Surgical Management of Psoriatic and Crystal-Induced Arthropathies of the Hand

Key Takeaway
Psoriatic arthritis and crystal-induced arthropathies present complex biomechanical challenges in the hand and upper extremity. Surgical intervention is indicated for severe deformity, intractable pain, or impending tendon rupture. This guide details evidence-based operative strategies, including metacarpophalangeal resection arthroplasty, proximal interphalangeal arthrodesis, and the management of tophaceous gout, providing orthopedic surgeons with critical technical pearls for optimizing functional outcomes in inflammatory hand disease.
INTRODUCTION TO INFLAMMATORY AND CRYSTAL ARTHROPATHIES
The surgical management of inflammatory and crystal-induced arthropathies of the hand and upper extremity requires a profound understanding of joint biomechanics, soft-tissue balancing, and the underlying systemic pathophysiology. While rheumatoid arthritis (RA) remains the most extensively described inflammatory arthropathy, psoriatic arthritis, gout, and pseudogout present unique patterns of joint destruction, soft-tissue compromise, and deformity.
An estimated 25% of patients with psoriatic arthritis develop a polyarticular presentation that clinically mimics rheumatoid arthritis. However, the surgical approach to psoriatic arthritis must account for its distinct propensity for profound osteolysis (arthritis mutilans), severe joint stiffness, and concurrent dermatological and vascular manifestations. Similarly, crystal arthropathies such as gout and calcium pyrophosphate dihydrate (CPPD) deposition disease (pseudogout) can cause catastrophic structural damage, necessitating meticulous surgical debridement, tendon reconstruction, and joint salvage procedures.
PSORIATIC ARTHRITIS OF THE HAND AND UPPER EXTREMITY
Epidemiology and Clinical Presentation
Psoriatic arthritis is a seronegative spondyloarthropathy that affects approximately 20% to 30% of patients with cutaneous psoriasis. The disease exhibits a highly variable clinical course, ranging from mild monoarthritis to severe, destructive polyarthritis. Unlike rheumatoid arthritis, which typically spares the distal interphalangeal (DIP) joints, psoriatic arthritis frequently involves the DIP joints, often in conjunction with characteristic nail changes.
Common clinical findings include:
* Dactylitis: "Sausage digits" resulting from concurrent tenosynovitis and joint inflammation.
* Nail Dystrophy: Pitting, onycholysis, and hyperkeratosis, which strongly correlate with DIP joint disease.
* Enthesitis: Inflammation at tendon and ligament insertions.
* Extra-articular Lesions: Psoriatic plaques commonly found on the extensor surfaces of the elbows and knees.
FIGURE 1: Common findings of psoriatic arthritis. Pitted nail deformities are a hallmark of the disease and are highly predictive of underlying distal interphalangeal joint arthropathy.

FIGURE 2: Typical psoriatic elbow lesion. Cutaneous manifestations often precede articular symptoms, though they may occur simultaneously.
Radiographic Evaluation and Differential Diagnosis
The radiographic hallmark of psoriatic arthritis is the simultaneous presence of erosive changes and bone proliferation. The classic "pencil-in-cup" deformity occurs due to severe osteolysis of the proximal phalanx head (the pencil) and periarticular bone proliferation at the base of the distal phalanx (the cup).
It is critical to differentiate psoriatic arthritis from other systemic inflammatory conditions, such as Systemic Lupus Erythematosus (SLE). SLE typically presents with Jaccoud's arthropathy—a non-erosive, reducible deformity driven by ligamentous laxity rather than primary articular destruction.
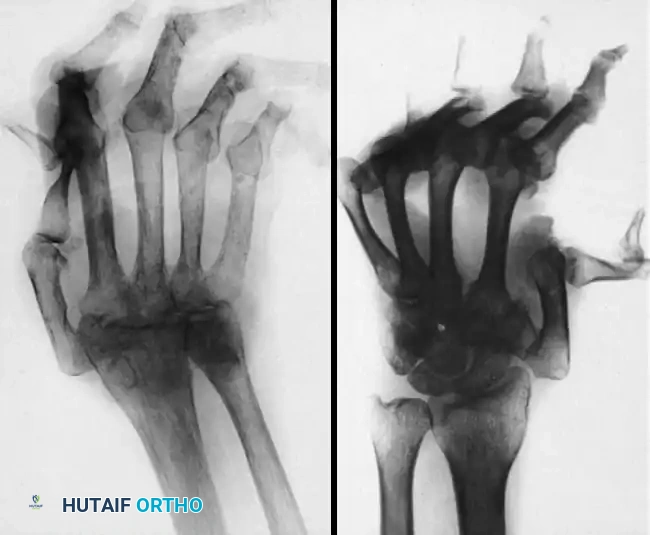
FIGURE 3: Typical radiographs of the hand and wrist in patients with systemic lupus erythematosus (SLE). Note the severe joint dislocations and ulnar drift without the erosive changes or joint space narrowing characteristic of psoriatic or rheumatoid arthritis.
In advanced psoriatic arthritis, profound joint destruction leads to subluxation and dislocation, particularly at the metacarpophalangeal (MCP) and interphalangeal (IP) joints.

FIGURE 4: Severe metacarpophalangeal joint dislocations and thumb interphalangeal joint destruction in advanced psoriatic arthritis.
Clinical Pearl: When evaluating a patient with severe hand deformities, the presence of joint subluxation without significant erosions should immediately raise the suspicion of SLE (Jaccoud's arthropathy), whereas profound osteolysis with periosteal reaction points toward psoriatic arthritis.
SURGICAL MANAGEMENT OF PSORIATIC HAND DEFORMITIES
Surgical intervention in psoriatic arthritis is indicated for intractable pain, progressive deformity, loss of function, and impending tendon rupture. Because psoriatic joints have a high propensity for spontaneous fusion and severe stiffness, the surgical strategy often differs from that of rheumatoid arthritis.
Proximal Interphalangeal (PIP) Joint Arthrodesis
Due to the severe soft-tissue contractures and the inherent tendency for psoriatic joints to stiffen, restoring functional movement at the PIP joint via arthroplasty is notoriously difficult and often yields poor long-term results. Consequently, arthrodesis is usually the procedure of choice for the proximal interphalangeal joint in psoriatic arthritis.
Surgical Technique:
1. Approach: A dorsal longitudinal or Chamay (V-shaped) incision is utilized over the PIP joint.
2. Preparation: The extensor tendon is split longitudinally. The collateral ligaments are excised to allow full exposure of the articular surfaces.
3. Joint Resection: The articular cartilage and subchondral bone are resected using a microsaw or rongeurs. A cup-and-cone reamer system can be used to maximize bony contact while allowing precise angular adjustments.
4. Positioning: The joints are fused in a functional cascade: typically 40° of flexion for the index finger, increasing by 5° for each subsequent ulnar digit (up to 55° for the small finger).
5. Fixation: Rigid fixation is achieved using crossed Kirschner wires, a tension band construct, or headless compression screws, depending on bone stock.
Metacarpophalangeal (MCP) Joint Resection Arthroplasty
MCP joint deformities in psoriatic arthritis may present as severe flexion contractures or paradoxical hyperextension deformities. Resection arthroplasty (often utilizing silicone interpositional implants) is an effective method to preserve joint motion and realign the digits.
Approach Based on Deformity (Nalebuff's Principles):
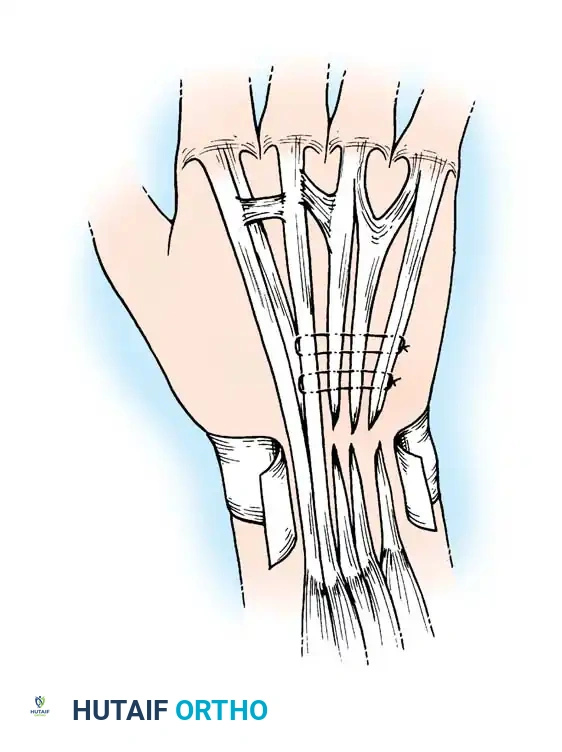
* Flexion Deformity: If the primary deformity is MCP flexion, the joint is approached through a standard dorsal incision. The extensor hood is incised, the metacarpal head is resected, and soft-tissue releases (including volar plate and collateral ligaments) are performed to correct the contracture.
* Hyperextension Deformity: If the MCP joint is hyperextended in conjunction with PIP joint flexion (a complex intrinsic-minus type posture), Nalebuff recommended approaching the MCP joint through a palmar incision. This allows for direct release of the contracted dorsal structures and volar subluxation, facilitating metacarpal head resection. This is typically followed by concurrent PIP joint fusion to stabilize the digit.
Despite meticulous surgical technique, patients with psoriatic arthritis often experience limited range of motion postoperatively due to the aggressive fibrotic nature of the disease.
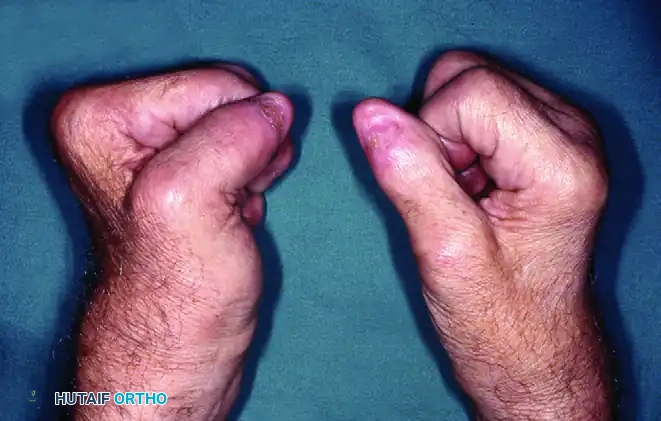
FIGURE 5: Right hand demonstrating limited finger flexion following metacarpophalangeal joint resection arthroplasty in a psoriatic patient.

FIGURE 6: The same right hand demonstrating limited finger extension. Postoperative stiffness remains a significant challenge in psoriatic arthroplasty.
Thumb Deformities and Contractures
The thumb in psoriatic arthritis frequently develops a severe web space adduction contracture, severely limiting grasp and pinch kinematics.
Surgical Correction:
* Soft Tissue Release: Release of the adductor pollicis muscle from its metacarpal origin is often required.
* Bony Procedures: If the carpometacarpal (CMC) joint is destroyed, trapezial excision (with or without ligament reconstruction and tendon interposition) is performed.
* Arthrodesis: Severe instability at the thumb MCP or IP joints is managed with primary arthrodesis to provide a stable post for pinch.
VASCULAR IMPAIRMENT AND ISCHEMIC COMPLICATIONS
A unique and challenging manifestation of psoriatic arthritis is severe digital ischemia, which can lead to fingertip ulceration and pulp necrosis. This vascular impairment is driven by chronic inflammation, vasculitis, and microvascular thrombosis.
Management of Fingertip Ulceration
Fingertip ulceration resulting from vascular impairment is best treated with an extremely conservative approach.
* Auto-amputation: Surgeons should generally wait for the ischemic tips to amputate spontaneously. This conservative strategy maximizes the retention of viable digital length and avoids operating in ischemic zones where surgical wounds will fail to heal.
* Medical Management: Intra-arterial injections of vasodilating drugs (e.g., reserpine, calcium channel blockers, or prostaglandins) can be highly effective in acutely improving digital circulation.
* Surgical Sympathectomy: Digital periarterial sympathectomy—involving the microsurgical stripping of the adventitia from the common and proper digital arteries—can relieve vasospasm. Although recurrence of ischemic changes may follow these procedures, the short-term result is often highly beneficial for wound healing and pain relief.
Management of Pulp Calcifications
Chronic ischemia and inflammation can lead to dystrophic calcification around the eroded fingertip pulps. These calcific deposits can be exquisitely painful.
* Surgical Excision: Calcifications may be excised through a mid-lateral incision to avoid scarring the tactile volar pad.
* Curettage: Alternatively, they may be carefully curetted. However, surgeons must warn patients that due to the underlying microvascular compromise, postoperative wound healing may be significantly delayed.
Surgical Warning: Never perform elective joint arthroplasty or arthrodesis in a digit with active ischemic ulceration. Vascular optimization and wound healing must precede any structural orthopedic reconstruction.
CRYSTAL-INDUCED ARTHROPATHIES: GOUT AND PSEUDOGOUT
Gouty Arthritis
Gout is a metabolic arthropathy characterized by the deposition of monosodium urate crystals in joints, tendons, and soft tissues. While women rarely develop gouty arthritis prior to menopause, the typical patient presenting with severe, destructive tophaceous gout is an elderly woman.
Diagnosis:
The presence of hyperuricemia alone does not establish the diagnosis of gout; serum uric acid levels may be elevated without an acute attack, and conversely, during an acute flare, serum uric acid levels may be entirely normal due to systemic inflammatory shifts.
* Definitive Diagnosis: Joint aspiration provides the only definitive diagnosis. Polarized light microscopy of the synovial fluid will reveal negatively birefringent, needle-shaped crystals.
Surgical Indications and Management:
Surgery for tophaceous deposits is rarely indicated as a first-line treatment, provided the patient can tolerate systemic uric acid–lowering therapies (e.g., allopurinol, febuxostat, pegloticase). However, surgical intervention becomes mandatory under specific conditions:
1. Nerve Compression: Tophaceous deposits frequently infiltrate the carpal tunnel, causing acute or chronic median nerve compression requiring urgent carpal tunnel release and tenosynovectomy.
2. Tendon Rupture: Urate crystals infiltrate the tendon substance, leading to attrition and spontaneous rupture (commonly the extensor pollicis longus or flexor tendons). Management requires debridement and tendon transfer or grafting.
3. Skin Breakdown and Infection: Massive tophi can cause overlying skin necrosis, leading to secondary bacterial infection.
4. Intractable Pain and Joint Destruction: Destroyed gouty joints may require arthrodesis or arthroplasty to restore function.
Surgical Techniques in Gout:
* Tophus Excision: Meticulous dissection is required, as tophi often intimately involve neurovascular bundles and tendon sheaths. Complete excision is rarely possible without damaging native structures; therefore, debulking is the primary goal.
* Tenosynovectomy: Extensive removal of infiltrated synovium helps decompress the compartment and prevent tendon rupture.
Pseudogout (CPPD Deposition Disease)
Pseudogout, or calcium pyrophosphate dihydrate (CPPD) crystal deposition disease, is more commonly recognized in the knee but frequently involves the hand and wrist.
Clinical Presentation:
In the upper extremity, CPPD most commonly affects the radiocarpal joint and the triangular fibrocartilage complex (TFCC), leading to a pattern of destruction known as SLAC (scapholunate advanced collapse) or SCAC (scaphoid chondrocalcinosis advanced collapse) wrist.
* Acute Flares: An acute attack of pseudogout in the hand or wrist presents with profound erythema, swelling, and severe pain, which can perfectly mimic acute septic arthritis.
* Diagnosis: Aspiration reveals positively birefringent, rhomboid-shaped crystals.
Surgical management of CPPD arthropathy mirrors that of osteoarthritis, often culminating in proximal row carpectomy (PRC) or partial/total wrist arthrodesis once conservative measures fail.
POSTOPERATIVE PROTOCOLS AND REHABILITATION
The postoperative management of inflammatory and crystal arthropathies requires a delicate balance between protecting surgical repairs and preventing catastrophic stiffness.
- Immobilization: Following PIP arthrodesis or MCP arthroplasty, the hand is immobilized in a bulky, non-compressive dressing with a volar plaster splint. The wrist is held in 20° to 30° of extension, with the MCP joints supported in appropriate alignment based on the procedure performed.
- Early Mobilization: For MCP resection arthroplasties, dynamic extension splinting is initiated within 3 to 5 days postoperatively to guide the alignment of the pseudo-capsule while allowing active flexion.
- Wound Care: Given the high incidence of microvascular compromise (especially in psoriatic and tophaceous patients), sutures are left in place longer than usual (typically 14 to 21 days) to prevent wound dehiscence.
- Medical Co-management: Close collaboration with a rheumatologist is essential. Biologic disease-modifying antirheumatic drugs (DMARDs) must be managed perioperatively to balance the risk of infection against the risk of a severe postoperative disease flare.
CONCLUSION
The surgical management of psoriatic arthritis, gout, and pseudogout demands a highly individualized approach. Surgeons must navigate compromised soft-tissue envelopes, severe osteolysis, and complex multi-planar deformities. By adhering to established biomechanical principles—favoring PIP arthrodesis for stability, utilizing strategic approaches for MCP arthroplasty, and exercising profound caution with ischemic digits—the orthopedic surgeon can reliably alleviate pain and restore functional capacity in this challenging patient population.
You Might Also Like