Unmasking Axillary Nerve Palsy in Complex Elbow Trauma: A Case of Missed Shoulder Injury
Key Takeaway
Axillary nerve palsy observed in complex elbow dislocation cases is a critical red flag for co-occurring, often missed, shoulder injuries like surgical neck fractures or glenohumeral dislocations. Thorough neurological assessment of deltoid strength and lateral shoulder sensation is paramount to guide targeted imaging and ensure comprehensive, timely treatment.
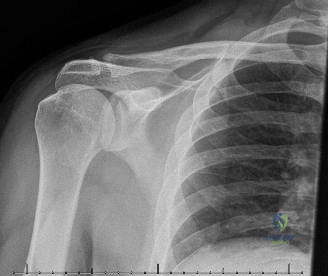
A 58-year-old carpenter presents with a high-energy fall onto an outstretched hand. You are presented with these initial radiographs. Describe your systematic approach to this patient and identify the key clinical concerns.
Candidate: I would perform an ATLS primary and secondary survey to rule out polytrauma. For the extremity, I identify a 'Terrible Triad' of the elbow (posterior dislocation, radial head fracture, and coronoid fracture) and a displaced two-part proximal humerus fracture. I would specifically perform a detailed neurological exam, particularly assessing the axillary nerve due to the shoulder injury, and ensure distal neurovascular integrity is documented before and after splinting.
Candidates often succumb to "tunnel vision," focusing exclusively on the elbow deformity. They may fail to mention the ipsilateral shoulder injury entirely or suggest immediate surgery without highlighting the need for systemic trauma clearance or specific neurovascular documentation.
The perfect answer demonstrates a hierarchical approach: 1. Safety: ATLS survey to rule out associated thoracic/cervical injuries. 2. Recognition: Explicitly identify the "Terrible Triad" (elbow) and the "Neer 2-part surgical neck" (shoulder). 3. Clinical Correlation: Acknowledge the risk of the "distracting injury." 4. Neurovascular focus: Explicitly mention the risk to the axillary nerve (deltoid motor/regimental badge sensation) and the importance of checking distal pulses and compartment status. 5. Systemic context: Briefly mention patient optimization (diabetes management) regarding infection risk.
You have decided on operative management for both the proximal humerus and the elbow. What is your surgical sequencing strategy, and what is the rationale behind it?
Candidate: I would stabilize the proximal humerus first. By securing the shoulder, I create a stable proximal lever arm. This makes the subsequent manipulation of the elbow during the Terrible Triad reconstruction safer, as I avoid placing stress on an unreduced or unstable humeral fracture while working on the elbow.
Suggesting the elbow should be addressed first. This is suboptimal because the maneuvers required to reduce the elbow joint under fluoroscopy place significant, uncontrolled leverage on the humerus, which could displace the fracture further or injure the neurovascular bundle.
A high-scoring answer explains the biomechanical logic: "I prioritize the proximal humerus to establish a stable proximal construct. This allows the limb to be manipulated safely during the complex elbow reconstruction. Furthermore, once the humerus is fixed, the surgeon has better control over the limb's rotation and length, which facilitates the tensioning of the elbow's ligamentous repairs (LUCL) and radial head prosthesis placement."
During your intraoperative assessment of the 'Terrible Triad', you note the coronoid fragment is small (Regan-Morrey Type II). Why is it critical to fix even this small fragment, and how would you surgically achieve this?
Candidate: The coronoid is the primary stabilizer against posterior subluxation. Even a small fragment often involves the anterior capsule. I would use a suture lasso technique or screw fixation to reattach it, ensuring the anterior buttress is restored to prevent recurrent instability.
Dismissing the coronoid fragment as "too small to fix." Candidates who miss the importance of the coronoid as the "keystone" of the elbow joint will fail the instability management component of the viva.
A comprehensive answer references the anatomy: "The coronoid provides the anterior buttress against the humerus. In the Terrible Triad, the coronoid is essentially the keystone of the joint. I would use a suture lasso technique—passing high-strength suture through the anterior capsule and tethering it to the posterior ulnar cortex—to convert the capsular injury into a stable, biological construct."
