Unraveling Extensor Mechanism Injuries: Patella Function & Trauma
Key Takeaway
In this comprehensive guide, we discuss everything you need to know about Unraveling Extensor Mechanism Injuries: Patella Function & Trauma. Extensor mechanism injuries, specifically patellar fractures, involve the largest sesamoid bone crucial for quadriceps leverage. These common injuries, affecting 20-50 year olds, arise from direct trauma or indirect forceful quadriceps contraction. Patients typically present with pain, swelling, tenderness, limited ambulation, and often impaired active knee extension, with open fractures being a surgical urgency.
Introduction and Epidemiology
Patellar fractures represent a significant disruption to the extensor mechanism of the lower extremity, necessitating precise anatomical understanding and rigorous surgical execution to restore baseline functional capacity. These fractures account for approximately 1% of all skeletal injuries. The demographic distribution demonstrates a male-to-female ratio of 2:1, with the highest incidence occurring in the active population between 20 and 50 years of age. Bilateral injuries are exceedingly uncommon and should immediately raise clinical suspicion for underlying metabolic bone disease, systemic tendinopathy, or high-energy polytrauma.
The mechanism of injury dictates the fracture pattern and the degree of soft tissue compromise.
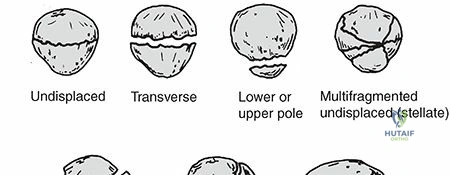
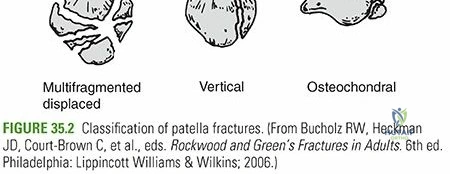
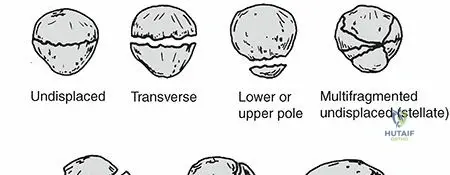
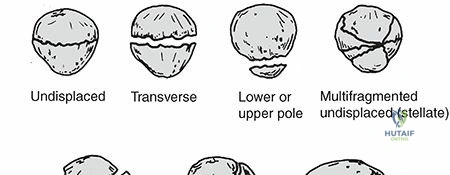
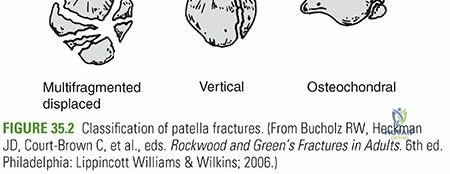
* Direct Trauma: Direct impact to the anterior knee, such as a dashboard injury during a motor vehicle collision or a direct fall onto a flexed knee, typically produces incomplete, simple transverse, stellate, or highly comminuted fracture patterns. Displacement is often minimal if the medial and lateral retinacular expansions remain intact. Abrasions or open traumatic arthrotomies are highly prevalent in this cohort. Active knee extension may be paradoxically preserved if the retinaculum is uncompromised.
* Indirect Trauma: This is the most common etiology, secondary to a forcible eccentric quadriceps contraction against a semiflexed knee (e.g., attempting to prevent a fall or stumbling). The intrinsic tensile strength of the patella is exceeded by the massive pull of the musculotendinous units. This mechanism classically yields a transverse fracture pattern, frequently accompanied by variable inferior pole comminution. The degree of osseous displacement correlates directly with the severity of retinacular tearing. Active knee extension is definitively lost.
* Combined Mechanisms: High-energy trauma, such as falls from significant heights, often imparts both axial loading and eccentric contractile forces, resulting in severely displaced, comminuted fractures with extensive soft tissue degloving.
Surgical Anatomy and Biomechanics
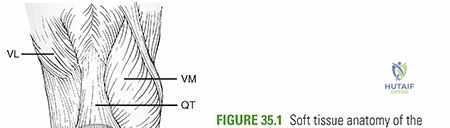
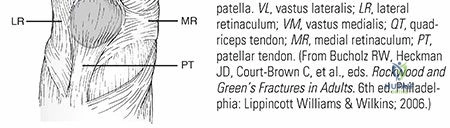
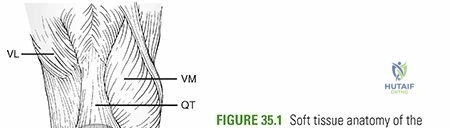
The patella is the largest sesamoid bone in the human body, embedded within the complex aponeurosis of the extensor mechanism. The quadriceps tendon inserts on the superior pole, blending fibers from the rectus femoris, vastus lateralis, vastus medialis, and vastus intermedius. The patellar ligament (tendon) originates from the inferior pole and inserts onto the tibial tubercle.
The posterior articular surface is divided by a vertical ridge into medial and lateral facets, with a smaller "odd" facet located on the extreme medial border. There are seven distinct articular facets in total. The lateral facet is the largest, comprising approximately 50% of the articular surface area. The patellar articular cartilage is the thickest in the human body, reaching up to 10 mm in depth, reflecting the massive patellofemoral joint reaction forces it must withstand.
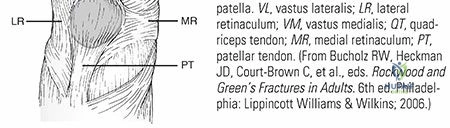
The medial and lateral extensor retinacula are robust longitudinal expansions of the vastus medialis and vastus lateralis aponeuroses, bypassing the patella to insert directly onto the proximal tibia. The preservation of these structures is critical; if they remain intact despite a transverse patella fracture, the patient may still demonstrate active straight-leg raise capabilities.
Biomechanically, the patella functions as a fulcrum. It displaces the extensor mechanism anteriorly away from the center of rotation of the knee joint, thereby increasing the mechanical advantage and moment arm of the quadriceps muscle by up to 30% to 50%. Furthermore, it aids in the nourishment of the distal femoral articular cartilage and acts as a bony shield protecting the femoral condyles from direct anterior trauma.
The vascular supply to the patella is precarious and clinically relevant. It arises from an extraosseous anastomotic ring formed by the supreme genicular, medial superior genicular, medial inferior genicular, lateral superior genicular, lateral inferior genicular, and anterior tibial recurrent arteries. The intraosseous blood supply enters primarily at the distal pole and courses proximally. Consequently, displaced transverse fractures significantly disrupt the blood supply to the proximal fragment, increasing the risk of avascular necrosis (AVN) or nonunion.
Clinical Evaluation and Radiographic Assessment
Patients typically present with an acute loss of ambulatory capacity, accompanied by significant hemarthrosis, focal swelling, and exquisite tenderness over the anterior knee. A palpable osseous defect or "gap" is often appreciated, particularly in displaced transverse fractures.
A meticulous soft tissue examination is mandatory to rule out open fractures, which constitute a surgical urgency. In cases of traumatic lacerations near the joint, a saline load test must be performed. This involves the intra-articular injection of at least 100 to 150 mL of sterile normal saline (often mixed with methylene blue) through an uncompromised portal to assess for extravasation through the traumatic wound, confirming an open joint.
Active knee extension must be formally evaluated to determine the integrity of the retinacular expansions. In the setting of severe pain and hemarthrosis, a straight-leg raise test may be falsely negative due to pain inhibition. This can be mitigated by performing an intra-articular aspiration of the hematoma followed by the injection of 10 to 20 mL of 1% lidocaine to provide local analgesia.
Associated injuries must be excluded. High-energy trauma necessitates a comprehensive evaluation of the ipsilateral hip, femur, tibia, and ankle to rule out concomitant fractures or ligamentous disruptions.
Standard radiographic evaluation mandates orthogonal views:
* Anteroposterior View: Useful for identifying vertical fracture patterns and assessing overall alignment. A bipartite patella (present in 8% of the population) may be mistaken for a fracture. It is typically located in the superolateral quadrant, features smooth, sclerotic margins, and is bilateral in 50% of cases.
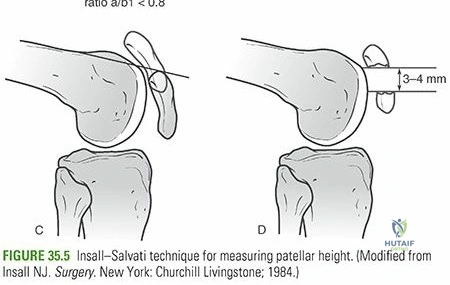
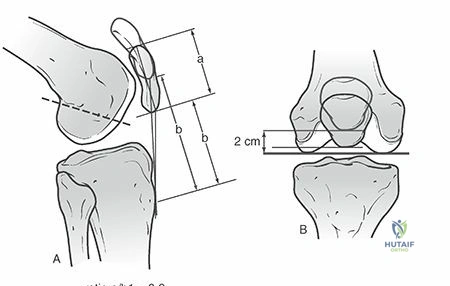
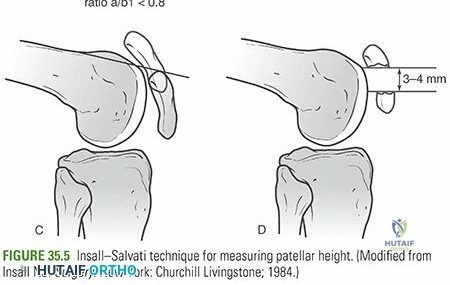
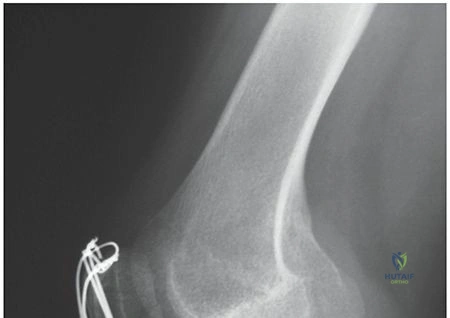
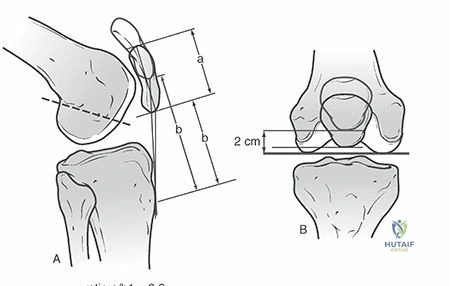
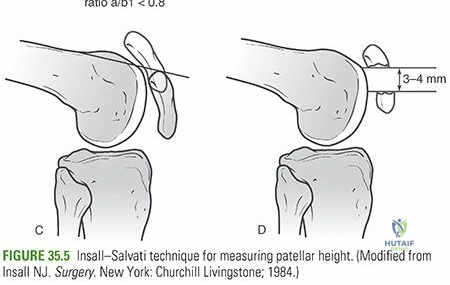
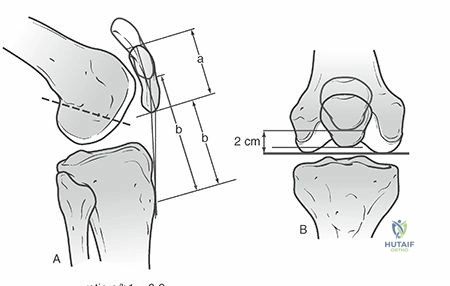
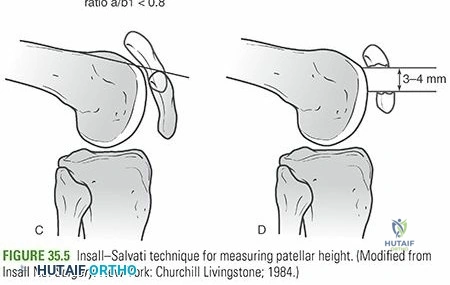
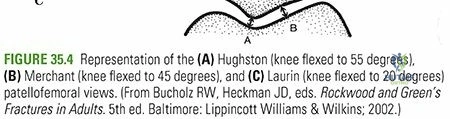
* Lateral View: The most critical view for assessing fracture displacement, articular step-off, and comminution. Insall-Salvati ratios can be calculated to assess for patella alta or baja, though acute trauma alters resting tendon length.
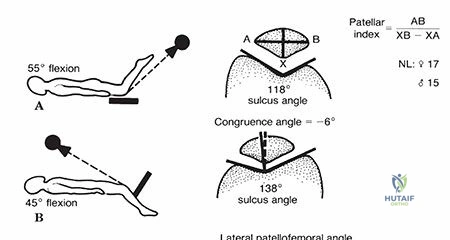
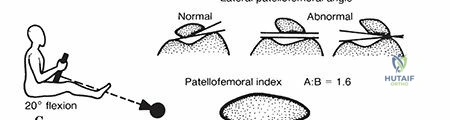
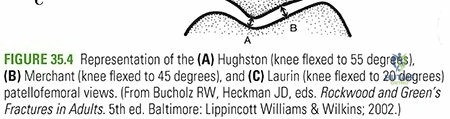
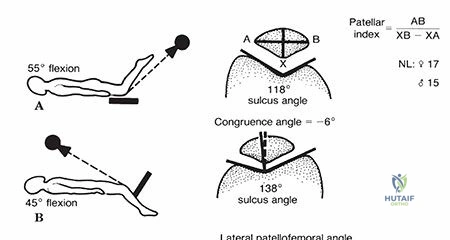
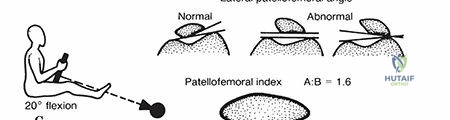
* Axial View: This view is critical for evaluating vertical fracture patterns, marginal osteochondral fractures, and assessing the congruity of the patellofemoral articulation.
Advanced imaging, such as Computed Tomography (CT), is increasingly utilized for surgical planning in the setting of highly comminuted fractures, distal pole fractures, or when assessing for occult osteochondral shearing injuries of the femoral trochlea.
Indications and Contraindications
The decision algorithm for operative versus non-operative management hinges on the integrity of the extensor mechanism, the degree of articular incongruity, and the overall functional demands of the patient.
| Management Strategy | Primary Indications | Relative Contraindications |
|---|---|---|
| Non-Operative | Intact extensor mechanism (positive straight leg raise) Articular step-off < 2 mm Fracture displacement < 3 mm Vertical or non-displaced stellate fractures |
Open fractures Loss of active extension Displaced intra-articular loose bodies |
| Operative | Disrupted extensor mechanism (inability to perform SLR) Articular step-off > 2 mm Fracture displacement > 3 mm Open fractures (surgical urgency) Osteochondral fractures with loose bodies |
Active soft tissue infection (absolute for internal fixation) Non-ambulatory baseline status Severe medical comorbidities precluding anesthesia |
Non-operative management typically consists of immobilization in a hinged knee brace locked in full extension or a cylinder cast for 4 to 6 weeks, with immediate weight-bearing as tolerated in extension. Frequent radiographic surveillance is required to ensure no secondary displacement occurs as swelling subsides.
Pre Operative Planning and Patient Positioning
Thorough preoperative planning involves a detailed review of all imaging modalities to anticipate the fracture pattern and select the appropriate fixation construct. The surgeon must ensure the availability of standard Kirschner wires (K-wires), cerclage wire, cannulated screws, and potentially patella-specific locking plates.
The patient is positioned supine on a radiolucent operating table. A bump may be placed under the ipsilateral hip to correct natural external rotation of the lower extremity, ensuring the patella faces directly anteriorly. A non-sterile pneumatic tourniquet is applied to the proximal thigh. The contralateral leg is padded and secured. Prophylactic intravenous antibiotics are administered within 60 minutes prior to incision. The operative extremity is prepped and draped in a standard sterile fashion, allowing for full, unrestricted flexion and extension of the knee joint. Fluoroscopy must be positioned to allow for orthogonal intraoperative views without compromising the sterile field.
Detailed Surgical Approach and Technique
Surgical Approach
A midline longitudinal incision is the standard of care. While a transverse incision may offer superior cosmesis, a longitudinal incision is strongly preferred as it is extensile and incorporates the standard approach for any potential future total knee arthroplasty. The incision extends from the superior pole of the patella to the tibial tubercle.
Full-thickness medial and lateral fasciocutaneous flaps are elevated to expose the anterior surface of the patella and the medial and lateral retinacular tears. It is imperative to maintain thick flaps to preserve the subdermal vascular plexus and minimize the risk of postoperative skin necrosis. The fracture hematoma is evacuated, and the joint is copiously irrigated to remove all intra-articular debris and small, non-viable chondral fragments.
Fracture Reduction
The fracture edges are debrided of interposed soft tissue or periosteum. The knee is fully extended to relax the quadriceps and minimize tension across the fracture site. Reduction is achieved using large, pointed reduction forceps (Weber clamps). The articular surface must be directly visualized or palpated through the medial and lateral retinacular defects to ensure absolute anatomic restoration of the chondral surface.
Tension Band Wiring Technique
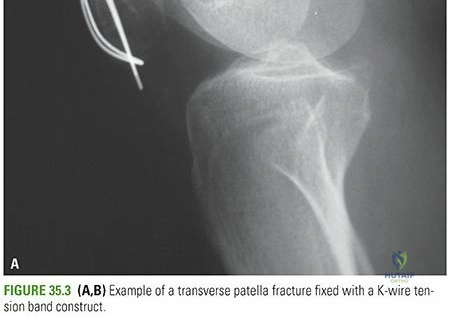
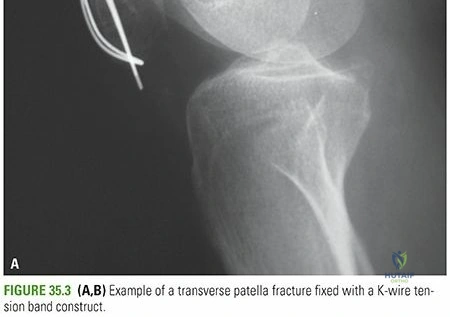
The modified anterior tension band construct remains a workhorse for simple transverse fractures. This biomechanical principle converts the tensile forces generated by the quadriceps during knee flexion into compressive forces at the articular surface.
- Longitudinal Fixation: Two parallel 2.0 mm or 2.4 mm K-wires are driven from the superior pole to the inferior pole, perpendicular to the fracture line. They should be positioned in the anterior half of the patella to maximize the tension band effect.
- Cerclage Wire Passage: An 18-gauge stainless steel cerclage wire is passed in a figure-of-eight fashion over the anterior surface of the patella, anchoring deep to the K-wires at both the superior and inferior poles. Passing the wire through the quadriceps and patellar tendons immediately adjacent to the bone is critical to prevent wire migration.
- Tensioning: The cerclage wire is tensioned symmetrically using dual wire tighteners. Ensure the twists are laid flat against the retinaculum to minimize soft tissue irritation.
- K-wire Management: The K-wires are bent, cut short, and rotated so the ends are buried deep into the quadriceps tendon superiorly and the patellar tendon inferiorly.
Cannulated Screw Tension Band Construct
Biomechanical studies have demonstrated that substituting K-wires with parallel cannulated screws (typically 4.0 mm or 4.5 mm) significantly increases the construct's resistance to gap formation.
1. Guide wires are placed parallel across the reduced fracture.
2. The screws are inserted over the guide wires.
3. The 18-gauge cerclage wire is passed through the cannulae of the screws and crossed in a figure-of-eight fashion over the anterior surface before tensioning.
Partial Patellectomy
Indicated for fractures with severe comminution of the superior or inferior pole where stable internal fixation is impossible.
1. The comminuted fragments are excised.
2. The articular edge of the remaining major fragment is smoothed to prevent chondral abrasion against the trochlea.
3. The patellar or quadriceps tendon is reattached to the remaining bone using heavy, non-absorbable sutures (e.g., #5 FiberWire) placed in a Krackow or grasping configuration.
4. The sutures are passed through three parallel longitudinal transosseous tunnels drilled in the remaining patellar fragment and tied securely at the opposite pole. Suture anchors may also be utilized as an alternative to transosseous tunnels.
Retinacular Repair
Regardless of the osseous fixation technique, the medial and lateral retinacular tears must be meticulously repaired. This is performed using heavy absorbable sutures (e.g., #1 Vicryl) in an interrupted fashion. Failure to repair the retinaculum compromises the extensor mechanism and significantly increases the risk of fixation failure.
Intraoperative fluoroscopy is utilized to confirm anatomic reduction of the articular surface and appropriate hardware placement. The knee is taken through a gentle range of motion to assess the stability of the construct under direct visualization.
Complications and Management
Patellar fractures, given their subcutaneous location and high biomechanical demands, are associated with a significant complication profile.
| Complication | Estimated Incidence | Etiology and Pathophysiology | Salvage and Management Strategy |
|---|---|---|---|
| Symptomatic Hardware | 30% - 50% | Prominent K-wires or cerclage knots irritating the subcutaneous tissues. Most common complication. | Hardware removal after radiographic confirmation of solid bony union (typically > 6-12 months post-op). |
| Loss of Reduction / Fixation Failure | 5% - 20% | Inadequate initial fixation, unrecognized comminution, patient non-compliance, or failure to repair retinaculum. | Revision open reduction and internal fixation (ORIF). May require transition from TBW to plate osteosynthesis or partial patellectomy. |
| Knee Stiffness (Arthrofibrosis) | 10% - 30% | Prolonged immobilization, excessive surgical trauma, or intra-articular adhesions. | Aggressive physical therapy. Manipulation under anesthesia (MUA) or arthroscopic lysis of adhesions if no progress by 3-4 months. |
| Infection | 2% - 10% | Subcutaneous nature of bone, thin soft tissue envelope, high rate of open fractures. | Superficial: Oral antibiotics. Deep: Urgent surgical debridement, hardware retention (if stable), IV antibiotics. Hardware removal if union achieved. |
| Nonunion | 1% - 5% | Inadequate fixation, avascularity of proximal pole, infection. | Revision ORIF with bone grafting. Partial or total patellectomy in severe, recalcitrant cases. |
| Avascular Necrosis (AVN) | Up to 25% (proximal pole) | Disruption of the distal-to-proximal intraosseous blood supply in transverse fractures. | Often asymptomatic and requires no treatment. If symptomatic and fragmented, partial patellectomy may be indicated. |
Total patellectomy is considered a salvage procedure of last resort. It results in a permanent 50% reduction in quadriceps strength, extensor lag, and profound alterations in patellofemoral tracking.
Post Operative Rehabilitation Protocols
The postoperative rehabilitation protocol must balance the protection of the surgical construct with the prevention of arthrofibrosis. Protocols vary based on the security of the fixation achieved intraoperatively.
Phase 1: Immediate Postoperative (0 to 2 Weeks)
- Immobilization: The knee is placed in a hinged knee brace locked in full extension.
- Weight-Bearing: Weight-bearing as tolerated (WBAT) with crutches, keeping the brace locked in extension to prevent eccentric loading of the quadriceps.
- Range of Motion: Depending on intraoperative stability, passive range of motion (PROM) from 0 to 30 degrees may be initiated under the guidance of a physical therapist. Active straight leg raises are permitted to maintain quadriceps tone.
Phase 2: Early Motion (2 to 6 Weeks)
- Immobilization: Continue brace use.
- Range of Motion: Progressive increase in flexion. The goal is to advance flexion by 15 to 30 degrees per week, aiming for 90 degrees of flexion by week 6. Active extension is initiated but strictly without resistance.
- Weight-Bearing: Continue WBAT in extension.
Phase 3: Strengthening (6 to 12 Weeks)
- Clinical Milestone: Radiographic evidence of progressive fracture consolidation.
- Immobilization: The brace is gradually unlocked for ambulation and eventually discontinued once the patient demonstrates excellent quadriceps control and no extensor lag.
- Range of Motion: Progression to full, symmetric range of motion.
- Strengthening: Introduction of closed kinetic chain exercises (e.g., mini-squats, leg presses). Open kinetic chain extension against resistance is delayed until complete bony union is confirmed.
Phase 4: Return to Function (3+ Months)
- Progression to sport-specific or work-specific functional training.
- Full return to heavy labor or contact sports is typically achieved between 4 to 6 months postoperatively, contingent upon symmetric quadriceps strength and complete radiographic union.
Summary of Key Literature and Guidelines
The management of patellar fractures is heavily guided by biomechanical research and consensus guidelines regarding periarticular trauma.
Biomechanical Superiority of Fixation Constructs:
Classic biomechanical studies, notably by Carpenter et al., have definitively demonstrated that the use of cannulated screws combined with a tension band wire provides superior resistance to fracture gap formation compared to traditional modified anterior tension band wiring using K-wires. The screw construct provides rigid interfragmentary compression, while the wire neutralizes tensile forces. Recent literature has also highlighted the utility of anterior locking plates for highly comminuted fractures, showing comparable or superior biomechanical profiles to tension band constructs, particularly in multi-fragmentary patterns.
Management of Open Fractures:
Guidelines from the Orthopaedic Trauma Association (OTA) and the British Orthopaedic Association Standards for Trauma (BOAST) dictate that open patellar fractures require urgent intravenous antibiotics, tetanus prophylaxis, and operative debridement. The timing of internal fixation depends on the degree of contamination and the viability of the soft tissue envelope. Immediate internal fixation is acceptable following thorough debridement in clean, low-energy open fractures.
Operative vs. Non-Operative Outcomes:
Long-term outcome studies indicate that while operative intervention reliably restores the extensor mechanism, patients frequently experience residual deficits. Up to 50% of patients report some degree of anterior knee pain or weather-related aching at long-term follow-up. Furthermore, the high incidence of symptomatic hardware removal underscores the need for meticulous surgical technique and careful patient counseling regarding the potential for secondary surgical interventions. The preservation of the patella, even in comminuted patterns, remains paramount, as the functional detriments of total patellectomy are severe and largely irreversible.
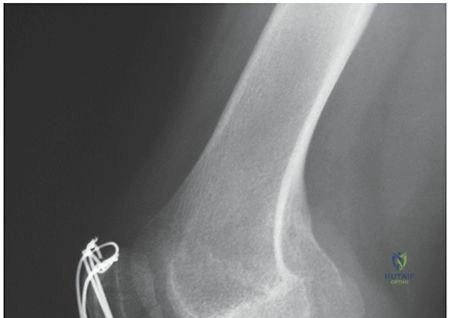
Clinical & Radiographic Imaging