Proximal Humeral Fractures: Comprehensive Surgical Management

Key Takeaway
Proximal humeral fractures demand a nuanced understanding of shoulder biomechanics, vascular anatomy, and bone quality. Treatment ranges from early mobilization in stable, non-displaced patterns to complex operative interventions—including locked plating, intramedullary nailing, and arthroplasty—for displaced multi-part fractures. This guide details evidence-based protocols, the Neer classification, Hertel radiographic criteria for ischemia, and step-by-step surgical techniques to optimize functional recovery and minimize complications like osteonecrosis.
PROXIMAL HUMERAL FRACTURES: ACADEMIC OVERVIEW AND EPIDEMIOLOGY
Proximal humeral fractures represent one of the most common fragility fractures encountered in orthopedic traumatology, particularly among the elderly osteoporotic population. The management of these injuries requires a profound understanding of shoulder biomechanics, the delicate vascular supply to the humeral head, and the deforming forces exerted by the rotator cuff.
The primary objective in treating proximal humeral fractures is to achieve a painless, functional shoulder. While many of these fractures are minimally displaced and amenable to nonoperative management, displaced multi-part fractures present a significant surgical challenge. The surgeon must carefully balance the need for anatomical reduction and stable fixation against the risks of soft tissue stripping, devascularization, and subsequent osteonecrosis (avascular necrosis).
Clinical Pearl: Always use adequate radiograms to fully understand the traumatic lesion. Be cautious about denying older patients effective operative treatment based solely on age; physiological age and functional demands are far more critical determinants. When operating, utilize a safe and simple surgical approach, know the options for internal fixation, and recognize the value of prosthetic replacement in unsalvageable fractures.
Clinical Anatomy and Biomechanics
The proximal humerus is anatomically divided into four distinct segments, which form the basis of modern classification systems:
1. The Humeral Head (Articular Segment): Covered by hyaline cartilage.
2. The Greater Tuberosity: The insertion site for the supraspinatus, infraspinatus, and teres minor.
3. The Lesser Tuberosity: The insertion site for the subscapularis.
4. The Proximal Humeral Shaft: The insertion site for the pectoralis major.
Fracture displacement is dictated by the pull of these attaching muscles. The supraspinatus pulls the greater tuberosity superiorly and posteriorly; the subscapularis pulls the lesser tuberosity medially; and the pectoralis major pulls the humeral shaft medially and anteriorly.
The Glenopolar Angle
The glenopolar angle is a critical radiographic measurement used to assess the rotational alignment of the glenoid, which can be altered in complex shoulder trauma involving the scapula and proximal humerus. The angle is measured between a line connecting the most cranial with the most caudal point of the glenoid cavity, and a line connecting the most cranial point of the glenoid cavity with the most caudal point of the scapular body.

Normal glenopolar angle (A). The normal glenopolar angle ranges from 30 to 45 degrees.

Abnormal glenopolar angle (B), indicating significant rotational displacement.
Vascular Anatomy and Osteonecrosis Risk
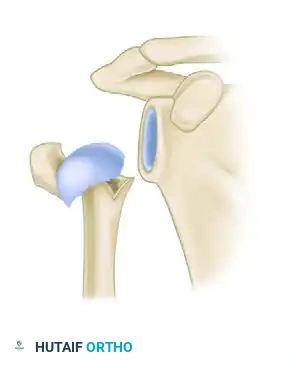
The blood supply to the proximal humerus is a critical factor in surgical decision-making. The primary arterial supply is derived from the anterior and posterior humeral circumflex arteries, which branch from the axillary artery.
The anterior humeral circumflex artery gives rise to the arcuate artery, which ascends in the bicipital groove and supplies the majority of the humeral head. However, recent microvascular studies emphasize the significant contribution of the posterior humeral circumflex artery, which supplies the posterior and inferior aspects of the humeral head via intraosseous anastomoses.
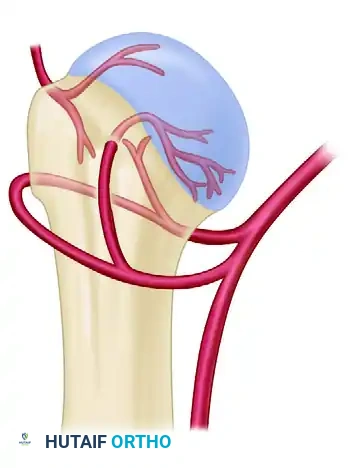
Blood supply of the proximal humerus, highlighting the anterior and posterior humeral circumflex arteries and the arcuate artery.
Displaced three-part and four-part fractures markedly alter the articular congruity of the glenohumeral joint and have the highest likelihood of disrupting this major blood supply. Osteonecrosis is most likely to occur after displaced four-part fractures, particularly when the medial calcar hinge is disrupted.
CLASSIFICATION SYSTEMS
The Neer Classification
Despite being cited for limitations regarding interobserver reliability, the Neer classification system remains the gold standard for guiding treatment. It is based on the four-part anatomy of the proximal humerus.
The Neer Criterion for Displacement: A segment is considered "displaced" only if there is greater than 1 cm of separation or greater than 45 degrees of angulation.
- One-Part Fractures: No fragments meet the displacement criteria, regardless of the number of fracture lines.
- Two-Part Fractures: One fragment is displaced (e.g., surgical neck, greater tuberosity).
- Three-Part Fractures: The shaft is displaced, and one tuberosity is displaced. The remaining tuberosity remains attached to the articular segment, causing rotational deformity.
- Four-Part Fractures: All four segments are displaced. The articular segment is devoid of soft tissue attachments and is at high risk for avascular necrosis.
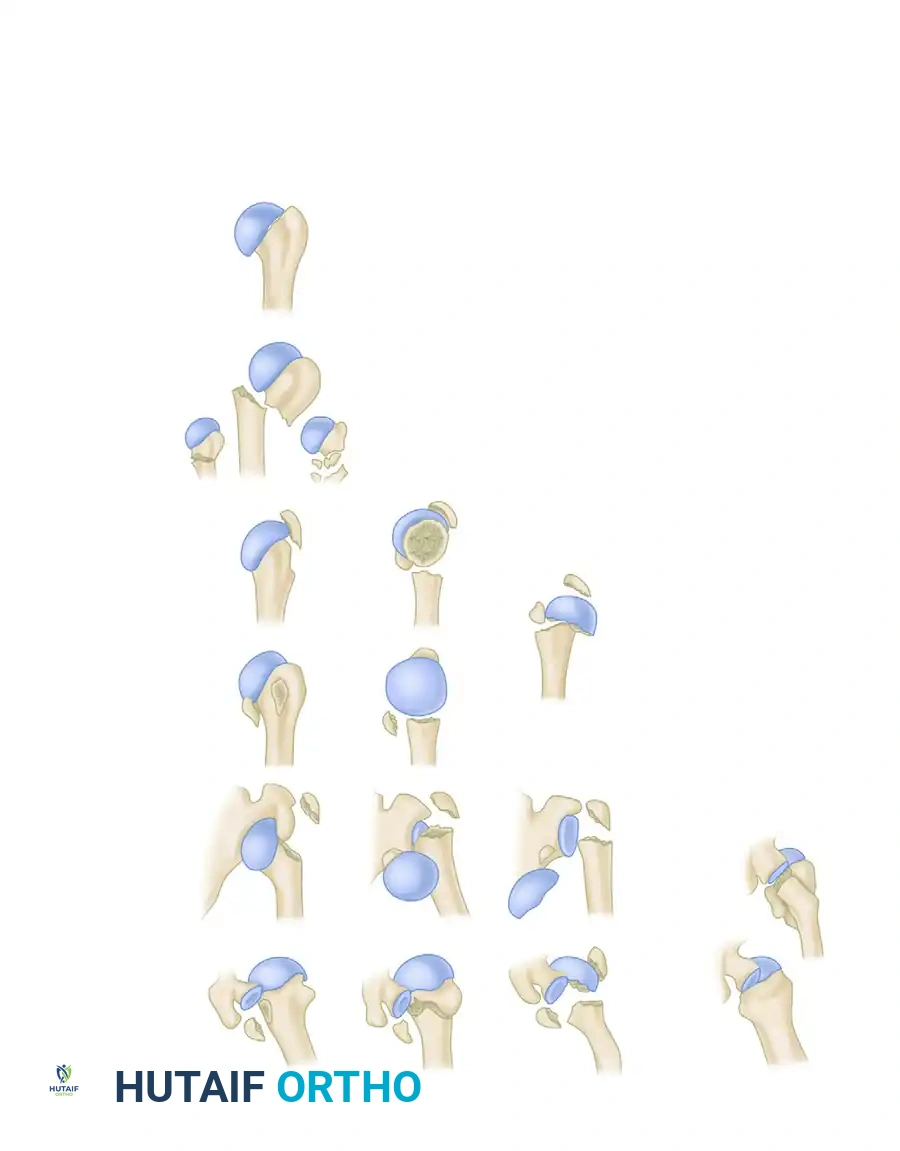
Neer’s terminology of the four-segment classification of displaced fractures and fracture-dislocations.
RADIOGRAPHIC EVALUATION
A complete trauma series of the shoulder is mandatory for all patients suspected of having a proximal humeral fracture. Relying on a single AP view is a common pitfall that leads to missed dislocations and misclassified fracture patterns.
- True Anteroposterior (AP) View (Grashey View): Taken perpendicular to the plane of the scapula to show the glenohumeral joint in profile.
- Scapular Y View (Lateral View): Taken parallel to the plane of the scapula to assess anterior or posterior displacement of the humeral head.
Special radiographic view perpendicular to the plane of the scapula to show the glenohumeral joint in profile (A).
View parallel to the plane of the scapula to show anterior and posterior displacement (B).
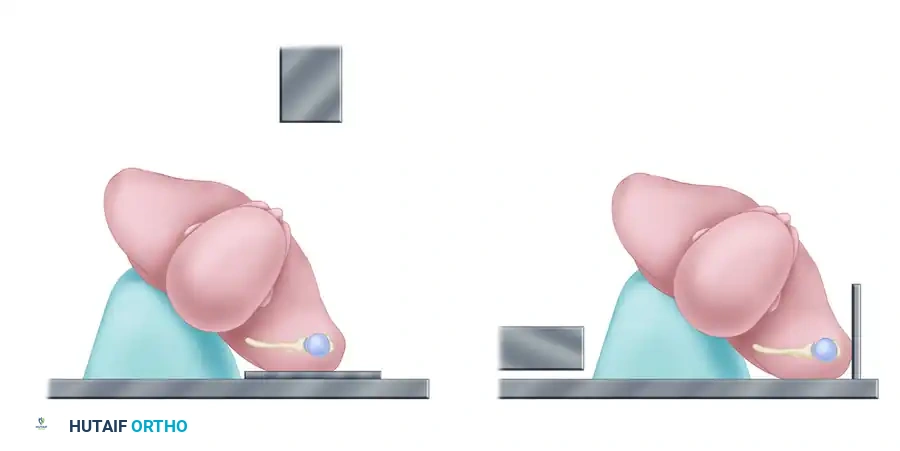
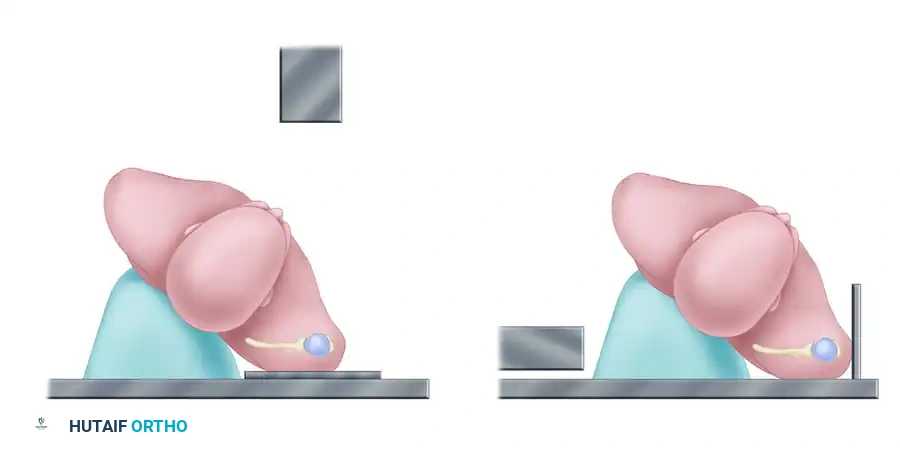
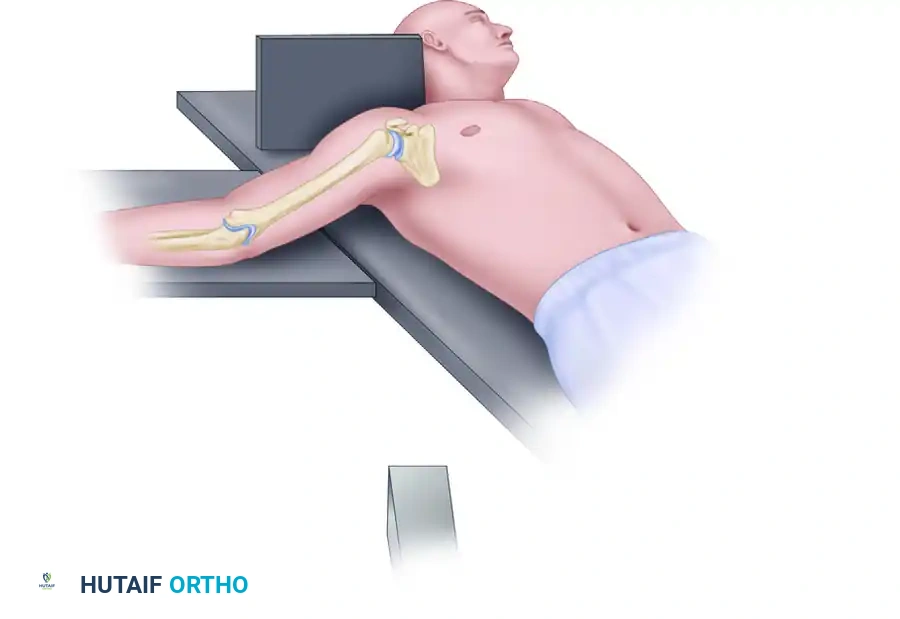
- Axillary View: Essential for determining the exact anteroposterior relationship of the humeral head to the glenoid and assessing lesser tuberosity fractures.

Method of obtaining an axillary view of the glenohumeral joint. Minimal abduction of the injured arm is required.
Advanced Imaging (CT Scanning)
If the amount of displacement of the humeral head or tuberosity fragments is unclear on standard radiographs, or if articular surface involvement (head-splitting fracture) is suspected, an axial CT scan with 2-mm sections and 3D reconstructions is highly indicated.
CT scan of a complex humeral head-splitting fracture, providing critical detail for preoperative planning.
PREDICTORS OF ISCHEMIA AND BONE QUALITY
Before surgery is considered, the surgeon must determine if the blood supply and bone quality are adequate to support internal fixation.
The Hertel Radiographic Criteria
Hertel et al. described specific radiographic criteria to predict ischemia of the humeral head following fracture. The combination of an anatomical neck fracture pattern, minimal metaphyseal extension, and disruption of the medial hinge has a 97% positive predictive value for humeral head ischemia.
- Metaphyseal Extension: The length of the diaphyseal cortical bone attached to the articular segment. Extension of < 8 mm is highly predictive of ischemia.
- Medial Hinge Disruption: Displacement of the medial calcar > 2 mm indicates severe periosteal tearing and vascular disruption.
Hertel Criteria A: Metaphyseal extension of the humeral head greater than 9 mm (Good prognosis).

Hertel Criteria B: Metaphyseal extension of the humeral head less than 8 mm (Poor prognosis).

Hertel Criteria C: Undisplaced medial hinge (Intact vascular supply).
Hertel Criteria D: Medial hinge with greater than 2-mm displacement (High risk of ischemia).
Assessing Bone Mineral Density (Cortical Thickness)
The cortical thickness of the humeral diaphysis is a reliable and reproducible predictor of bone mineral density (BMD) and the potential success of internal fixation. The combined cortical thickness is the average of the medial and lateral cortical thickness at two specific levels.
Surgical Warning: A combined cortical thickness of less than 4 mm generally precludes standard internal fixation because adequate screw purchase cannot be obtained. In such cases, sling immobilization, transosseous suture fixation, or hemiarthroplasty/reverse total shoulder arthroplasty may be superior options.
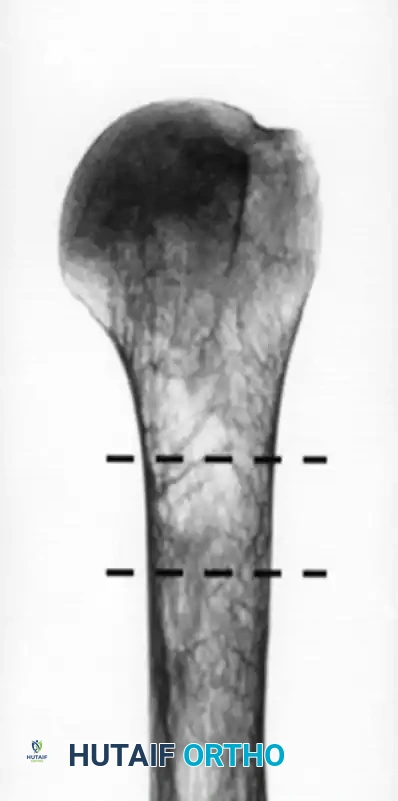
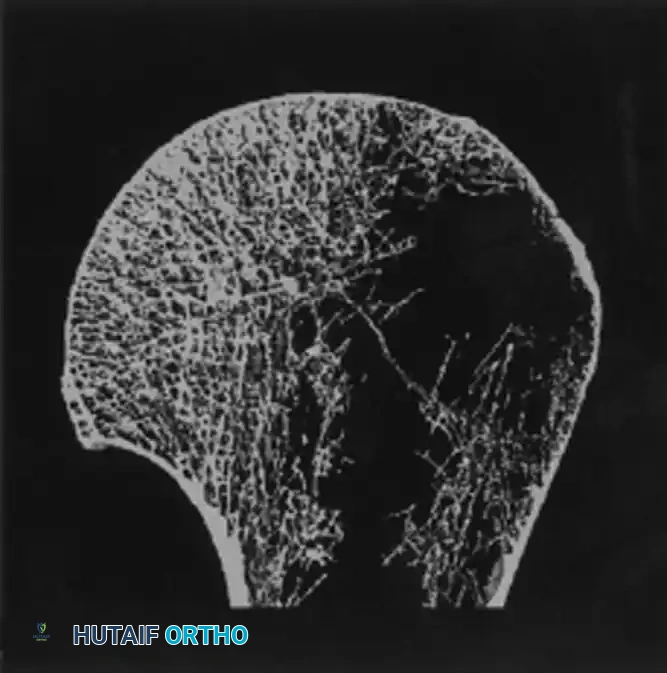
Example of a patient with low bone mineral density (A). Notice the extremely thin cortices.
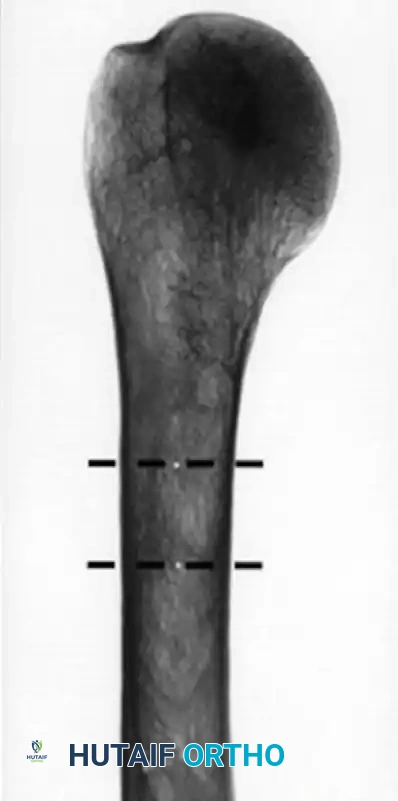
Example of a patient with high bone mineral density (B). Two levels are used to measure cortical thickness of the humeral diaphysis.
NONOPERATIVE TREATMENT
Nonoperative treatment can achieve a functional, painless extremity in the vast majority (up to 80%) of proximal humeral fractures. The glenohumeral joint's extensive range of motion accommodates moderate angular deformity without significant functional loss.
Indications for Nonoperative Management:
* Minimally displaced fractures (Neer one-part).
* Two-, three-, or four-part fractures in elderly, low-demand patients, or those with severe medical comorbidities precluding anesthesia.
* Acceptable angulation (generally < 45 degrees) and displacement (< 1 cm). Varus angulation is poorly tolerated compared to valgus impaction.
Rehabilitation Protocol:
The first step is to determine if the humeral head and shaft move as a unit. If the fracture is stable, a sling is used for comfort, and a physical therapy regimen with pendulum exercises is initiated early, usually within 1 week. A randomized controlled trial demonstrated that early (within 72 hours) passive mobilization in impacted fractures is safe and more effective in restoring function than conventional 3-week immobilization. If the fracture is unstable, physical therapy is delayed for 2 to 4 weeks.
OPERATIVE TREATMENT: SURGICAL TECHNIQUES
The decision to operate is driven by fracture displacement, instability, and patient factors (age, activity level). The ultimate goal is the anatomical restoration of the proximal humerus with stable fixation that permits early functional range of motion. Chronic malunions and nonunions are notoriously difficult to treat and yield poor outcomes.
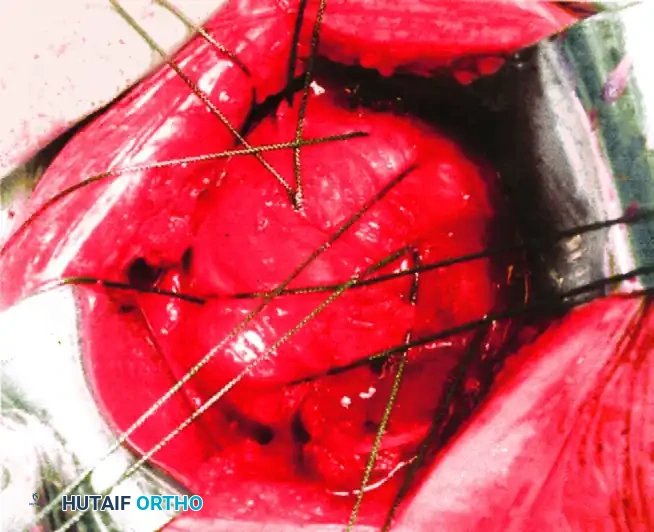
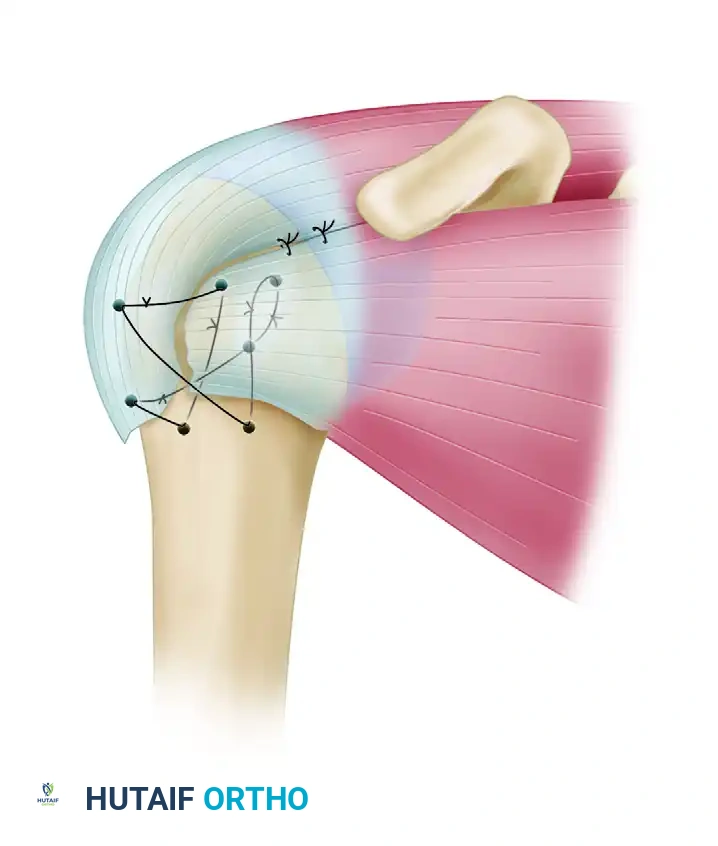
1. Transosseous Suture Fixation
Transosseous suture fixation is an excellent, minimally invasive technique, particularly in patients with poor bone quality where metal implants might fail.
Advantages:
* Incorporates the robust rotator cuff insertion to increase fixation strength.
* Minimal soft tissue dissection, preserving the delicate blood supply.
* Low rates of osteonecrosis.
* Avoidance of bulky, expensive hardware that may cause subacromial impingement.
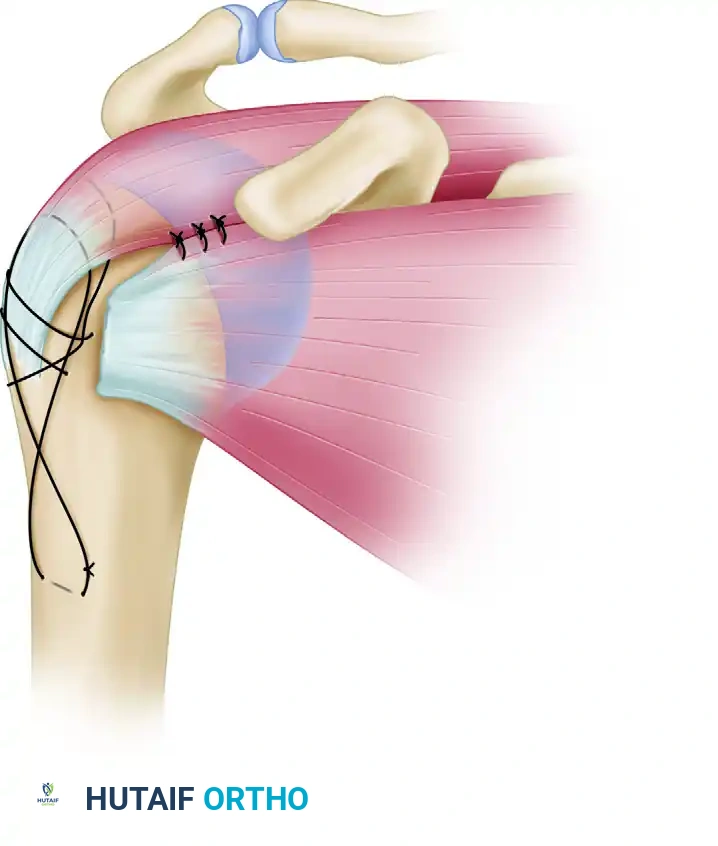
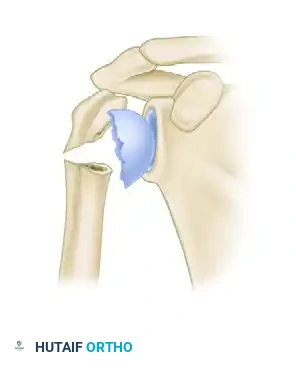
Transosseous nonabsorbable sutures incorporate the rotator cuff to increase fixation and help control tuberosity fragments.
Technique: Heavy, nonabsorbable sutures (e.g., #5 FiberWire) are passed through the bone-tendon junction of the supraspinatus and subscapularis. These are then passed through drill holes in the intact humeral shaft and tied securely, neutralizing the deforming forces of the rotator cuff.
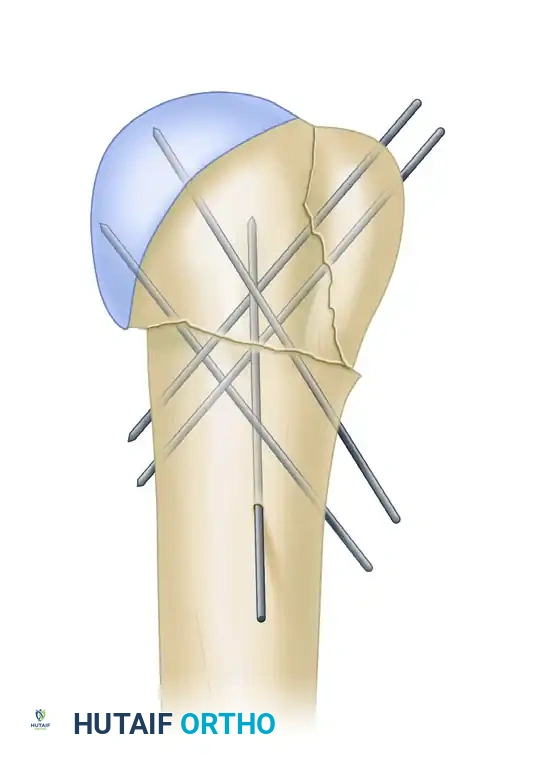
2. Percutaneous Pinning
Percutaneous pinning offers the advantage of avoiding further damage to the soft tissue envelope. It is relatively inexpensive and yields good results in two-part, three-part, and valgus-impacted four-part fractures.
Indications & Prerequisites:
* Satisfactory closed reduction must be achievable.
* Adequate bone stock.
* Minimal metaphyseal comminution.
* Intact medial calcar.
Fluoroscopic setup and initial pin placement for percutaneous fixation.

AP fluoroscopic view demonstrating terminally threaded Schanz pins inserted from the lateral cortex into the humeral head.
Lateral fluoroscopic view confirming multi-planar pin fixation.
Pitfall: Loss of fixation, pin track infections, and axillary nerve injuries are common complications. The axillary nerve runs approximately 5-7 cm distal to the lateral acromion; pins must be placed carefully to avoid this structure. Percutaneous pinning is strictly contraindicated for fractures with severe metaphyseal comminution.
3. Intramedullary Nailing
Intramedullary (IM) nailing provides superior biomechanical stability compared to percutaneous pinning, functioning as a load-sharing device. It is particularly useful for surgical neck fractures with diaphyseal extension.
Advantages:
* More stable fixation in osteoporotic bone.
* Minimal soft tissue dissection required for insertion.
* Newer nail designs feature polyaxial locking screws and polyethylene bushings to prevent screw back-out.
Disadvantages:
* Insertion violates the rotator cuff (supraspinatus tendon), which can lead to postoperative shoulder pain and cuff dysfunction.
* Poor results in multi-part fractures with displaced tuberosities.

Guidewire placement and initial reaming for antegrade intramedullary nailing.
Insertion of the proximal locking screws through the nail to secure the humeral head.
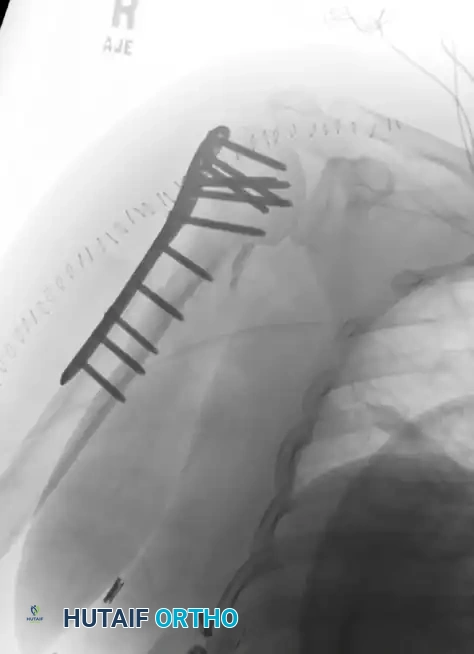
Final fluoroscopic AP view demonstrating stable intramedullary nail fixation of a proximal humeral fracture.
4. Open Reduction and Internal Fixation (ORIF) with Locked Plating
ORIF with a proximal humeral locking plate (e.g., PHILOS) is the workhorse for displaced multi-part fractures. Locking plates act as fixed-angle constructs, providing rigid stability even in osteoporotic bone.
Surgical Approach (Deltopectoral):
1. Positioning: The patient is placed in the beach-chair position. The arm must be freely draped to allow manipulation.
2. Incision: A standard deltopectoral incision is made, utilizing the internervous plane between the deltoid (axillary nerve) and pectoralis major (medial/lateral pectoral nerves).
3. Deep Dissection: The cephalic vein is identified and usually retracted laterally with the deltoid. The clavipectoral fascia is incised.
4. Reduction: The fracture is reduced. Heavy nonabsorbable sutures are placed through the rotator cuff insertions at the greater and lesser tuberosities to manipulate the fragments and later tie them to
Associated Surgical & Radiographic Imaging