative Indications | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Arthroscopic Rotator Cuff Repair | Acute traumatic tear; Chronic tear failing >3 mos conservative care; Intact muscle bulk (Goutallier 0-2). | Active joint infection; Neuropathic joint; Advanced glenohumeral osteoarthritis (requires arthroplasty). | Active smoking; Poor compliance; Advanced fatty infiltration (Goutallier 3-4). |
| Arthroscopic Bankart Repair | Recurrent anterior instability; First-time dislocation in young collision athlete; <15% glenoid bone loss. | Critical glenoid bone loss (>20%); Engaging Hill-Sachs lesion (Off-track). | Generalized ligamentous laxity (Ehlers-Danlos); Voluntary dislocators. |
| Latarjet Procedure | Anterior instability with >15-20% glenoid bone loss; Failed prior soft-tissue stabilization; Off-track lesions. | Coracoid hypoplasia; Active infection; Severe subscapularis dysfunction. | Advanced age with low functional demand; Heavy smoking (risk of graft non-union). |
| UCL Reconstruction (Elbow) | Symptomatic AMCL tear in overhead athlete failing conservative care; Chronic valgus instability. | Degenerative joint disease of the elbow; Asymptomatic tears in non-throwers. | Ulnar neuropathy (requires concurrent transposition); Inadequate bone stock. |
| Elbow Arthrolysis/Capsular Release | Functional ROM deficit (<30-130°) failing 6 mos static progressive splinting. | Immature heterotopic ossification; Active intra-articular infection. | Severe articular incongruity; Poor patient motivation for rigorous post-op therapy. |
Pre-Operative Planning, Templating, and Patient Positioning
Advanced Radiographic Imaging and 3D Templating
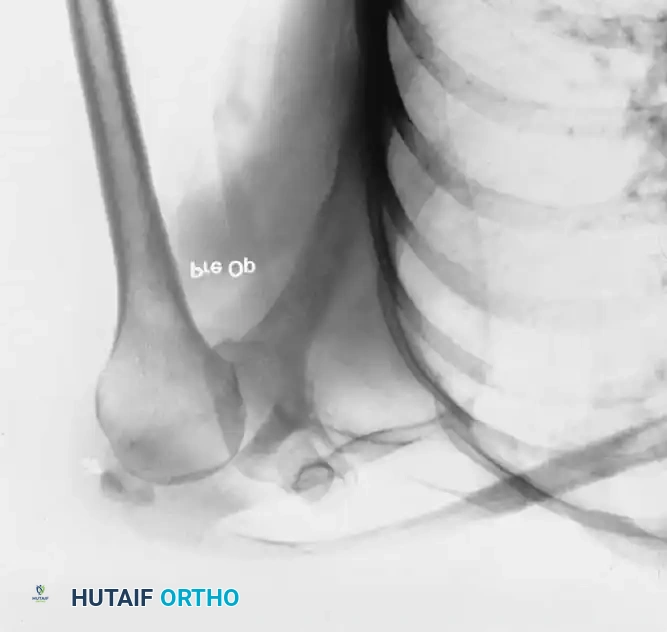
The foundation of successful operative intervention is meticulous preoperative planning utilizing advanced, high-resolution imaging modalities. Standard orthogonal radiographs (true anteroposterior, scapular Y, and axillary lateral views for the shoulder; AP and lateral for the elbow) remain the initial screening tool. However, MRI is the gold standard for evaluating the soft-tissue envelope. For the shoulder, non-contrast MRI is typically sufficient for diagnosing rotator cuff pathology, assessing tear retraction (Patte classification), and evaluating muscle atrophy and fatty infiltration (Goutallier classification) on T1-weighted sagittal oblique sequences.
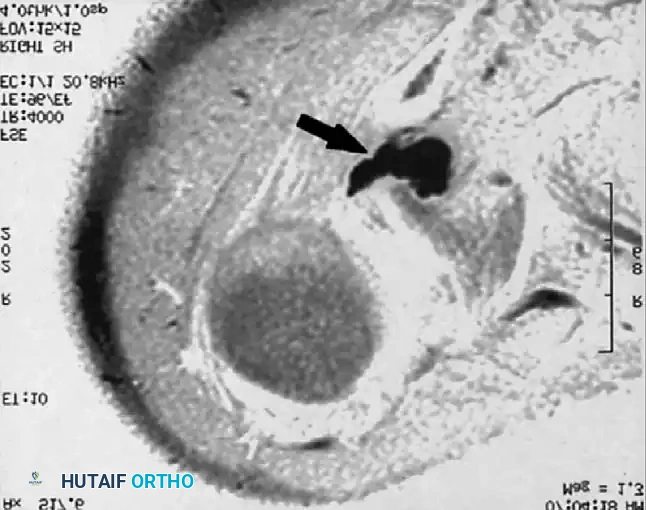
When evaluating glenohumeral instability or superior labral anterior-posterior (SLAP) lesions, MR arthrography (MRA) with intra-articular gadolinium provides superior sensitivity and specificity. The ABER (abduction and external rotation) sequence is particularly critical for placing tension on the IGHL, allowing for the precise identification of subtle anteroinferior labral detachments and articular-sided partial rotator cuff tears (PASTA lesions). For the elbow, MRA is highly sensitive for identifying undersurface tears of the AMCL, commonly seen as the "T-sign" where contrast leaks medial to the sublime tubercle.
In the setting of osseous pathology—such as glenoid bone loss in instability, complex proximal humerus fractures, or advanced osteoarthritis—high-resolution CT scanning with 3D reconstruction is mandatory. Advanced 3D templating software allows the surgeon to digitally subtract the humeral head, calculate the exact percentage of glenoid bone loss using the best-fit circle method, and determine the "on-track" or "off-track" nature of a Hill-Sachs lesion. This digital templating is crucial for determining whether a soft-tissue Bankart repair will suffice or if an osseous augmentation (Latarjet) is required.
Anesthesia and Regional Blockade Considerations
Optimization of the anesthetic plan is vital for minimizing perioperative morbidity, managing postoperative pain, and facilitating early discharge in the ambulatory setting. The current standard of care for advanced shoulder arthroscopy involves a multimodal analgesic approach, heavily relying on regional anesthesia. The interscalene brachial plexus block, administered under direct ultrasound guidance, provides profound analgesia to the shoulder joint and the lateral aspect of the arm. It drastically reduces intraoperative volatile anesthetic requirements, thereby stabilizing hemodynamics and minimizing postoperative nausea and vomiting (PONV).
However, the interscalene block is not without risks. It invariably causes ipsilateral phrenic nerve blockade, resulting in transient hemidiaphragmatic paresis. While well-tolerated in healthy individuals, it is relatively contraindicated in patients with severe chronic obstructive pulmonary disease (COPD) or contralateral diaphragmatic dysfunction. In such cases, a supraclavicular block or a targeted suprascapular and axillary nerve block may be utilized to spare pulmonary function while providing adequate analgesia.
For elbow procedures, a supraclavicular or infraclavicular block is preferred, as the interscalene block frequently spares the ulnar nerve distribution (C8-T1), which is critical for medial-sided elbow surgery. The anesthesiologist and surgeon must coordinate meticulously, especially when intraoperative neuromonitoring or immediate postoperative neurological assessment is required, as dense regional blockade will mask iatrogenic nerve injury until the block resolves.
Patient Positioning: Beach Chair vs Lateral Decubitus
Patient positioning for shoulder surgery is a subject of ongoing debate, with the choice largely dictated by surgeon preference, specific pathology, and the planned procedure. The two primary positions are the Beach Chair (semi-seated) and the Lateral Decubitus position.
The Beach Chair position offers several distinct advantages: it provides an upright, anatomical orientation that is intuitive for the surgeon; it allows for unrestricted manipulation of the arm through a full range of motion, which is critical for assessing dynamic impingement and tensioning rotator cuff repairs; and it facilitates seamless conversion to an open procedure (e.g., deltopectoral approach) if necessary. However, the Beach Chair position carries a significant risk of cerebral hypoperfusion. The anesthesiologist must meticulously monitor mean arterial pressure (MAP), recognizing that the MAP at the level of the brain is significantly lower than at the brachial artery. Hypotensive bradycardic events (Bezold-Jarisch reflex) must be aggressively managed to prevent catastrophic ischemic encephalopathy.
The Lateral Decubitus position involves placing the patient on their non-operative side, with the operative arm suspended in longitudinal and lateral traction (typically 10-15 lbs). This position provides unparalleled, expansive visualization of the glenohumeral joint and the inferior recess, making it the preferred position for complex instability repairs and inferior capsular shifts. The traction opens the subacromial space, facilitating visualization during cuff repairs. The primary drawback is the non-anatomical orientation, which can disorient the novice arthroscopist, and the risk of traction neurapraxia to the brachial plexus if excessive weight is applied or if the procedure is excessively prolonged.
Step-by-Step Surgical Approach and Fixation Technique
Arthroscopic Rotator Cuff Repair: Double-Row Transosseous-Equivalent Technique
The arthroscopic management of a full-thickness rotator cuff tear requires meticulous execution of sequential steps to ensure biomechanical stability and biological healing.
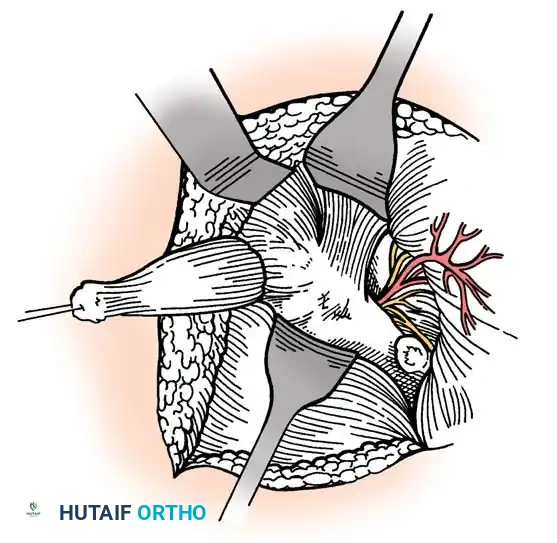
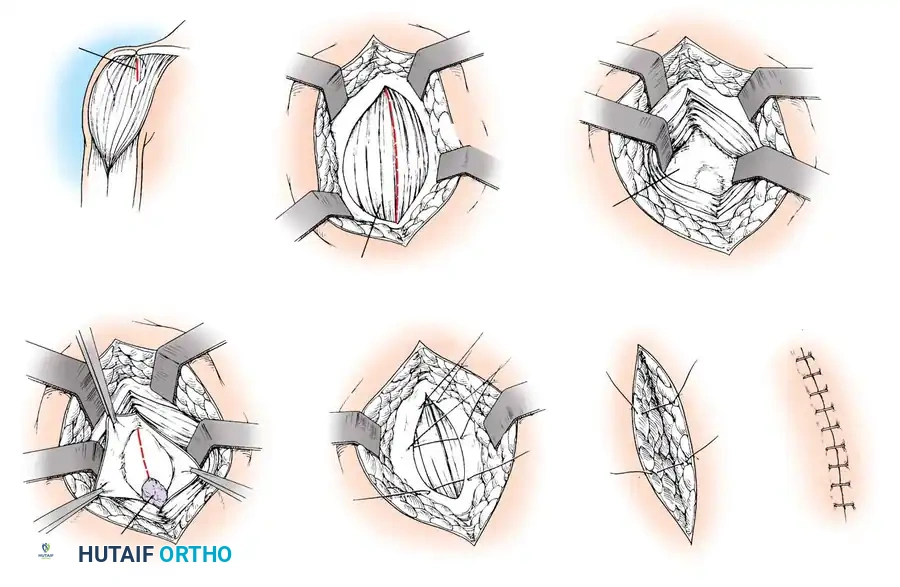
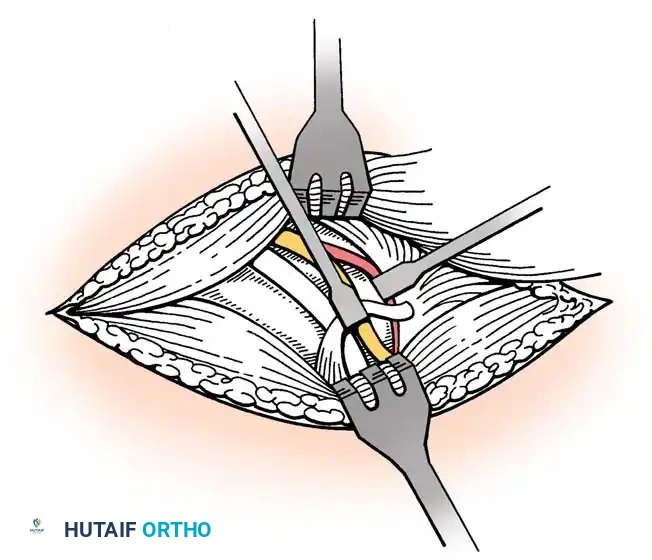
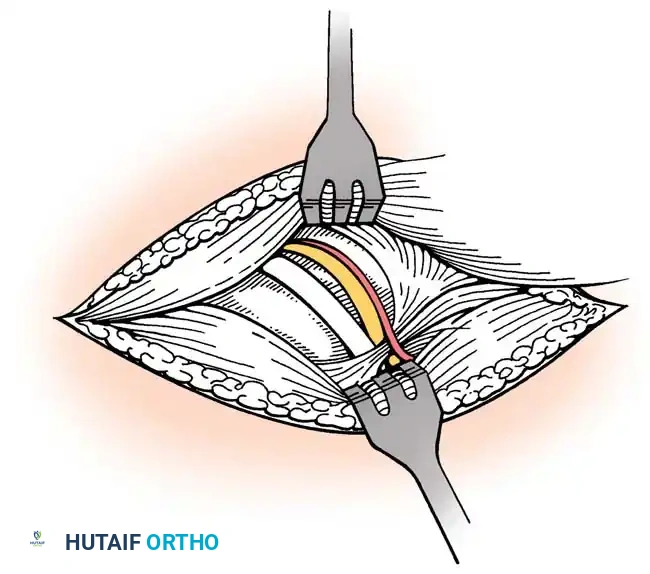
- Diagnostic Arthroscopy and Preparation: A standard posterior viewing portal is established. The glenohumeral joint is systematically inspected for concomitant labral pathology, biceps tendon fraying (which may necessitate tenodesis or tenotomy), and the articular margin of the cuff tear. The arthroscope is then redirected into the subacromial space, and a lateral working portal is established. A motorized shaver and radiofrequency wand are utilized to perform a thorough bursectomy, clearing the subacromial space to visualize the entire bursal surface of the rotator cuff and the coracoacromial arch.
- Acromioplasty and Footprint Preparation: If a Type II or III acromion is present, an acromioplasty is performed using a barrel burr to resect the anteroinferior acromial spur, creating a flat, non-impinging surface. The greater tuberosity footprint is then meticulously debrided of all soft tissue down to a bleeding cortical bed. This decortication releases marrow-derived mesenchymal stem cells and growth factors, optimizing the biological milieu for tendon-to-bone healing.
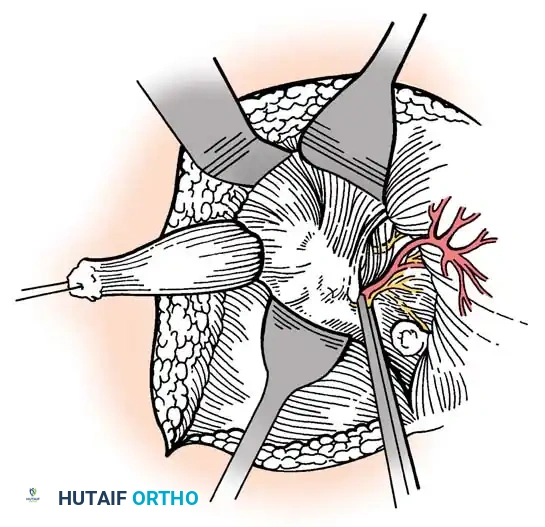
- Tendon Mobilization: The tear pattern (crescent, U-shaped, L-shaped) is identified. If the tendon is retracted, aggressive mobilization is required. This involves releasing capsular adhesions and performing interval slides—the anterior slide between the supraspinatus and subscapularis, and the posterior slide between the supraspinatus and infraspinatus—to allow the tendon to reach the footprint without excessive tension.
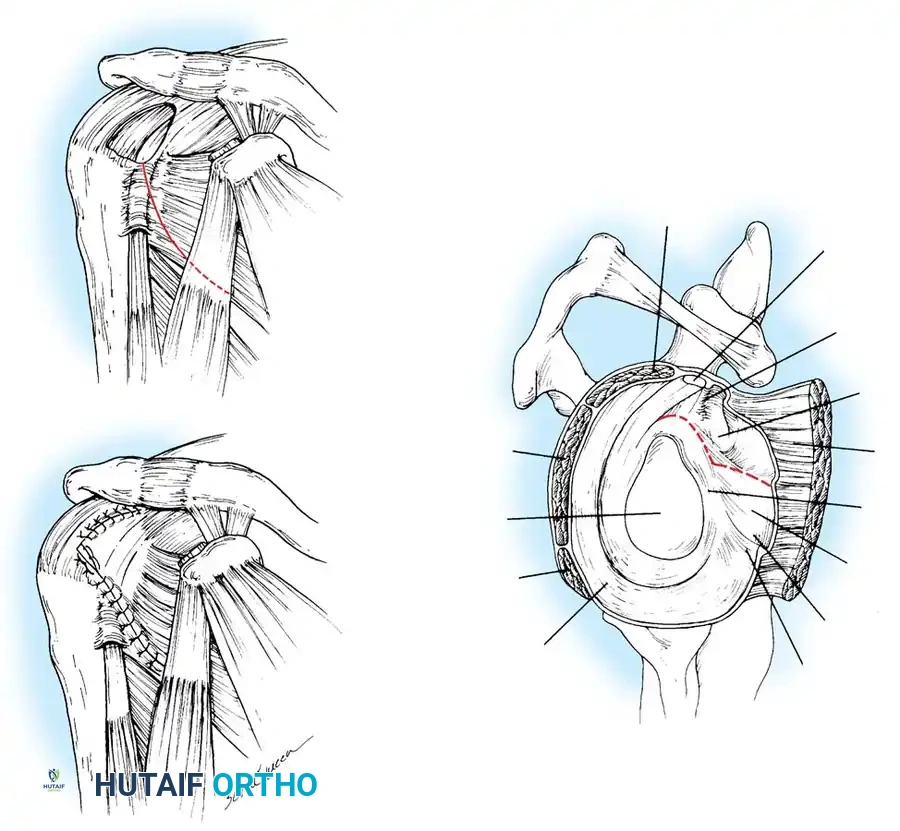
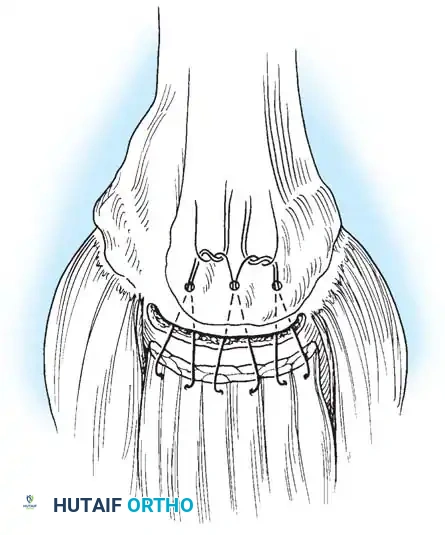
- Anchor Placement and Fixation (Double-Row Transosseous-Equivalent): To maximize the footprint contact area and compression, a double-row, suture-bridge (transosseous-equivalent) technique is employed. First, medial row anchors (biocomposite or PEEK) double-loaded with high-strength suture tape are placed at the articular margin of the footprint. Using a retrograde suture passer, the suture limbs are passed through the musculotendinous junction of the cuff. The medial row is tied using sliding-locking knots. Next, one suture limb from each medial anchor is retrieved laterally, crossed over the bursal surface of the tendon to create a "bridge," and loaded into knotless lateral row anchors. These lateral anchors are impacted into the lateral cortex of the greater tuberosity, tensioning the suture tapes and compressing the tendon flat against the prepared footprint, creating a robust, watertight construct.
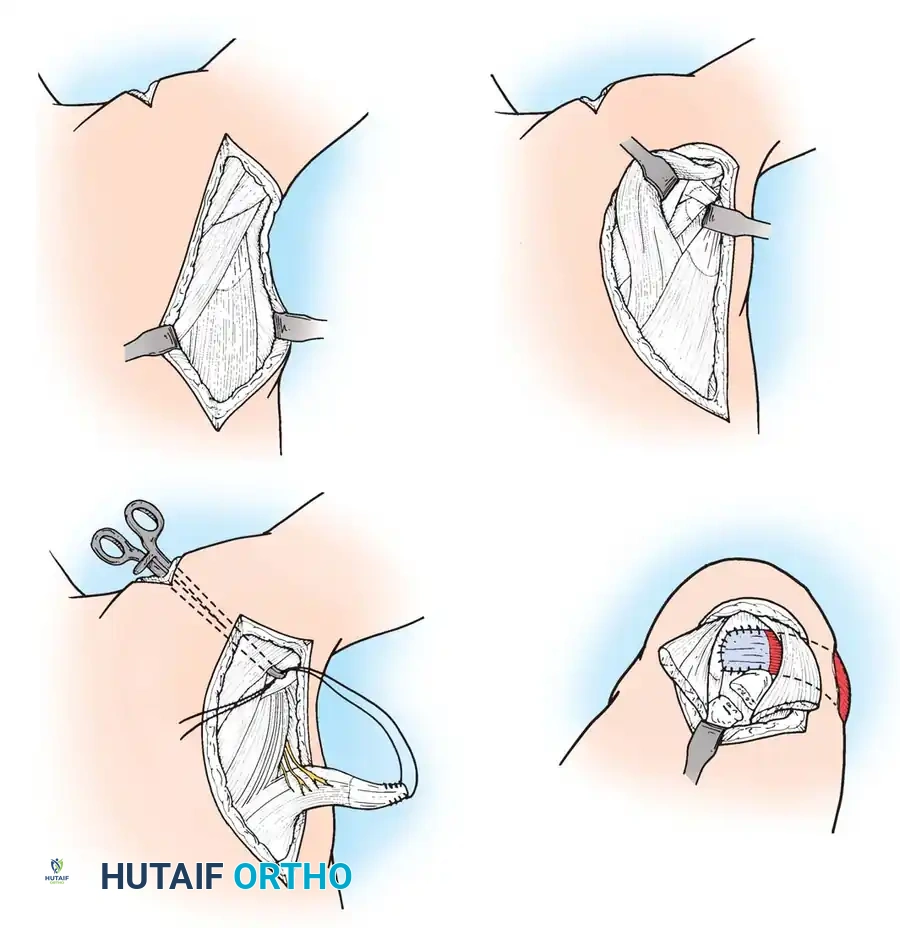
Anterior Glenohumeral Instability: Arthroscopic Bankart and Open Latarjet
For soft-tissue anterior instability without critical bone loss, the Arthroscopic Bankart Repair is the gold standard. Following diagnostic arthroscopy, the anteroinferior labrum and the attached IGHL complex are mobilized from the glenoid neck using an elevator. It is critical to release the tissue inferiorly to the 6 o'clock position to allow for a superior shift. The anterior glenoid neck is decorticated with a burr. Suture anchors (typically 1.5 to 2.9 mm) are placed on the articular margin,
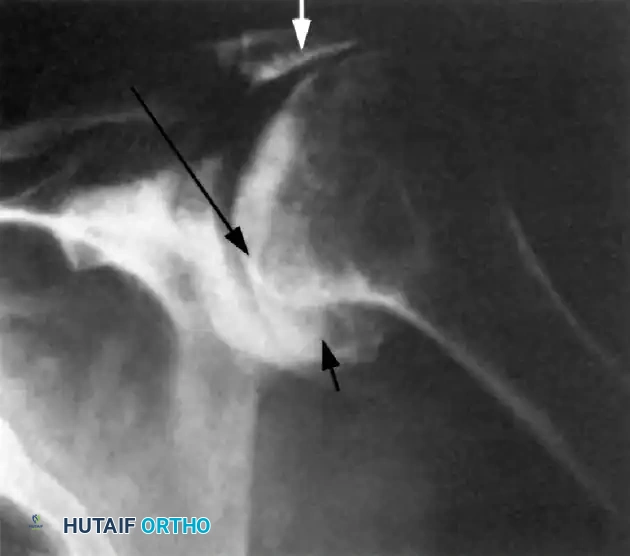
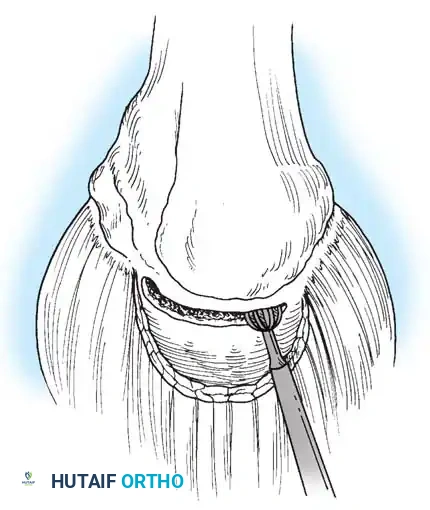
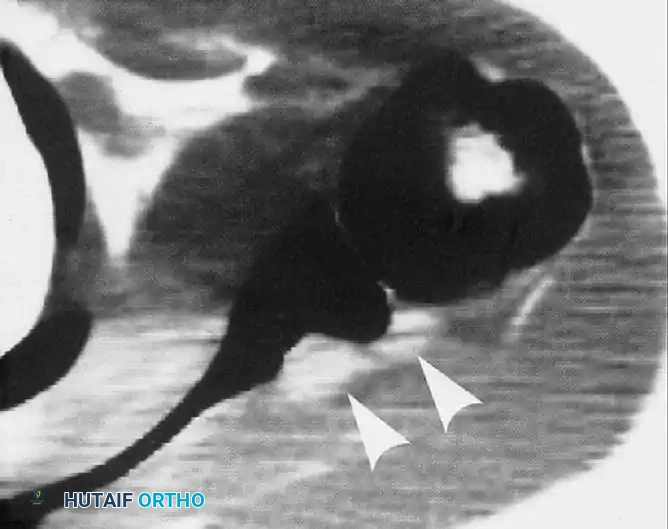
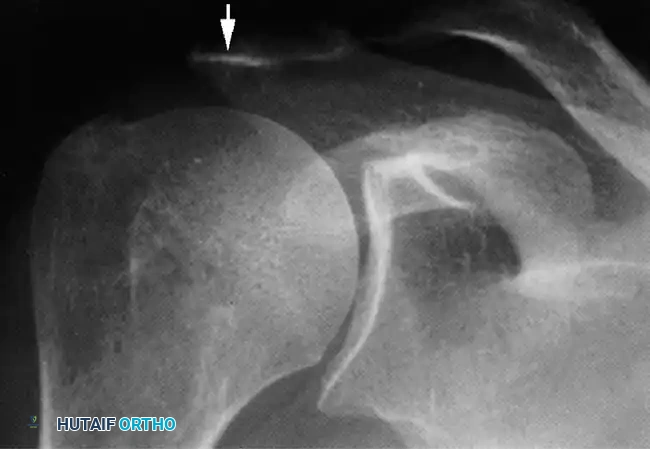
Clinical & Radiographic Imaging Archive