Orthopedic Prometric Exam Preparation MCQs - Part 2
Orthopedic Prometric Exam Preparation MCQs - Part 2
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
While he is working, an industrial worker sustains a puncture wound to the plantar aspect of his foot. He suspects the wound was caused by a sharp protruding nail that penetrated his sneaker. The most likely organism to be responsible for a subsequent infection is:
Explanation
Question 2
A 54-year-old woman sustained an injury to her knee 16 months ago. She describes the injury as a dislocation, and she was treated with ligament reconstruction. She has plantarflexion and inversion strength, absent ankle dorsiflexion, and weak eversion. She desires an improvement in the function of the ankle and the ability to comfortably ambulate. The ideal treatment for her is:
Explanation
Question 3
A 61-year-old man has been treated for type I diabetes for 6 years and presents for evaluation and treatment of an ulcer on the plantar aspect of the forefoot. The ulcer has been present for 4 weeks. The ulcer does not appear infected, claw toe deformities are present, and a posterior tibial pulse is palpable. An important screening test for this patient is:
Explanation
Question 4
The most common complication following medial subtalar dislocation with incarceration of the talus in the extensor brevis muscle is:
Explanation
Question 5
A patient sustained a fracture of the calcaneus 9 months ago. The fracture was treated with non-weight bearing and cast immobilization. The patient experiences constant pain and is unable to work. On examination, he has limited inversion, eversion motion of the foot, and lateral foot pain. Radiographs are presented. The recommended treatment is:
Explanation
Question 6
A 44-year-old woman presents with chronic pain in the region of the forefoot. She is unable to wear a shoe with a heel and she has pain in the region of the second toe. On examination, she has swelling of the second toe and painful inflammation of the metatarsophalangeal joint. A clinical picture of her foot is presented. Your initial treatment consists of:
Explanation

Question 7
The most reliable clinical finding of an acute compartment syndrome of the foot is:
Explanation
Question 8
A 9-year-old girl presents for treatment of a calcaneus deformity of the foot that has progressively worsened over the past 3 years. She has a history of poliomyelitis. Upon examination, she has poor plantarflexion, neutral varus and valgus of the hindfoot, and strong dorsiflexion. The preferred treatment for this deformity is:
Explanation
Question 9
A 54-year-old woman presents for treatment of leg weakness. She is unable to walk up stairs. She recalls an injury to her ankle while playing tennis 1 year ago. Upon examination, she has poor plantarflexion strength, but excellent dorsiflexion and inversion strength. A magnetic resonance image of her leg is presented. The recommended treatment is:
Explanation
Question 10
A 19-year-old collegiate lacrosse player presents for treatment of acute pain along the lateral aspect of the foot. The pain developed during a preseason game 1 week ago. A radiograph is presented. The treatment that will return the athlete to playing competitively with the least likelihood of complications is:
Explanation
 junction of the metaphysis and diaphysis is preferred treatment. Although nonoperative treatment is associated with fracture healing, the limited function and requirement for immobilization, and possibly limited weight bearing, makes this alternative less appealing in the athlete.
junction of the metaphysis and diaphysis is preferred treatment. Although nonoperative treatment is associated with fracture healing, the limited function and requirement for immobilization, and possibly limited weight bearing, makes this alternative less appealing in the athlete.
Question 11
A 19-year-old woman presents for treatment of a painful hallux valgus deformity. In addition to the foot deformity, she has spastic hemiplegic cerebral palsy. A clinical picture of her foot is presented. The recommended treatment is:
Explanation
Question 12
The most common complication of arthrodesis of the proximal interphalangeal (PIP) joint is:
Explanation
Question 13
A 59-year-old woman presents for treatment of a painful hallux valgus deformity. She has a prominent bunion, normal motion of the hallux metatarsophalangeal (MP) joint, and painful callosity under the second MP joint. Radiographs of the foot are presented. The recommended treatment is:
Explanation
Question 14
In surgical correction of the adult acquired flatfoot deformity, a medial translational calcaneal osteotomy is often performed in conjunction with additional soft tissue correction medially. One of the proposed biomechanical effects of the osteotomy associated with improvement in the arch of the foot is:
Explanation
Question 15
One year ago, a patient underwent a triple arthrodesis for management of a severe foot deformity. Although the deformity of her foot is notably improved since the surgery, she has not walked comfortably and the pain is worse than it had been prior to surgery. Upon clinical examination, she is noted to have a fixed supination deformity of the forefoot and callosity under the base of the fifth metatarsal. The recommended management of this problem is:
Explanation
Question 16
A 28-year-old woman presents for treatment of pain and swelling in the foot. She had twisted her ankle 2 months ago and her initial treatment consisted of limited activity, crutches, and immobilization. Because she has not been able to wean off the crutches, she has pain in the foot radiating to the ankle and distal lateral leg. She has constant pain in the foot and the swelling appears worse than at the time of her injury. C linically, there are multiple areas of tenderness in the foot and ankle that appear swollen and sensitive to examination. The study that would be most helpful to clarify this diagnosis is:
Explanation
Question 17
A 52-year-old man presents for evaluation and treatment of a painful flatfoot deformity. While playing tennis 2 years ago, he felt a tearing sensation in his foot and ankle. Since that time, he notes that the arch of his foot has become progressively flatter. Upon examination, he has a flatfoot inability to perform a single heel rise and weak inversion strength. He desires to have this deformity corrected. At surgery, the posterior tibial tendon is grossly normal in appearance. The most likely source of his deformity is:
Explanation
Question 18
A 27-year-old man sustained an injury to his foot 2 ½ years ago when a forklift crushed his foot. He sustained a fracture dislocation of the midfoot and was treated with open reduction and internal fixation. His current complaints are burning in the foot associated with numbness over the dorsal foot surface. On examination, he has severe focal sensitivity over the dorsal foot, particularly in the first web space radiating proximally to the ankle. Radiographs demonstrate mild arthritis and anatomic reduction of the tarsometatarsal and midfoot joints. The prognosis for relief of his foot pain at this stage is:
Explanation
Question 19
A 34-year-old woman presents for treatment of pain in the hallux. She notes pain upon weight bearing and wearing high-heel shoes. Upon examination, the range of motion of the hallux metatarsophalangeal (MP) joint is 10° dorsiflexion and 30° plantarflexion, with pain upon passive dorsiflexion. Radiographs demonstrate osteophytes over the dorsal surface of the metatarsal head, maintenance of the joint space, and a metatarsal declination angle of 10°. The first metatarsal is elevated above the second metatarsal at the level of the metatarsal neck by 4 mm. The ideal procedure to correct this problem and alleviate pain is:
Explanation
Question 20
A patient experienced a nondisplaced fracture of the medial and middle cuneiforms. His nonoperative treatment consisted of cast immobilization for 2 weeks with no weight bearing permitted, followed by ambulation as tolerated. He presents for treatment 1 week later with severe swelling in the foot, stiffness of the toes, and limited motion of the hindfoot. The fracture of the cuneiforms appears healed. The ideal management of the stiffness and swelling of the foot is:
Explanation
Question 21
A 31-year-old woman presents for treatment of pain in the hallux. She has been experiencing the pain for 2 years. She notes limited motion of the hallux with pain in the joint, particularly when wearing high-heel shoes. She is unable to toe off with running activities. Upon examination, the motion in the hallux metatarsophalangeal (MP) joint is limited in dorsiflexion and radiographs demonstrate mild arthritis of the joint. She requests surgery to correct this disorder. The recommended treatment is:
Explanation
Question 22
A 17-year-old woman presents for evaluation of a painful hallux valgus deformity. She is unable to wear shoes comfortably, has pain with athletic and daily activities, and notices that the deformity is gradually worsening. Upon clinical examination, she has generalized ligamentous laxity, with motion of the hallux metatarsophalangeal (MP) joint 75° dorsiflexion and 25° plantarflexion. Motion of the first metatarsal is approximately 8° to 10° of combined dorsiflexion and plantarflexion. There is no pain to range of motion of these joints. The hallux valgus angle is 28° and the 1-2 intermetatarsal angle is 12°. The recommended treatment is:
Explanation
Question 23
An 82-year-old woman presents for treatment of a painful second toe deformity. The toe is subluxated at the metatarsophalangeal (MP) joint, and a fixed claw toe deformity is present. Despite severe hallux valgus, and the hallux under riding the second toe, the hallux and bunion are not symptomatic. The procedure that will ideally correct this deformity is:
Explanation
Question 24
A 19-year-old woman had previously been treated for hallux valgus deformity with resection of the medial eminence only. She now presents with severe recurrent deformity of the hallux, with pain. There is neither pain nor crepitus upon range of motion of the hallux metatarsophalangeal (MP) joint. The procedure that will successfully correct the deformity of the hallux and the first metatarsal and maintain motion at the MP joint is:
Explanation
Question 25
A 63-year-old woman who underwent attempted correction of a hallux valgus deformity 3 years previously presents to the office. She has pain in the hallux from dorsal abutment of the hallux on the shoe. There is no pain in the lesser toes or metatarsals. The recommended procedure to alleviate the irritation of the hallux is:

Explanation
Question 26
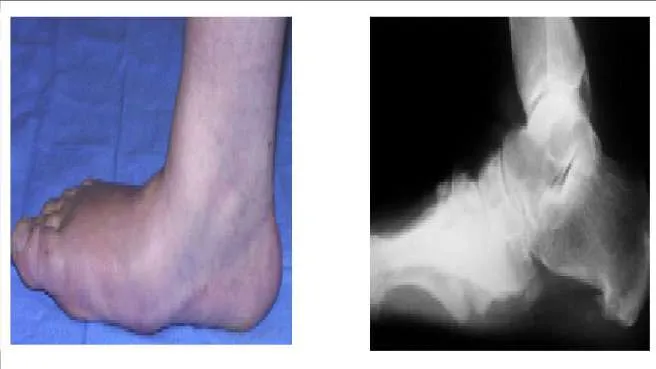
A 66-year-old woman has experienced the gradual onset of a flatfoot deformity over the past 10 years. She notes that the condition is bilateral, although worse on one side. Presented are clinical and radiographic images of her condition. This is associated with pain upon ambulation and difficulty with shoe wear. The most likely cause of this flatfoot deformity is:
Explanation
Question 27
A 66-year-old woman has experienced the gradual onset of a flatfoot deformity over the past 10 years. She notes that the condition is bilateral, although worse on one side. Presented are clinical and radiographic images of her condition. This is associated with pain upon ambulation and difficulty with shoe wear. The most likely cause of this flatfoot deformity is tarsometatarsal arthritis. The initial recommended treatment is:
Explanation
Question 28
Many materials are used in the production of orthotic arch supports. Plastizote is a material commonly used either alone or in combination. The problem with this material is:
Explanation
Question 29
A 35-year-old man has experienced ankle pain for 7 years. It is associated with giving way and progressive deformity of the foot. He notices that the foot is rolling inward and is becoming flatter. The cause of his condition is:
Explanation
Question 30
A 14-year-old boy presents for treatment of a painful foot, which has been present for 2 years. He has limited his athletic activities. He has similar symptoms in the opposite foot, although not as severe. On clinical examination, the alignment and appearance of the foot are normal; motion of the foot and ankle is good; and some discomfort is present in the sinus tarsi. Standard radiographs, of which the lateral view is presented, include anteroposterior, lateral, and oblique views. Because the diagnosis is unclear, more imaging studies are required. The next study to obtain is:
Explanation
 The radiograph demonstrates changes in the subtalar joint suggestive of a middle facet coalition. Note the sclerosis of the joint surface. Although a computed axial tomography scan may be helpful, standard axial views of the subtalar joint (Harris) taken in the plane of the joint are usually diagnostic of tarsal coalition. Motion of the subtalar joint may be normal in the adolescent with a tarsal coalition.
The radiograph demonstrates changes in the subtalar joint suggestive of a middle facet coalition. Note the sclerosis of the joint surface. Although a computed axial tomography scan may be helpful, standard axial views of the subtalar joint (Harris) taken in the plane of the joint are usually diagnostic of tarsal coalition. Motion of the subtalar joint may be normal in the adolescent with a tarsal coalition.
Question 31
The radiograph of a 22-year-old woman with ankle pain and instability is presented. She has noted this problem for 10 years, and it appears to be worsening. The opposite ankle is not symptomatic. She has not had any previous treatment for foot or ankle problems. The cause of this ankle deformity is most likely to be associated with which of the following conditions:
Explanation
Question 32
The sustentaculum tali is the anatomic roof of which tendon:
Explanation
Question 33
The nerve most likely to be at risk during surgical exposure when performing a triple arthrodesis is the:
Explanation
Question 34
A 55-year-old man presents for treatment of pain in the Achilles tendon. This has been present for 2 years, but has suddenly become much worse. The pain is approximately 6 cm proximal to the insertion. He is unable to push off during walking and has pain when ascending stairs. C linical examination reveals thickening of the tendon, weakness of the gastrocnemius-soleus, and pain upon squeezing the Achilles tendon. The magnetic resonance image is shown. The diagnosis is:
Explanation

Question 35
A patient presents for surgical correction of a ruptured Achilles tendon. He recalls injuring his ankle 1 year previously, but did not seek any medical treatment at that time. You plan to repair the tendon, and at surgery, a gap between the tendon ends is noted (Slide). The following procedure is not consistent with an acceptable outcome:
Explanation
 End-to-end repair of a chronic rupture of the Achilles tendon may not be considered if the gap is greater than 2 cm. Equinus positioning is never acceptable. Although each of the other alternatives above may be considered, each has its proponents and potential disadvantages.
End-to-end repair of a chronic rupture of the Achilles tendon may not be considered if the gap is greater than 2 cm. Equinus positioning is never acceptable. Although each of the other alternatives above may be considered, each has its proponents and potential disadvantages.
Question 36
You are commencing a repair of an acute rupture of the Achilles tendon that occurred 8 days previously in a 32-year-old recreational tennis player. Fibrillation of the tendon ends is noted. The following is most important to maximize the ultimate outcome of the repair:
Explanation
Question 37
A 17-year-old patient presents for evaluation and treatment of pain in the back of her ankle. She is a ballet dancer and has noticed that for the past year, she is unable to assume the pointe position without pain. Upon clinical examination she has full range of motion, excellent strength, normal toe function, and pain with pressure in the posterior ankle. The cause of her pain is:
Explanation
 Posterior ankle impingement is common in ballet dancers. When in the pointe position, maximum plantar flexion of the ankle is present, and pain may occur from impingement in the posterior ankle. Flexor hallucis tendonitis may cause posterior ankle pain, but there is no evidence for this condition here.
Posterior ankle impingement is common in ballet dancers. When in the pointe position, maximum plantar flexion of the ankle is present, and pain may occur from impingement in the posterior ankle. Flexor hallucis tendonitis may cause posterior ankle pain, but there is no evidence for this condition here.
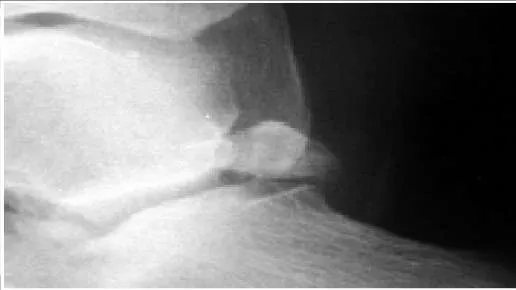
Question 38
The structure that lies immediately medial to the bone prominence in the posterior ankle shown is the:
Explanation
The os trigonum presented in the radiograph may be the cause of posterior ankle impingement. The flexor hallucis longus lies immediately medial to the os and must be protected during excision of this bone.
Question 39
A 43-year-old construction worker sustained a work-related injury to his foot 7 months ago. He was initially treated with cast immobilization and limited weight bearing. He has lateral foot pain and inability to walk comfortably. He has limited walking endurance. Upon examination, pain is present laterally along the course of the peroneal tendons, and no motion of the subtalar joint is present. The recommendation is:
Explanation
 A worker who sustains a calcaneus fracture must be returned to the work force as soon as possible. Although these alternatives for treatment may be considered in the patient with limited activity and low demands, the longer the time from injury to salvage surgery with arthrodesis, the less likely it is that the injured worker will ever return to gainful employment. Therefore, subtalar arthrodesis should be performed.
A worker who sustains a calcaneus fracture must be returned to the work force as soon as possible. Although these alternatives for treatment may be considered in the patient with limited activity and low demands, the longer the time from injury to salvage surgery with arthrodesis, the less likely it is that the injured worker will ever return to gainful employment. Therefore, subtalar arthrodesis should be performed.
Question 40
The structure on the side of the metatarsophalangeal joint of the second toe which is marked by the pointer is the:
Explanation
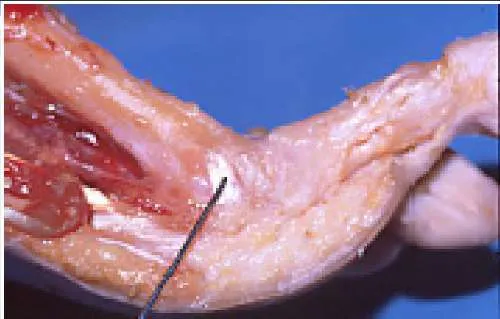 The structure is the volar plate ligament. This ligament may assume a pathologic role in claw toe deformity and instability of the metatarsophalangeal joint.
The structure is the volar plate ligament. This ligament may assume a pathologic role in claw toe deformity and instability of the metatarsophalangeal joint.
Question 41
A 21-year-old man presents for evaluation of high arches, which have been present his entire life. C urrently, he is experiencing some discomfort with running activities. His brother and mother have high arches. He does not recall any trauma as a child, or any other pertinent childhood musculoskeletal problems. C linical examination reveals a rigid deformity bilaterally. The most common cause for his high arches is:
Explanation
Question 42
A 21-year-old man presents for evaluation of high arches, which have been present his entire life. C urrently, he is experiencing some discomfort with running activities. His brother and mother have high arches. He does not recall any trauma as a child, or any other pertinent childhood musculoskeletal problems. C linical examination reveals a rigid deformity bilaterally. What structure is responsible for plantarflexion of the first metatarsal:

Explanation
Question 43
A 22-year-old patient presents for treatment of a painful foot deformity. On examination, a flexible cavovarus deformity is present. The patient has good dorsiflexion foot strength, and eversion strength is weak. A possible tendon transfer that can be used to correct this deformity is:
Explanation
Question 44
A 56-year-old man presents for treatment of chronic ankle pain. He has noted long-standing pain associated with activities since early adulthood. He does not have any other pertinent musculoskeletal history. C linical and radiographic examinations reveal ankle arthritis. A probable cause for this arthritis and deformity is:

Explanation
Question 45
When performing fasciotomy of the foot for acute compartment syndrome, the muscle specifically decompressed through medial fasciotomy is:
Explanation
Question 46
This muscle group demonstrates electrical activity at the time of heel strike:
Explanation
Question 47
A 7-year-old boy presents with bilateral high arches. His parents report that they are having difficulty finding shoes that comfortably fit him. The patient denies any foot pain. The father had similar problems with his feet and was diagnosed with a mild neurologic condition. On exam, the child has bilateral pes cavus with a supple hindfoot. Treatment of the feet at this time should consist of:
Explanation
Question 48
A 50-year-old woman presents with pain in the second toe. She describes this as burning and notes swelling of the toe for the past month. Upon examination, there appears to be instability of the toe with a positive dorsal subluxation stress test. The anatomic structure which is responsible for this patientâ s symptoms is:
Explanation
Question 49
A 15-year-old boy presents with a 2-year history of pain in the foot associated with a sense stiffness and of giving way of the ankle. Upon examination, pain in the sinus tarsi, slightly decreased subtalar motion, and normal ankle motion with no apparent instability are noted. A lateral foot radiograph is presented. The next radiograph to obtain is:
Explanation
 This child presents with symptoms suggestive of a tarsal coalition. There is stiffness, and symptoms of ankle discomfort or instability. On the lateral radiograph, there is consolidation of trabeculation under the posterior facet in the shape of a â C â , a typical finding of a middle facet coalition, which should be investigated further with an axial view of the subtalar joint (Harris).
This child presents with symptoms suggestive of a tarsal coalition. There is stiffness, and symptoms of ankle discomfort or instability. On the lateral radiograph, there is consolidation of trabeculation under the posterior facet in the shape of a â C â , a typical finding of a middle facet coalition, which should be investigated further with an axial view of the subtalar joint (Harris).
Question 50
Which ancillary test is not helpful in the diagnosis of C harcot-Marie-Tooth disease (C MT):
Explanation
Question 51
A 6-year-old child sustains a completely displaced supracondylar humerus fracture. After closed reduction and percutaneous pinning, the fracture heals. However, at 1-year follow-up, the child has a noticeable cubitus varus deformity. What is the most common cause of this specific deformity?
Explanation
Question 52
A 28-year-old man sustains a vertically oriented, displaced femoral neck fracture (Pauwels type III) after a motor vehicle collision. Which of the following fixation constructs provides the greatest biomechanical stability for this specific fracture pattern?
Explanation
Question 53
A 22-year-old female soccer player undergoes anterior cruciate ligament (ACL) reconstruction using a bone-patellar tendon-bone (BTB) autograft. Which of the following is the most frequent complication specific to this graft choice compared to hamstring autografts?
Explanation
Question 54
A 35-year-old carpenter sustains a volar laceration over the proximal phalanx of his index finger, resulting in an inability to flex both the DIP and PIP joints. This injury is classified as occurring in which flexor tendon zone?
Explanation
Question 55
A 45-year-old man presents with sudden severe lower back pain, bilateral sciatica, saddle anesthesia, and urinary retention. MRI reveals a massive L4-L5 central disc herniation. To maximize the chance of full neurological recovery, surgical decompression should ideally be performed within what timeframe?
Explanation
Question 56
A 15-year-old boy presents with progressive knee pain and swelling for 2 months. Radiographs of the distal femur show a mixed lytic and blastic lesion, cortical destruction, and a Codman triangle. After staging, what is the most appropriate next step in management?
Explanation
Question 57
Following a primary total hip arthroplasty via a posterior approach, a patient experiences recurrent posterior dislocations. Radiographs demonstrate an acetabular cup with 5 degrees of retroversion and 45 degrees of inclination. What is the most appropriate surgical intervention?
Explanation
Question 58
A 40-year-old recreational athlete sustains an acute Achilles tendon rupture and opts for non-operative management. What functional protocol has been shown to result in re-rupture rates comparable to surgical repair?
Explanation
Question 59
A diaphyseal tibial fracture is treated with a rigid locked intramedullary nail. Which type of bone healing predominantly occurs in this scenario?
Explanation
Question 60
A 13-year-old obese boy presents with a 3-week history of right groin pain and an obligatory external rotation of the hip when the hip is flexed. What is the most appropriate initial treatment?
Explanation
Question 61
A hemodynamically unstable 30-year-old man is brought in after a motorcycle accident. Pelvic radiograph shows a pubic symphysis diastasis of 4 cm and widening of the sacroiliac joints. After initiating massive transfusion protocols, what is the most appropriate immediate orthopedic intervention?
Explanation
Question 62
A 65-year-old man presents with chronic shoulder pain and pseudoparalysis. MRI reveals a massive, retracted tear of the supraspinatus and infraspinatus tendons with severe fatty infiltration (Goutallier stage 4). What is the most appropriate surgical treatment?
Explanation
Question 63
A 70-year-old woman presents with worsening clumsiness in her hands, difficulty buttoning her shirt, and a broad-based gait. Physical examination reveals a positive Hoffmann's sign bilaterally and lower extremity hyperreflexia. What is the most likely diagnosis?
Explanation
Question 64
A 25-year-old athlete presents with midfoot pain after an axial load to a plantarflexed foot. On an anteroposterior radiograph of the foot, which alignment abnormality is most indicative of a Lisfranc injury?
Explanation
Question 65
A 4-year-old boy presents with refusal to bear weight on his right leg. He has a temperature of 38.8°C (101.8°F), an ESR of 50 mm/hr, and a WBC count of 14,000/mm³. Based on Kocher's criteria, what is the approximate probability that this child has septic arthritis of the hip?
Explanation
Question 66
A 13-year-old obese boy presents with left thigh pain and an obligatory external rotation of the hip during flexion. Radiographs confirm a slipped capital femoral epiphysis (SCFE). Which of the following is the most significant risk factor for the development of chondrolysis in this patient?
Explanation
Question 67
A 35-year-old man sustains a high-energy Schatzker VI tibial plateau fracture.
Twelve hours post-admission, he develops severe pain out of proportion to the injury, exacerbated by passive stretch of his toes. His pedal pulses are palpable. What is the most appropriate next step in management?
Explanation
Question 68
A 55-year-old active man undergoes a total hip arthroplasty. The surgeon opts for a highly cross-linked polyethylene (HXLPE) liner. Which of the following best describes the mechanical trade-off associated with the increased cross-linking of the polyethylene?
Explanation
Question 69
A 68-year-old woman presents with bilateral lower extremity pain that worsens when walking and improves when she leans forward on a shopping cart. She has a history of hypertension and osteoarthritis. Which of the following physical examination findings best differentiates her condition from vascular claudication?
Explanation
Question 70
A 22-year-old male falls on an outstretched hand and presents with anatomic snuffbox tenderness. Radiographs show a displaced fracture of the proximal pole of the scaphoid.
If left untreated, which of the following represents the typical progression of arthritic changes in the wrist?
Explanation
Question 71
A 19-year-old soccer player sustains a twisting injury to her knee. Radiographs reveal an avulsion fracture of the anterolateral proximal tibia (Segond fracture). Which of the following examination findings is most likely to be present?
Explanation
Question 72
A 58-year-old man with a 15-year history of poorly controlled diabetes presents with a red, hot, swollen right foot. There are no open ulcers, and radiographs show fragmentation, periarticular debris, and subluxation of the tarsometatarsal joints. His WBC count is normal. What is the most appropriate initial management?
Explanation
Question 73
A 14-year-old boy presents with progressive knee pain. Radiographs demonstrate a destructive metaphyseal lesion of the distal femur with a sunburst periosteal reaction.
Biopsy confirms high-grade osteosarcoma. Which of the following factors is the most important prognostic indicator for his long-term survival?
Explanation
Question 74
A 42-year-old man is brought to the trauma bay after a motorcycle collision. He is hypotensive with a mechanically unstable pelvis. The trauma team decides to apply a pelvic binder. To be maximally effective in reducing pelvic volume, where should the binder be centered?
Explanation
Question 75
A 66-year-old woman presents with right knee pain 3 years after a total knee arthroplasty. Her ESR is 45 mm/hr and CRP is 22 mg/L. Joint aspiration yields synovial fluid with a WBC count of 4,500 cells/uL with 85% polymorphonuclear leukocytes. Which of the following tests would provide the highest specificity for confirming a periprosthetic joint infection (PJI)?
Explanation
Question 76
A 6-week-old female infant is undergoing treatment for developmental dysplasia of the hip (DDH) with a Pavlik harness. During a follow-up visit, the mother notes that the infant is no longer actively extending her knee on the affected side. What is the most appropriate next step in management?
Explanation
Question 77
A 32-year-old carpenter sustains a small puncture wound to his left index finger. Two days later, he presents with uniform swelling of the digit, flexed resting posture, and excruciating pain with passive extension.
Which of the following is the fourth Kanavel sign typically seen in this condition?
Explanation
Question 78
A 35-year-old man is involved in a high-speed motor vehicle collision. Radiographs and CT of the cervical spine reveal a unilateral facet dislocation at C5-C6. He is neurologically intact. MRI shows a large, extruded disc herniation posterior to the C5 vertebral body. What is the most appropriate next step in management?
Explanation
Question 79
A 12-year-old obese boy presents with a stable slipped capital femoral epiphysis (SCFE) of the left hip. The surgeon plans in situ fixation with a single partially threaded cannulated screw. To avoid the most common complication leading to chondrolysis, which of the following is the most sensitive intraoperative imaging technique to ensure the screw has not penetrated the joint?
Explanation
Question 80
A patient sustains a severe laceration to the proximal forearm, completely transecting the median nerve. However, clinical examination reveals intact intrinsic function of the hand typically supplied by the ulnar nerve, and unexpectedly, intact thenar muscle function. Which of the following anatomical anomalies best explains this physical examination finding?
Explanation
Question 81
A 65-year-old man who underwent a metal-on-metal total hip arthroplasty 8 years ago presents with groin pain and a palpable mass. Serum cobalt and chromium levels are significantly elevated. Aspiration yields sterile, cloudy fluid. Histopathology of the periprosthetic tissue is most likely to show which of the following?
Explanation
Question 82
A 22-year-old soccer player sustains a twisting injury to his knee. Radiographs demonstrate an avulsion fracture of the anterolateral tibial plateau (Segond fracture). Which of the following structures is most likely injured in association with this radiographic finding?
Explanation
Question 83
A 78-year-old woman with a history of severe osteoporosis presents with a displaced intracapsular femoral neck fracture (Garden IV). She is an independent community ambulator but suffers from mild Alzheimer's dementia. Which of the following is the most appropriate surgical treatment?
Explanation
Question 84
A 28-year-old construction worker drops a heavy beam on his midfoot. Radiographs reveal widening of the space between the bases of the first and second metatarsals. What is the anatomical path of the intact Lisfranc ligament?
Explanation
Question 85
A 15-year-old boy presents with progressive pain and swelling in his distal femur. Radiographs reveal a mixed lytic and sclerotic lesion with cortical destruction and a "sunburst" periosteal reaction. Biopsy confirms high-grade osteosarcoma. What is the most important prognostic factor for his overall survival?
Explanation
Question 86
During the process of secondary bone healing, which of the following mechanical and biological environments most strongly promotes the differentiation of mesenchymal stem cells into chondrocytes, leading to endochondral ossification?
Explanation
Question 87
A 65-year-old woman complains of neurogenic claudication and low back pain. Upright lateral radiographs show a grade I degenerative spondylolisthesis at L4-L5. Which of the following anatomical features is most characteristic of degenerative spondylolisthesis compared to isthmic spondylolisthesis?
Explanation
None
