Peroneal Tendon Repair and Reconstruction: Advanced Surgical Guide
Key Takeaway
Peroneal tendon repair and reconstruction are critical procedures for addressing lateral hindfoot pain and instability caused by traumatic or attritional ruptures. This comprehensive guide details the biomechanical principles, precise surgical techniques—including tenodesis, superior peroneal retinaculum reinforcement, and concurrent lateral ligament stabilization—and evidence-based postoperative protocols necessary to restore dynamic ankle stability and prevent recurrent subluxation in high-demand patients.
Comprehensive Introduction and Patho-Epidemiology
Peroneal tendon disorders encompass a complex and multifaceted spectrum of lateral hindfoot pathologies, ranging from acute inflammatory tenosynovitis and chronic tendinosis to longitudinal split tears, acute ruptures, attritional degeneration, and chronic subluxation or dislocation. The peroneus longus and peroneus brevis tendons serve as the primary dynamic stabilizers of the lateral ankle and hindfoot, working in concert with the static lateral ligamentous complex to resist inversion stresses. When conservative management algorithms—such as immobilization, physical therapy, and judicious orthotic management—fail to yield symptomatic relief, surgical intervention via advanced peroneal tendon repair and reconstruction becomes an absolute imperative. The overarching surgical goals are to restore the biomechanical integrity of the lateral column, alleviate debilitating lateral hindfoot pain, prevent progressive hindfoot varus deformity, and facilitate a return to pre-injury functional levels.
The epidemiology of peroneal tendon pathology reveals a bimodal distribution, frequently afflicting young, high-demand athletes as well as older individuals with progressive degenerative changes. In the athletic population, particularly those involved in sports requiring rapid changes of direction, pivoting, or jumping (e.g., basketball, soccer, gymnastics), acute injuries often manifest as sudden avulsions, superior peroneal retinaculum (SPR) stripping, or traumatic dislocations. Conversely, in the older demographic, the etiology is typically insidious, driven by repetitive microtrauma, chronic lateral ankle instability (CLAI), and underlying biomechanical malalignments such as a driven cavovarus foot. The chronic laxity of the anterior talofibular ligament (ATFL) and calcaneofibular ligament (CFL) places an exorbitant eccentric load on the peroneal tendons, accelerating their degeneration and predisposing them to attritional failure.
Pathomechanically, the "bowstringing" effect plays a critical role in the development of peroneal tendon disorders. When the SPR is attenuated or acutely ruptured, the tendons lose their primary static restraint. During active dorsiflexion and eversion, the tendons subluxate or dislocate anteriorly over the lateral malleolus. This recurrent mechanical instability leads to a "nutcracker" phenomenon, wherein the peroneus brevis tendon—situated anterior and medial to the peroneus longus—is repeatedly crushed against the sharp posterior fibular ridge. This repetitive shear stress is the primary genesis of longitudinal split tears within the peroneus brevis. Furthermore, an anatomically shallow or convex retromalleolar groove exacerbates this instability, creating a hostile mechanical environment that precludes spontaneous healing and necessitates comprehensive surgical reconstruction.
Recognizing the intricate relationship between peroneal tendon pathology and global foot and ankle biomechanics is paramount for the operating surgeon. Isolated repair of a torn tendon in the presence of an uncorrected, rigid hindfoot varus deformity or profound lateral ankle instability is universally doomed to failure. The abnormal kinematics will relentlessly overload the meticulous surgical repair, leading to recurrent tearing, persistent pain, and progressive functional decline. Therefore, an advanced surgical approach mandates a holistic evaluation of the patient's lower extremity alignment, ensuring that any concurrent osseous or ligamentous abnormalities are addressed simultaneously—often requiring calcaneal osteotomies, first metatarsal dorsiflexion osteotomies, or lateral ligamentous reconstructions—to optimize the biomechanical milieu for tendon healing.
Detailed Surgical Anatomy and Biomechanics
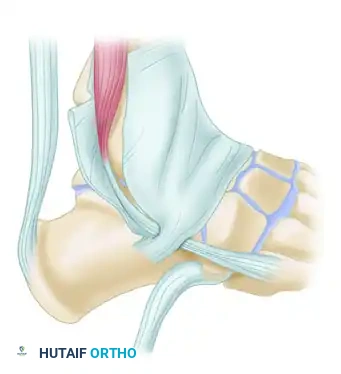
A profound, three-dimensional understanding of the lateral ankle and hindfoot anatomy is non-negotiable for the orthopedic surgeon undertaking peroneal tendon reconstruction. The osteology of the distal fibula forms the foundational architecture of the lateral compartment. The posterior surface of the lateral malleolus features the retromalleolar groove, a sulcus that houses the peroneal tendons. Morphological studies indicate significant anatomical variance in this groove; it is concave in only approximately 11% to 30% of the population, flat in the majority, and distinctly convex in a smaller subset. A shallow or convex groove inherently predisposes the patient to tendon subluxation. The floor of this groove is lined with fibrocartilage, which facilitates smooth tendon gliding and must be meticulously managed during any groove-deepening procedures to prevent postoperative adhesions.
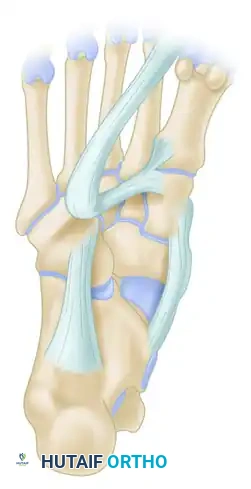
The Peroneus Brevis (PB) muscle originates from the distal two-thirds of the lateral fibular shaft and the adjacent intermuscular septa. As it transitions into its tendinous portion, it courses distally within the retromalleolar groove, lying anterior and medial to the peroneus longus, directly juxtaposed against the fibrocartilaginous surface of the fibula. It then passes inferior to the peroneal tubercle of the calcaneus before inserting onto the tuberosity at the base of the fifth metatarsal. Biomechanically, the PB is the primary evertor of the foot and a crucial dynamic stabilizer against inversion forces. Its deep, constrained position within the groove makes it uniquely susceptible to mechanical attrition and longitudinal split tears, particularly when compressed by the overlying, more robust peroneus longus tendon during forceful muscle contraction.
The Peroneus Longus (PL) muscle possesses a more proximal origin, arising from the head and proximal two-thirds of the lateral fibula. Its tendon courses posterior and lateral to the PB within the retromalleolar groove. Distal to the lateral malleolus, the PL tendon diverges from the PB, wrapping acutely around the cuboid within the cuboid groove, and traverses the plantar aspect of the midfoot to insert onto the plantar-lateral aspect of the medial cuneiform and the base of the first metatarsal. The PL serves a dual biomechanical role: it acts as an evertor of the hindfoot and a powerful plantarflexor of the first ray. This plantarflexion of the first ray is essential for stabilizing the medial column during the terminal stance and toe-off phases of the gait cycle. The presence of the os peroneum—a sesamoid bone located within the PL tendon at the level of the calcaneocuboid joint, present in approximately 20% of individuals—can complicate pathology, serving as a nidus for degenerative tearing or painful impingement syndromes.
The vascular supply to the peroneal tendons is a critical determinant of their healing capacity and a primary factor in the pathogenesis of degenerative ruptures. Both tendons receive their blood supply from the peroneal artery proximally and the posterior tibial artery distally via a complex network of vincula within their common synovial sheath. However, rigorous microangiographic studies have identified distinct "watershed" zones of relative hypovascularity. In both tendons, a significant avascular zone exists precisely at the turn of the lateral malleolus, corresponding to the area subjected to the highest mechanical friction and shear stress. An additional hypovascular zone exists in the PL tendon as it wraps around the cuboid. These regions of compromised perfusion are disproportionately vulnerable to tendinosis, attritional tearing, and delayed healing following surgical repair.
The retinacular system provides the essential static restraints that maintain the peroneal tendons within their anatomical trajectory. The Superior Peroneal Retinaculum (SPR) is the primary structure preventing anterior subluxation. It originates from the posterolateral ridge of the distal fibula and inserts onto the lateral calcaneal wall, blending with the Achilles tendon sheath and the superficial fascia. The SPR is not a simple, homogenous band; it consists of distinct superior and inferior bands that must be carefully evaluated and anatomically reconstructed during surgery. The Inferior Peroneal Retinaculum (IPR) originates from the lateral calcaneus and blends with the inferior extensor retinaculum, stabilizing the tendons as they course toward their respective insertions. Failure to restore the integrity and appropriate tension of these retinacular structures invariably leads to recurrent instability and surgical failure.
Exhaustive Indications and Contraindications
The decision to proceed with surgical intervention for peroneal tendon pathology requires a nuanced synthesis of the patient's clinical presentation, anatomical variants, functional demands, and response to conservative modalities. Surgery is rarely indicated as a first-line treatment for acute, non-traumatic tenosynovitis or mild tendinosis, which typically respond to a minimum of three to six months of conservative management, including immobilization in a controlled ankle motion (CAM) boot, non-steroidal anti-inflammatory drugs (NSAIDs), targeted physical therapy, and lateral heel wedges. However, structural lesions and mechanical instability represent definitive indications for operative management, as these pathologies lack the capacity for spontaneous biological resolution and will progressively deteriorate without mechanical restoration.
Primary indications for surgical repair include acute or chronic, complete ruptures of either the peroneus brevis or peroneus longus tendons. Longitudinal split tears of the peroneus brevis—often presenting with persistent retromalleolar pain and a palpable "click" during circumduction—are classic surgical indications, particularly when conservative measures fail to alleviate symptoms. Recurrent peroneal tendon subluxation or dislocation, whether traumatic in origin (associated with an avulsion of the SPR from the fibula) or habitual (associated with a shallow fibular groove), mandates surgical reconstruction to prevent rapid destruction of the tendons. Furthermore, attritional ruptures associated with an enlarged peroneal tubercle or os peroneum syndrome (hypertrophy, fracture, or proximal migration of the sesamoid) require surgical excision of the offending osseous prominence and concomitant tendon repair or tenodesis.
Contraindications to peroneal tendon surgery must be rigorously evaluated to prevent catastrophic postoperative complications. Absolute contraindications include active, uncontrolled local or systemic infection, severe peripheral arterial disease compromising the vascularity of the lateral surgical flap, and profound medical comorbidities that preclude the safe administration of general or regional anesthesia. Severe, unmanageable peripheral neuropathy (e.g., advanced Charcot neuroarthropathy) is generally considered an absolute contraindication due to the unacceptably high risk of postoperative wound breakdown, non-compliance with weight-bearing restrictions, and failure of the reconstruction.
Relative contraindications require careful preoperative optimization and shared decision-making. Patients with poorly controlled diabetes mellitus, active tobacco use, or chronic corticosteroid use are at a significantly elevated risk for wound dehiscence, delayed tendon healing, and deep infection. In these populations, surgery should be delayed until glycemic control is optimized and smoking cessation is achieved. Additionally, performing an isolated peroneal tendon repair in a patient with a severe, uncorrected, rigid cavovarus foot deformity is a relative contraindication; the underlying biomechanical driver must be addressed concurrently (e.g., via a Dwyer calcaneal osteotomy) to prevent inevitable failure of the soft-tissue reconstruction.
| Category | Specific Conditions | Clinical Rationale |
|---|---|---|
| Absolute Indications | Acute complete rupture of PB or PL | Loss of dynamic lateral stability; requires primary repair to restore function. |
| Recurrent Subluxation/Dislocation | Incompetent SPR and/or shallow groove causing mechanical attrition; requires SPR reconstruction and groove deepening. | |
| Symptomatic Os Peroneum Syndrome | Fracture or attritional tear at the cuboid tunnel; requires excision and tenodesis. | |
| Relative Indications | Chronic longitudinal split tears | Refractory to 3-6 months of conservative care; requires tubularization and debridement. |
| Severe stenosing tenosynovitis | Failure of conservative management; requires tenosynovectomy and sheath release. | |
| Absolute Contraindications | Active local or systemic infection | High risk of deep space infection and hardware/repair failure. |
| Severe Peripheral Arterial Disease | Inadequate perfusion to heal the extensile posterolateral incision; high risk of necrosis. | |
| Advanced Charcot Neuroarthropathy | Lack of protective sensation leads to non-compliance and catastrophic failure of repair. | |
| Relative Contraindications | Uncorrected rigid cavovarus deformity | Biomechanical overload will lead to recurrent rupture if the bony alignment is not corrected concurrently. |
| Active heavy tobacco use | Significant risk of wound dehiscence and delayed tendon healing; requires cessation protocol. |
Pre-Operative Planning, Templating, and Patient Positioning
Comprehensive preoperative planning is the cornerstone of successful peroneal tendon reconstruction. The clinical evaluation must be exhaustive, beginning with a detailed history of the mechanism of injury, duration of symptoms, and response to prior treatments. Physical examination involves precise palpation along the course of the tendons, from the posterior fibula to their respective insertions, to localize the point of maximal tenderness and identify any palpable defects or masses (such as a migrated os peroneum). Provocative testing is critical; the surgeon must assess for active subluxation by having the patient forcefully dorsiflex and evert the foot against resistance. Furthermore, a thorough assessment of global hindfoot alignment using the Coleman block test is mandatory to differentiate between a flexible, driven cavovarus deformity (which may correct with soft-tissue balancing) and a rigid deformity (which necessitates corrective osteotomies).
Imaging modalities are utilized to confirm the clinical diagnosis and meticulously map the extent of the pathology. Standard weight-bearing radiographs of the foot and ankle (anteroposterior, lateral, and mortise views) are obtained to assess for avulsion fractures of the lateral malleolus (the "fleck sign" indicative of SPR avulsion), hypertrophy of the peroneal tubercle, the position and integrity of the os peroneum, and overall hindfoot alignment. High-resolution ultrasound is highly operator-dependent but offers the distinct advantage of dynamic assessment, allowing the surgeon to visualize real-time subluxation of the tendons during active motion. Magnetic Resonance Imaging (MRI) remains the gold standard for preoperative templating. Axial T2-weighted sequences are particularly crucial for identifying longitudinal split tears of the peroneus brevis, assessing the depth of the retromalleolar groove, and evaluating the degree of tendinosis. The surgeon must be acutely aware of the "magic angle" artifact, which can artificially increase signal intensity in the tendons as they curve around the lateral malleolus, mimicking tendinopathy.
Surgical templating involves anticipating the required reconstructive techniques based on the MRI findings. If a massive, irreparable defect of both tendons is identified, the surgeon must be prepared with appropriate allograft tissue (e.g., semitendinosus or gracilis allograft) or autograft harvest options. The availability of specialized instrumentation, including high-speed burrs for groove deepening, small joint suture anchors (2.5mm to 3.0mm) for SPR reconstruction, and robust non-absorbable sutures (e.g., FiberWire or Orthocord) for tenodesis, must be confirmed prior to the induction of anesthesia. If concurrent lateral ankle instability is suspected, the necessary equipment for a modified Broström-Gould procedure must also be readily available.
Patient positioning is a critical element that dictates the ease and safety of the surgical exposure. The procedure is typically performed under general anesthesia, often supplemented with a regional popliteal sciatic nerve block for optimal postoperative analgesia. The patient is most commonly placed in the lateral decubitus position, ensuring the operative leg is uppermost and securely supported. Alternatively, a supine position with a substantial, firm bump placed under the ipsilateral hip can be utilized to internally rotate the leg, providing excellent, unhindered access to the posterolateral ankle while allowing simultaneous access to the anterior ankle or medial foot if concurrent procedures are planned. A well-padded thigh tourniquet is applied and inflated to an appropriate pressure (typically 250-300 mmHg) only after meticulous exsanguination of the limb using an Esmarch bandage, ensuring a bloodless surgical field.
Step-by-Step Surgical Approach and Fixation Technique
Incision and Extensile Exposure
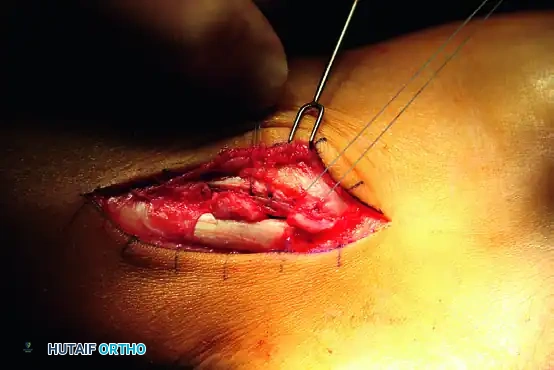
The surgical approach utilizes an extensile posterolateral incision, meticulously planned to provide comprehensive access to the entire retromalleolar region and the distal course of the tendons. The incision follows the posterior border of the fibula, beginning approximately 5 to 7 cm proximal to the tip of the lateral malleolus, and extends distally, curving gently toward the base of the fifth metatarsal or the cuboid, depending on the anticipated location of the primary pathology.
Dissection is carried sharply through the skin and subcutaneous tissues. It is of paramount importance to identify, mobilize, and protect the sural nerve and the lesser saphenous vein, which typically cross the surgical field in the distal aspect of the incision. The sural nerve is highly variable in its branching pattern and is exquisitely sensitive to traction; aggressive retraction must be strictly avoided to prevent devastating postoperative neuromas or neuropraxia. The surgeon must maintain full-thickness fasciocutaneous flaps to preserve the delicate vascular supply to the skin edges, thereby mitigating the risk of postoperative wound necrosis.
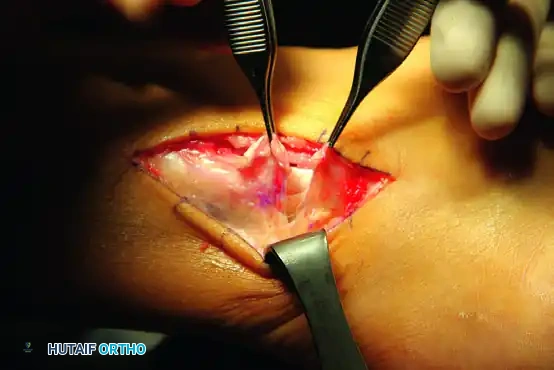
Retinaculum Incision and Tendon Assessment
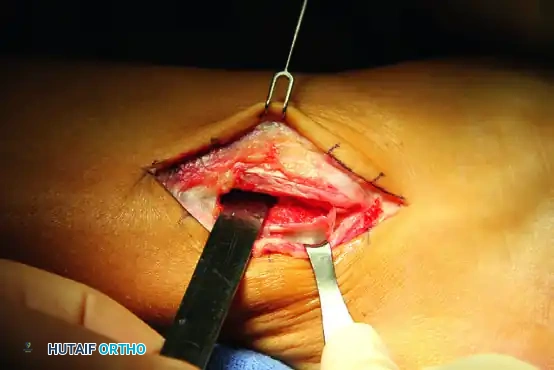
Once the superficial fascia is cleared, the Superior Peroneal Retinaculum (SPR) is definitively identified. The SPR is incised longitudinally, parallel to the posterior border of the fibula. Crucially, the surgeon must leave a robust 2 to 3 mm cuff of retinacular tissue attached to the fibular ridge. This cuff is essential; it provides a strong, vascularized tissue base for the subsequent watertight repair and imbrication of the retinaculum at the conclusion of the procedure.
Upon opening the common peroneal tendon sheath, a thorough tenosynovectomy is performed to remove inflammatory tissue and improve visualization. Both the peroneus brevis and longus tendons are systematically inspected along their entire visible length. The surgeon assesses for the presence of longitudinal split tears (most common in the brevis), complete transverse ruptures, severe tendinosis characterized by bulbous thickening and loss of normal fibrillar architecture, and any low-lying muscle bellies of the peroneus brevis or anomalous muscles (e.g., peroneus quartus) that may be contributing to overcrowding within the retromalleolar space.

Management of Tendon Ruptures and Tears
Primary Repair and Tubularization
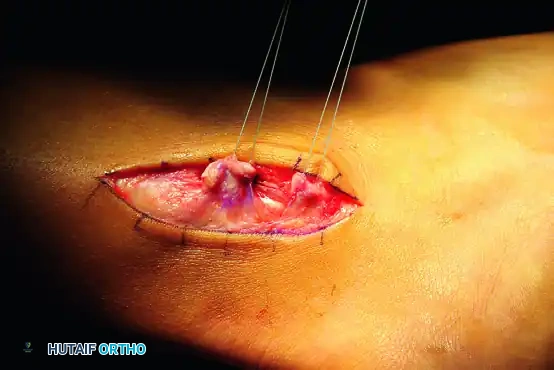
For isolated longitudinal split tears of the peroneus brevis, the degenerative, central, avascular portion of the tear is meticulously debrided using a scalpel or small rongeur. If more than 50% of the tendon's cross-sectional area remains viable and healthy, the tendon is repaired primarily. A running, interlocking suture technique using a 3-0 or 4-0 non-absorbable monofilament is employed to "tubularize" the tendon, restoring its smooth, cylindrical contour and ensuring it glides effortlessly within the fibular groove.
Tenodesis for Irreparable Single Tendon Rupture
If one tendon (frequently the peroneus brevis) is severely degenerated, fragmented, or irreparably ruptured, while the adjacent tendon remains structurally intact and robust, a tenodesis is definitively indicated. The diseased, non-viable segments of the ruptured tendon are aggressively excised back to healthy, bleeding tissue. The proximal and distal stumps of the excised tendon are then securely sutured to the adjacent intact tendon (e.g., a side-to-side tenodesis of the brevis to the longus). This is achieved using multiple, interrupted, figure-of-eight sutures with a heavy 2-0 non-absorbable braided suture. The critical technical nuance here is setting the tension: the tenodesis must be performed with the foot held in neutral dorsiflexion and mild eversion to establish appropriate resting tension and prevent a postoperative varus or valgus contracture.
Management of Attritional Ruptures at the Cuboid Level
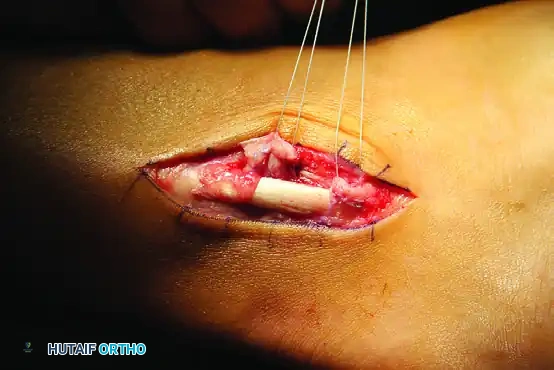
Attritional ruptures of the peroneus longus frequently occur distally, beneath the cuboid, and are intimately associated with pathology of the os peroneum.
The surgical exposure must be extended distally to visualize the cuboid tunnel. The attritional rupture site is identified, and the distal, degenerative end of the peroneus longus is resected 1 to 2 cm plantarward. If a fractured, hypertrophic, or degenerative os peroneum is present within this segment, it must be completely excised to eradicate the source of mechanical impingement.
Following resection, a tenodesis of the proximal stump of the peroneus longus to the intact peroneus brevis tendon is performed. As emphasized previously, this tenodesis must be executed under moderate tension while the foot is meticulously held in mild equinovalgus. This precise positioning is non-negotiable; it ensures the appropriate resting tension of the musculotendinous unit and prevents catastrophic postoperative over-lengthening, which would result in a profound loss of first ray plantarflexion power.
Fibular Groove Deepening
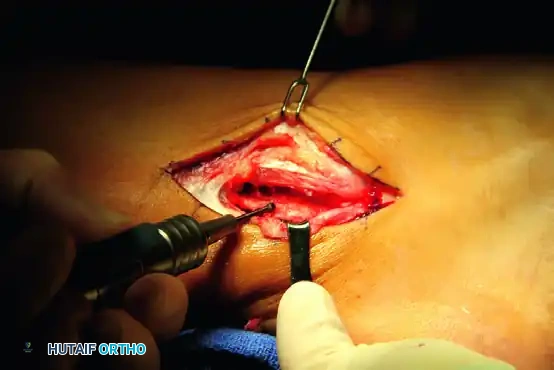
To definitively prevent postoperative subluxation, particularly in patients with a demonstrably shallow or convex retromalleolar groove, a groove-deepening procedure is mandatory. The periosteum and overlying fibrocartilage of the fibular groove are carefully incised and elevated as a single, contiguous flap, hinged laterally.
Using a high-speed, 4.0mm or 5.0mm spherical cutting burr, the surgeon decorticates the underlying cancellous bone of the distal fibula, creating a deep, concave trough. Crucially, the cortical shell of the groove must be preserved. Once adequate cancellous bone is removed, the cortical floor is tamped down into the newly created void using a broad bone tamp and mallet, effectively creating a deep, concave sulcus while preserving the smooth, gliding fibrocartilaginous surface for the tendons.
Superior Peroneal Retinaculum (SPR) Reconstruction
Following tendon repair and groove deepening, the SPR must be meticulously reconstructed and tensioned to restore the primary static restraint. The posterolateral ridge of the fibula is prepared by denuding it of soft tissue to expose a bleeding bony bed. Suture anchors (typically 2.5mm to 3.0mm, double-loaded with high-strength suture) are placed at 1.0 to 1.5 cm intervals along the fibular ridge. Alternatively, transosseous drill holes can be utilized if anchors are unavailable or contraindicated.

The sutures are passed through the lateral edge of the incised SPR in a horizontal mattress fashion. The retinaculum is then advanced and firmly secured to the fibula. The tension must be perfectly balanced: it must be tight enough to absolutely prevent anterior subluxation of the tendons over the fibular ridge, yet loose enough to allow unhindered, smooth gliding of the tendons during a full, dynamic range of ankle motion.
The "Trapdoor" Reinforcement Technique
In complex revision cases, or when the native SPR is severely attenuated, friable, or deficient, a periosteal flap reinforcement—often termed the "trapdoor" technique—is utilized to provide essential mechanical augmentation.
A posteriorly based, rectangular flap of thick periosteum is sharply elevated from the anterior and lateral aspects of the distal fibula, leaving its posterior attachment intact near the fibular ridge. This robust periosteal "trapdoor" is then reflected posteriorly, turned back over the newly repaired tendons, and sutured directly on top of the reconstructed
Clinical & Radiographic Imaging Archive
