Orthopedic Prometric Exam Preparation MCQs - Part 4

Orthopedic Prometric Exam Preparation MCQs - Part 4
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Which of the following procedures is not indicated as part of the reconstruction of the cavovarus hindfoot:
Explanation
Question 2
Transfer of the extensor hallucis longus tendon to the first metatarsal and arthrodesis of the hallux interphalangeal joint is indicated for which of the following deformities:
Explanation
Question 3
A 43-year-old diabetic patient has had an ulcer on the plantar aspect of her foot for 9 months. She has no systemic symptoms. There is minimal drainage from the ulcer, and she has no pain in the foot. Initial management of this patient must include:
Explanation
Question 4
The primary cause for the deformity shown (Slide) is:
Explanation
Question 5
A patient had a fixed deformity of the hallux interphalangeal (IP) joint (Slide) for 3 years following forefoot surgery. She complains of pain over the distal aspect of the hallux where rubbing occurs on the shoe. On examination, the hallux is flexible at the metatarsophalangeal (MP) and IP joints, there is no crepitus of the MP joint, and radiographs demonstrate normal alignment of the first metatarsal. The recommended procedure for correcting this deformity is:

Explanation
Question 6
A 33-year-old recreational athlete presents for treatment of chronic ankle pain. He recalls multiple ankle sprains that occurred 10 years ago. He has not undergone any surgical treatment. On examination, his ankle is stable, there is no crepitus on range of motion, and pain is present to palpation of the posterior ankle. A computerized axial tomography is presented (Slide). The surgical procedure most consistent with a rapid recovery and predictable outcome is:
Explanation
Question 7
A 52-year-old man presents for treatment of acute pain in the forefoot. He notes that the onset of pain started 24 hours ago, and he is unable to walk. Examination of the hallux (Slide) is uncomfortable. The recommended treatment for this condition is:
Explanation
This patient presents with a classic acute gout attack. Although the hallux is in severe valgus, it is unlikely that this is the cause of the joint pain. Note the swelling of the hallux and the shiny skin from the acute inflammation. These clinical findings are typical of gout. Intra-articular injection of steroids is effective treatment and can be combined with oral anti-inflammatory agents.
Question 8
A 43-year-old patient presents for treatment of a chronically painful ankle. He notes pain with ambulation, is unable to exercise, and has had marked swelling of the ankle for the last 6 months. When walking, he notes continued instability of the ankle. Examination of the ankle is unremarkable with the exception of swelling. A plain radiograph and intraoperative photograph are shown (Slide 1 and Slide 2). The most likely cause for this condition is:

Explanation
Question 9
A patient sustains a crush injury when heavy farm equipment rolls over his foot. He presents to the emergency department 4 hours later with pain and swelling in the foot. Radiographic examination is normal. You examine him for a compartment syndrome. The intracompartmental pressure in the interosseous compartment is 20 mm Hg. The next phase of management may include all of the following except:
Explanation
Question 10
A 61-year-old woman presents for treatment of a painful ankle. She reports that 4 years ago, she sustained a fracture of her ankle that was treated with cast immobilization. She has experienced progressively worsening pain over the past 2 years. On examination, she has good range of motion of the ankle with crepitus and pain. Radiographs are presented (Slide 1 and Slide 2). All of the following are acceptable forms of surgical correction except:

Explanation
Question 11
This patient developed a peripheral neuropathy of uncertain etiology. She has a partial peroneal nerve palsy with lack of extensor function of the hallux. She repeatedly stubs and catches the hallux when walking. Upon examination, she has good strength of the extensor digitorum longus tendon, as well as the anterior tibial tendon. Flexor strength of the foot is intact. All of the following are acceptable surgical alternatives except:
Explanation
Question 12
A 28-year-old professional athlete presents for treatment of foot pain following an inversion injury to her ankle. She has been immobilized in a short leg walker boot for 1 month with minimal relief of symptoms. On examination, pain is present in the sinus tarsi. The patientâ s ankle is not painful or unstable. Radiographs demonstrate a calcaneonavicular coalition. Recommended treatment includes:
Explanation
Question 13
A 43-year-old woman presents for treatment of pain in her forefoot that has been present for 1 year. The pain is localized to the second toe and radiates out to the tip of the toe with activities. When the patient wears high heel shoes, the pain is associated with numbness and burning of the toe. Your initial treatment consists of:
Explanation
Question 14
A 62-year-old man presents for treatment of ankle pain. He suffered a fibular fracture 7 months ago while hiking in the mountains. He was treated with a short leg walking cast. On examination, he has pain on range of motion of the ankle, pain over the distal fibula, and no instability or crepitus to range of motion of the ankle. Pain is present on external rotation of the foot under the leg. Radiographs of the ankle demonstrate a healed fibular fracture with 7 mm of shortening and slight external rotation. There is a 7° valgus tilt of the tibiotalar joint and a widening of the medial clear space. The joint space laterally appears slightly narrowed. Recommended treatment includes:
Explanation
Question 15
The most common complication following operative treatment of an acute rupture of the Achilles tendon is:
Explanation
Question 16
A 67-year-old obese patient presents for treatment of ankle pain. Twenty- five years ago, he underwent a total ankle replacement. He was asymptomatic for 15 years, and his symptoms have become intolerable. He has limited ankle motion, associated with pain in the ankle. His radiograph is presented (Slide). Which of the following is the preferred surgical procedure:

Explanation
Question 17
A 53-year-old woman presents for treatment of recurrent symptoms following excision of a third web space interdigital neuroma. She was asymptomatic for 6 months following surgery. On examination, pain is present in the third web space and reproduced with compression of the forefoot. The likelihood of a good result following revision surgery is:
Explanation
Question 18
A patient presents for treatment of a dislocated second metatarsophalangeal joint. Radiographs demonstrate the dislocation. In addition to soft tissue balancing, you perform an oblique shortening osteotomy of the second metatarsal head (Weil). The most common complication following this osteotomy is:
Explanation
Question 19
A 26-year-old professional football player presents for evaluation of ankle pain. He was playing in a match 2 days ago and felt a pop in his ankle. On examination, the peroneal tendon is felt to subluxate anterior to the fibula. Magnetic resonance imaging confirms a tear of the superior peroneal retinaculum. Recommended treatment includes:
Explanation
Question 20
A patient presents for treatment of a painful hallux. The pain is over the dorsal surface of the hallux metatarsophalangeal joint and is worsened with plantar flexion of the toe. The passive range of motion is 30° of dorsiflexion and 10° of plantarflexion. The radiographs confirm the presence of mild arthritis of the metatarsophalangeal joint, with dorsal osteophytes on the metatarsal head. Which of the following procedures is most likely to be associated with a long-term satisfactory outcome:
Explanation
Question 21
This patient is a 17-year-old athlete who presents for treatment of a feeling of giving way of the ankle. The inversion clinical stress is demonstrated below (Slide). Which statement concerning the image presented below is correct:
Explanation
 Although some laxity may be present in this patient, it is impossible to determine whether this is present in the ankle or the subtalar joint based upon this clinical test. Simple inversion stress without simultaneously palpating the lateral shoulder of the talus cannot indicate the presence or the type of instability. An anterior drawer that is positive and, in particular, is associated with a vacuum phenomenon in the anterolateral ankle is more diagnostic of ankle instability.
Although some laxity may be present in this patient, it is impossible to determine whether this is present in the ankle or the subtalar joint based upon this clinical test. Simple inversion stress without simultaneously palpating the lateral shoulder of the talus cannot indicate the presence or the type of instability. An anterior drawer that is positive and, in particular, is associated with a vacuum phenomenon in the anterolateral ankle is more diagnostic of ankle instability.
Question 22
What structure is held in between the forceps in this photograph (Slide):
Explanation
 The extensor retinaculum is an important structure in maintaining and possibly augmenting the stability of the lateral ankle and subtalar joint. The inferior root of the extensor retinaculum inserts in the floor of the sinus tarsi, improving stability of the subtalar joint. This structure can be used to augment a repair of ankle instability.
The extensor retinaculum is an important structure in maintaining and possibly augmenting the stability of the lateral ankle and subtalar joint. The inferior root of the extensor retinaculum inserts in the floor of the sinus tarsi, improving stability of the subtalar joint. This structure can be used to augment a repair of ankle instability.
Question 23
A 37-year-old woman injured her ankle 17 weeks ago when stepping off a sidewalk. She has experienced pain in the ankle since that time, and no treatment has yet been initiated. Presented is a view of the ankle performed with external rotation stress (Slide). The recommended treatment at this time is:
Explanation
Question 24
A 42-year-old male patient presents with a history of repeated giving way of his ankle. He notes that this has been present for 1 year. He does not experience any pain, even with the episodic bouts of the ankle buckling. On examination, the ankle range of motion is normal, no pain is elicited, and there is no crepitus. A stress radiograph (Slide 1) and a lateral weight- bearing radiograph (Slide 2) are presented. The patient does not want to undergo surgery, but he needs to know the possibility of problems with his ankle in the future. The patient should be advised that:

Explanation
Question 25
A 73-year-old woman states that she has been tripping over her right foot for the past year (Slide). She walks with a limp, and she states that her foot â slapsâ the ground. On examination, weakness in which muscle is likely present:
Explanation
Question 26
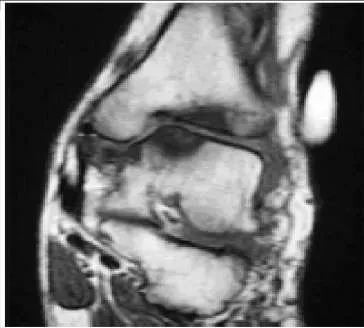
A 76-year-old man has experienced aching in the anterior aspect of his ankle for 6 months. He felt a sudden onset of soreness 6 months ago. Since then, he has noted weakness of the foot. He walks with a limp, and the foot hits the ground during the heel contact phase of gait. On examination there is a mobile subcutaneous mass in the anterior ankle. The patientâ s magnetic resonance image (MRI) is presented (Slide). Which of the following is the most accurate diagnosis:

Explanation
Question 27
A 23-year-old carpenter fell off a roof 4 weeks ago. He has pain in the ankle and a deformity. The lateral radiograph is presented (Slide). Which of the following treatments is most likely to return this patient to work with a functioning foot and ankle:
Explanation
 with early arthrodesis, which should be combined with an open reduction internal fixation of the calcaneus.
with early arthrodesis, which should be combined with an open reduction internal fixation of the calcaneus.
Question 28
A patient underwent an arthrodesis of the hallux metatarsophalangeal joint for correction of painful arthritis (Slide 1 and Slide 2). She remains symptomatic and cannot walk without pain. The most likely cause for her pain is:
Explanation
Question 29
A 53-year-old woman presents for treatment of painful toe and metatarsal deformities (Slide). She underwent surgery to the hallux 2 years ago for correction of arthritis of the hallux metatarsophalangeal joint. Pain in the joint persists. She has no systemic disease, and the opposite foot is normal. What is the ideal surgical correction for her forefoot:

Explanation
Question 30
A 17-year-old patient presents with pain in the second toe. Pain becomes worse with exercise and has been present for 6 months. On examination, swelling is present around the metatarsophalangeal joint, and pain is present over the joint and upon squeezing the forefoot. Radiographic evaluation demonstrates a lucency in the second metatarsal head. The most likely cause of this condition is:
Explanation
Question 31
An 11-year-old girl presents with chronic foot pain. Her mother notes that her daughter has had flatfeet since birth, but the condition is worsening. The patient has aching in her foot, the arch of her foot, and her leg with walking and activities. She has been treated for 3 years with various orthotic arch supports. The foot is mobile and flexible on examination. Radiographs (Slide 1 and Slide 2) and a photograph (Slide 3) of her foot are presented. Which of the following surgical treatment alternatives is unacceptable in this patient:
Explanation

Question 32
A 12-year-old girl was successfully treated for a flexible flatfoot deformity on the left foot. A clinical photograph (Slide 1) of her foot and a lateral radiograph (Slide 2) are presented. What is the purpose of the implant noted under the talus in the radiograph:
Explanation
 motion further. This procedure is indicated for a patient who has a flexible flatfoot deformity and can be used either as the sole or an adjunctive procedure for correction.
motion further. This procedure is indicated for a patient who has a flexible flatfoot deformity and can be used either as the sole or an adjunctive procedure for correction.
Question 33
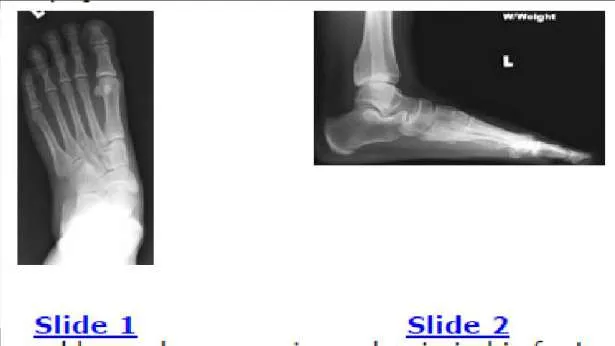
The patient presented (Slide 1 and Slide 2) has a hereditary sensory motor neuropathy. Based upon the photographs, a surgeon should be able to determine the pattern of muscle weakness. Weakness in which muscle is most likely the cause of this deformity:
Explanation
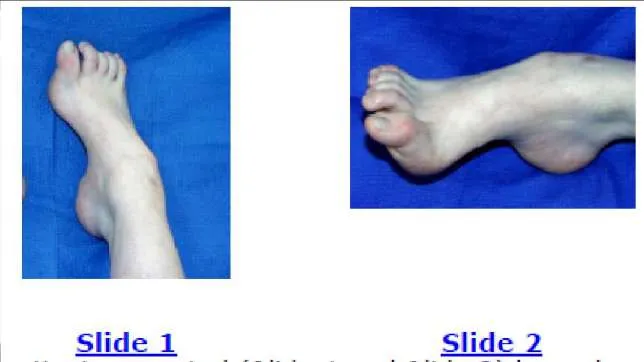 Although the anterior tibial muscle is weak, the cavus is the predominant deformity of this condition, caused by weakness of the peroneus brevis. The peroneus longus is functioning and is responsible for the plantarflexion of the first metatarsal.
Although the anterior tibial muscle is weak, the cavus is the predominant deformity of this condition, caused by weakness of the peroneus brevis. The peroneus longus is functioning and is responsible for the plantarflexion of the first metatarsal.
Question 34
You are planning a tendon transfer to help correct deformity in a patient with hereditary sensory motor neuropathy. Which of the following muscles will be used for the transfer based upon the clinical appearance of the foot (Slide 1 and Slide 2):
Explanation
Question 35
Which combination of muscle weakness is typically associated with hereditary sensory motor neuropathy:
Explanation
Question 36
A 42-year-old man with diabetes presents for treatment of a swollen foot (Slide). He does not recall the onset of swelling, and he states that his foot is not painful. On examination, the foot is hot to touch and swollen. Upon radiographic examination, no deformities are evident. Which of the following treatment options should be used next:
Explanation
Question 37
A 29-year-old woman presents for treatment of a swollen foot. Although her foot is not painful, it has been swollen for 2 weeks. The patient walks into the office without any assistive device. On examination, the foot is swollen and warm. The patient does not have protective sensation in the foot, and she denies a history of diabetes and does not have a clinically relevant medical history. A radiograph of her foot is presented (Slide). Which of the following tests will be most helpful in determining the etiology of her condition:

Explanation
Question 38
A patient with diabetes and severe peripheral neuropathy has been treated for a C harcot ankle deformity for 9 months (Slide 1, Slide 2, and Slide 3). An ankle foot orthosis has been used for 4 months. No skin breakdown occurred in the brace. Swelling is present but has decreased over the past month. Ankle range of motion is limited, and crepitus is present upon examination of the ankle. Which surgical procedure is most consistent with the future treatment of this patient:

Explanation
Question 39
An 83-year-old woman presents for treatment of a painful second toe deformity. The hallux, the bunion, and the third toe are not painful. A fixed crossover toe deformity is present (Slide), with a dislocation of the second metatarsophalangeal joint noted radiographically. Which procedure is likely to give the patient rapid pain relief:
Explanation

Question 40
A 60-year-old man experiences pain under the lesser metatarsal heads. Prominence of the metatarsal heads under the second, third, and fourth metatarsal is noted, as well as associated fixed claw toe deformities (Slide). The etiology of the foot pain is:
Explanation

Question 41
A patient presents with a claw toe deformity (Slide). What is the strongest flexor of the metatarsophalangeal joint, which in this patient is not functioning adequately:
Explanation
 Although the long and short flexor tendons have some effect albeit indirect on the flexion of the metatarsophalangeal joint, the flexor that acts directly on the joint is the interosseous muscle. Intrinsic atrophy will lead to claw toe deformity.
Although the long and short flexor tendons have some effect albeit indirect on the flexion of the metatarsophalangeal joint, the flexor that acts directly on the joint is the interosseous muscle. Intrinsic atrophy will lead to claw toe deformity.
Question 42
A 54-year-old woman presents for treatment of an ulcer (Slide). She has diabetes, no protective sensation, and slight deformity of the foot. There is no inflammation of the foot and no purulent drainage. Slight serous oozing is present daily. Initial evaluation and treatment should consist of:
Explanation
 Ambulatory treatment for a patient with diabetes is always the preferable treatment. In this patient, there is no evidence of infection. Unless drainage is purulent and the ulcer is in contact with bone, there should be minimal concern for infection. Reconstruction of a Charcot deformity of the midfoot is only indicated following repeated failure of nonoperative treatments.
Ambulatory treatment for a patient with diabetes is always the preferable treatment. In this patient, there is no evidence of infection. Unless drainage is purulent and the ulcer is in contact with bone, there should be minimal concern for infection. Reconstruction of a Charcot deformity of the midfoot is only indicated following repeated failure of nonoperative treatments.
Question 43
A 63-year-old patient underwent a triple arthrodesis for correction of flatfoot deformity. He presents with continued ankle pain, as well as a hindfoot valgus deformity. The ankle deformity is flexible, and the joint can be reduced. All of the following are reasonable surgical alternatives as a single or staged procedure with the exception of:
Explanation
Question 44
A 34-year-old patient presents for treatment of painful ankle arthritis. Deformity of the ankle is present with posttraumatic arthritis and 20° of varus deformity as a result of erosion of the distal tibial plafond. There is minimal motion of the subtalar joint, and the forefoot is plantigrade. You plan an ankle arthrodesis. In addition to the position of the ankle arthrodesis, what additional procedure should you consider:
Explanation
Question 45
A 26-year-old woman presents for treatment of ankle arthritis following trauma. She is an active individual despite her arthritis. On examination, her foot is fixed in equinus, no ankle motion is present, and the motion in the subtalar joint is normal. Ankle arthritis is noted radiographically. In a preoperative discussion, she states the desire to have as mobile a foot as possible, wear high heel shoes, and participate in realistic exercise activities. You perform an ankle arthrodesis. What is the ideal position for the arthrodesis:
Explanation
Question 46
A 22-year-old man has experienced pain in his foot and ankle for 10 years. His radiographs are presented (Slide 1 and Slide 2). The foot is flexible, and pain is present in the sinus tarsi and along the medial border of the foot. With the subtalar joint held in a reduced neutral position, the forefoot is in 15° of supination. You attempt orthotic arch supports and when these do not alleviate his pain, a brace is suggested. He refuses to wear a brace. You plan an osteotomy of the calcaneus with lengthening bone graft at the neck of the calcaneus (lateral column lengthening). The most common complication following this procedure is:
Explanation
Question 47
A 44-year-old obese man presents for treatment of acute ankle pain. He does not have a history of trauma or a systemic history of note. His opposite foot has had multiple episodes of acute pain in the past, lasting from 3 to 5 days. On examination, the ankle is warm, swollen, and exquisitely tender to palpation and any range of motion (Slide1, Slide 2, and Slide 3). Concerned about the source of pain, you aspirate the joint and send the sample for analysis. You expect to find:
Explanation

Question 48
This patient presents for treatment of a painful hallux varus deformity following correction of hallux valgus deformity (Slide). All of the following procedures may be acceptable surgical alternatives for correction of deformity with the exception of:
Explanation
 correction of a fixed claw deformity of the interphalangeal joint, usually in conjunction with a tendon transfer. Arthrodesis of the metatarsophalangeal joint is a reasonable alternative provided there is no fixed deformity of the interphalangeal joint present and when arthritis or fixed deformity of the metatarsophalangeal joint is present.C orrect Answer: First metatarsal osteotomy
correction of a fixed claw deformity of the interphalangeal joint, usually in conjunction with a tendon transfer. Arthrodesis of the metatarsophalangeal joint is a reasonable alternative provided there is no fixed deformity of the interphalangeal joint present and when arthritis or fixed deformity of the metatarsophalangeal joint is present.C orrect Answer: First metatarsal osteotomy
Question 49
Which of the following is true concerning Achilles tendon ruptures:
Explanation
Question 50
Which of the following is true concerning the repair of acute Achilles tendon ruptures:
Explanation
Question 51
A 55-year-old diabetic patient presents with a warm, swollen, erythematous foot without an open wound. Radiographs show fragmentation of the navicular and cuneiforms. Which of the following is the most appropriate initial management?
Explanation
Question 52
A 40-year-old man sustains a high-energy varus directed force to his knee resulting in a medial tibial plateau fracture.
Which of the following associated neurovascular injuries is most frequently seen with this specific high-energy fracture pattern compared to lateral plateau injuries?
Explanation
Question 53
Which of the following is an accepted indication for prophylactic in situ pinning of the contralateral asymptomatic hip in a patient presenting with an acute slipped capital femoral epiphysis (SCFE)?
Explanation
Question 54
A 65-year-old man presents with bilateral leg pain exacerbated by walking and relieved by sitting and leaning forward. He reports that riding a stationary bicycle does not provoke his symptoms. What is the most likely pathophysiological mechanism of his symptoms?
Explanation
Question 55
A 32-year-old manual laborer presents with dorsal wrist pain and decreased grip strength. Radiographs reveal sclerosis and early fragmentation of the lunate, with negative ulnar variance, but no carpal collapse.
What is the most appropriate surgical intervention?
Explanation
Question 56
During an anterior cruciate ligament (ACL) reconstruction using a bone-patellar tendon-bone (BPTB) autograft, the surgeon must be aware that this graft has a higher incidence of which of the following postoperative complications compared to a hamstring autograft?
Explanation
Question 57
Which of the following bearing surface combinations in total hip arthroplasty historically demonstrates the lowest volumetric wear rate?
Explanation
Question 58
Bone morphogenetic protein-2 (BMP-2) and BMP-7 promote bone healing primarily through which of the following molecular intracellular pathways?
Explanation
Question 59
According to the Ponseti method for the treatment of idiopathic clubfoot, what is the correct sequence of deformity correction?
Explanation
Question 60
A 28-year-old motorcyclist is brought to the ED after a collision. Pelvic radiographs show a symphyseal diastasis of 3.5 cm and widening of the anterior sacroiliac joints bilaterally.
Which ligamentous structures are completely ruptured in this injury?
Explanation
Question 61
In a patient diagnosed with high-grade conventional intramedullary osteosarcoma, which of the following represents the most significant prognostic factor for long-term survival?
Explanation
Question 62
During a posterior-stabilized total knee arthroplasty, the surgeon notes that the knee is tight in flexion and well-balanced in extension. Which of the following maneuvers is most appropriate to balance the knee?
Explanation
Question 63
A 30-year-old man sustains a closed tibial shaft fracture. Twelve hours later, he complains of severe leg pain out of proportion to the injury. Which of the following physical examination findings is the most sensitive early clinical indicator of acute compartment syndrome?
Explanation
Question 64
A 58-year-old woman presents with clumsiness of her hands, frequent tripping, and a sensation of electric shocks shooting down her spine upon neck flexion (Lhermitte's sign). Physical examination reveals a positive Hoffmann's sign bilaterally. What is the most appropriate next step in diagnosis?
Explanation
Question 65
A 24-year-old carpenter suffers a laceration over the volar aspect of his proximal phalanx of the index finger, resulting in an inability to flex both the PIP and DIP joints.
Which of the following accurately describes the anatomical flexor tendon zone of this injury?
Explanation
Question 66
A 22-year-old overhead athlete sustains an acute anterior shoulder dislocation. After reduction, an MRI arthrogram reveals an avulsion of the anterior-inferior labrum along with the anterior band of the inferior glenohumeral ligament (IGHL). What is the specific name of this lesion?
Explanation
Question 67
In evaluating an ankle fracture for syndesmotic instability, which radiographic parameter on a standard AP or mortise view is most indicative of a syndesmotic injury?
Explanation
Question 68
A 4-week-old female infant is diagnosed with developmental dysplasia of the hip (DDH) and placed in a Pavlik harness. Two weeks later, she presents with decreased active extension of her knee, though she still kicks her foot. What complication has most likely occurred?
Explanation
Question 69
A 6-year-old child sustains a completely displaced extension-type supracondylar fracture of the humerus. Examination reveals inability to flex the interphalangeal joint of the thumb and the distal interphalangeal joint of the index finger. Which nerve is most likely injured?
Explanation
Question 70
A 3-month-old girl has a persistent dislocated hip after 4 weeks of Pavlik harness treatment for developmental dysplasia of the hip. What is the most appropriate next step in management?
Explanation
Question 71
A 45-year-old man presents with a Schatzker type II tibial plateau fracture. Which of the following surgical approaches is most commonly utilized for open reduction and internal fixation of this injury?
Explanation
Question 72
During an ACL reconstruction using a bone-patellar tendon-bone autograft, the surgeon notes a minor mismatch between the graft length and the tunnel length, leading to graft protrusion from the femoral tunnel. Which maneuver is best to resolve a minor (2-3 mm) mismatch?
Explanation
Question 73
A 35-year-old male presents with severe lower back pain, saddle anesthesia, and acute urinary retention. MRI reveals a massive L4-L5 disc herniation. What is the most critical prognostic factor for neurological recovery?
Explanation
Question 74
A 25-year-old carpenter lacerates his volar index finger at the level of the proximal phalanx, cutting both the FDS and FDP tendons. This injury corresponds to which flexor tendon zone?
Explanation
Question 75
A 72-year-old female presents with chronic shoulder pain and pseudoparalysis. Radiographs show superior migration of the humeral head and an acromiohumeral interval of 3 mm. Which treatment provides the best predictable outcomes for this specific condition?
Explanation
Question 76
An obese 13-year-old boy presents with right knee pain and a limp. Examination shows obligatory external rotation of the right hip during passive flexion. What is the most appropriate definitive management?
Explanation
Question 77
A 55-year-old diabetic patient presents with a swollen, erythematous, and warm left foot. There are no open ulcers. Radiographs show soft tissue swelling but no acute fractures. What is the most appropriate initial management?
Explanation
Question 78
A biopsy of a destructive, lytic bone lesion in the diaphysis of the femur of a 15-year-old boy shows sheets of uniform, small round blue cells. Cytogenetic analysis reveals a t(11;22) translocation. What is the most likely diagnosis?
Explanation
Question 79
A 28-year-old male sustains a closed tibia fracture. Hours later, he develops severe pain out of proportion to the injury. Intracompartmental pressure testing is performed. Which measurement is generally considered the threshold indicating the need for emergent fasciotomy?
Explanation
Question 80
According to the Ponseti method for congenital talipes equinovarus (clubfoot), which component of the deformity is typically corrected last?
Explanation
Question 81
A 45-year-old highly active male is undergoing a total hip arthroplasty. To minimize wear rates and the risk of osteolysis, which of the following bearing surface combinations is most appropriate?
Explanation
Question 82
A 30-year-old motorcyclist sustains an anteroposterior compression (APC) type III pelvic ring injury. What is the most common primary source of life-threatening hemorrhage in this specific injury pattern?
Explanation
Question 83
A patient complains of numbness in the thumb, index, and middle fingers. Symptoms are exacerbated by tapping over the volar wrist. Which nerve is compressed, and in which anatomical space?
Explanation
Question 84
A 24-year-old football player sustains a hyperplantarflexion injury to his midfoot. Radiographs show widening of the space between the medial cuneiform and the base of the second metatarsal. What is the primary stabilizing structure injured?
Explanation
Question 85
A 14-year-old gymnast presents with chronic low back pain. Radiographs reveal a pars interarticularis defect with a 25% forward slip of L5 on S1. According to the Meyerding classification, what is the grade of this spondylolisthesis?
Explanation
Question 86
One year following a posterior-stabilized total knee arthroplasty, a patient presents with a painful popping sensation when extending the knee from a flexed position. What is the most likely etiology?
Explanation
Question 87
A 20-year-old male suffers a traumatic anterior shoulder dislocation. Post-reduction radiographs show a posterolateral humeral head impaction fracture. What is the eponym for this specific lesion?

Explanation
Question 88
A 4-year-old boy presents with an acute limp, fever of 38.8°C, refusal to bear weight, and a WBC count of 14,000/mm³. According to the Kocher criteria, what is the approximate probability that this child has septic arthritis of the hip?
Explanation
Question 89
A 55-year-old female presents with medial ankle pain and a progressive flatfoot deformity. Examination reveals an inability to perform a single-leg heel rise, but the hindfoot remains flexible and correctable. Which of the following surgical interventions is most appropriate for this stage of disease?
Explanation
Question 90
During open reduction and internal fixation of a Weber C ankle fracture, the syndesmosis is reduced and clamped. Which of the following radiographic parameters best confirms accurate reduction of the syndesmosis on a standard mortise view?
Explanation
Question 91
A 22-year-old professional basketball player sustains an acute fracture of the proximal fifth metatarsal at the metaphyseal-diaphyseal junction (Zone 2). What is the most appropriate management to minimize the risk of nonunion and expedite return to play?
Explanation
Question 92
A 60-year-old patient with poorly controlled diabetes presents with a deep, non-healing plantar ulcer probing to bone. MRI confirms osteomyelitis of the first metatarsal head. Which of the following is the most definitive method to identify the causative organism and direct targeted antibiotic therapy?
Explanation
Question 93
A 45-year-old weekend warrior feels a 'pop' in his posterior ankle while playing tennis. Clinical examination reveals a positive Thompson test. If non-operative management is chosen, which of the following functional rehabilitation protocols yields outcomes most comparable to surgical repair regarding re-rupture rates?
Explanation
Question 94
A 52-year-old patient with long-standing peripheral neuropathy presents with an acutely swollen, warm, and erythematous left foot. Radiographs show no fractures or dislocations, and laboratory markers (ESR, CRP) are within normal limits. What is the most appropriate initial management?
Explanation
Question 95
A 30-year-old male sustains a severely displaced talar neck fracture following a high-speed motor vehicle collision. Disruption of which of the following blood vessels places the talar body at the highest risk for developing avascular necrosis (AVN)?
Explanation
Question 96
A 40-year-old female presents with painful bunions. Weight-bearing radiographs demonstrate a hallux valgus angle of 35 degrees and an intermetatarsal angle of 15 degrees. Clinical exam reveals gross hypermobility of the first tarsometatarsal (TMT) joint. Which of the following surgical procedures is most indicated?
Explanation
Question 97
A 48-year-old woman complains of burning pain in the plantar forefoot radiating to the third and fourth toes, worsening with tight shoes. A palpable Mulder's click is present. If standard operative treatment is performed following failed conservative measures, what is the most common post-surgical complication?
Explanation
Question 98
A 35-year-old roofer falls from a height and sustains a severely comminuted intra-articular calcaneal fracture. Which of the following radiographic findings on a lateral foot radiograph best indicates the loss of calcaneal height and collapse of the posterior facet?
Explanation
None
