Orthopedic Prometric Exam Preparation MCQs - Part 12
Orthopedic Prometric Exam Preparation MCQs - Part 12
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Lateral epicondylitis is associated with a tear in the fibers of which muscle:
Explanation
Question 2
The gold standard for diagnosis of lateral epicondylitis is considered:
Explanation
Question 3
The amount of time that nonoperative management should be followed for lateral epicondylitis is closest to:
Explanation
Question 4
Extracorporeal shock wave therapy ____ in the treatment of lateral epicondylitis in high-quality trials.
Explanation
Question 5
All of the following medications are indicated in the early treatment of frostbite injury except:
Explanation
Question 6
Orthopedic sequelae of frostbite injury include all of the following except:
Explanation
Question 7
Initial treatment of an acute frostbite injury should include:
Explanation
Question 8
All of the following except _ increase the risk of frostbite injury.
Explanation
Question 9
Treatment for frostbite injury includes:
Explanation
Question 10
Arthritis of the wrist is estimated to effect what percentage of the U.S. population:
Explanation
Question 11
The accessory ulnar collateral ligament inserts on the:
Explanation
Question 12
Which of the following nerves is not a primary articular nerve of the wrist:
Explanation
Question 13
Which of the following nerves provides principal innervation to the central dorsal portion of the wrist:
Explanation
Question 14
What is the area of innervation of the anterior interosseous nerve (AIN):
Explanation
Question 15
When performing complete wrist denervation as described by Wilhem, what pain pathology did not have predictable results:
Explanation
Question 16
What two nerves are resected through a single dorsal incision for wrist denervation:
Explanation
Question 17
What muscle is at risk for denervation when a single dorsal incision is used to denervate the radial side of the wrist:
Explanation
Question 18
A 62-year-old man presents with weakness in finger extension in his right hand. He has had the weakness for 1 month but denies any significant traumatic event. The patient maintains an active lifestyle, including golf and tennis. He denies pain or numbness in his hand and is otherwise neurologically intact. Which of the following is the most likely diagnosis:
Explanation
Question 19
Which of the following are characteristic signs of PIN palsy:
Explanation
Question 20
What is the most common site of posterior interosseous nerve entrapment:
Explanation
Question 21
Which of the following muscles is innervated by the posterior interosseous nerve:
Explanation
Question 22
Posterior interosseous nerve palsy affects finger extension at the metacarpophalangeal and interphalangeal joints.
Explanation
Question 23
A 53-year-old woman presents with bilateral hand numbness and tingling. Her right hand is more affected than her left. The numbness wakes her up at night and is relieved when she shakes her hand. In addition, the patient has had increasing difficulty with fine motor tasks, such as shirt buttoning, over the past 2 to 3 months. Upon close inspection, muscle atrophy is present at the base of her thumbs. Which of the following is the most likely diagnosis:
Explanation
Question 24
All of the following muscles are innervated by the median nerve except:
Explanation
Question 25
All of the following are true regarding the transverse carpal ligament except:
Explanation
Question 26
All of the following structures pass through the carpal tunnel except:
Explanation
Question 27
Dupuytrenâ s contracture characteristically involves which part of the hand:
Explanation
Question 28
The use of clostridial collagenase for Dupuytrenâ s contracture is performed by:
Explanation
Question 29
Dupuytrens cord tissue is characterized by what change from normal:
Explanation
Question 30
A 29-year-old man with a remote history of wrist trauma and chronic pain presents with a palpable clunk on radio-ulnar deviation of the wrist. The most sensitive technique for identifying a scapholunate injury is:
Explanation
Question 31
The radiographic abnormality seen on the lateral radiograph characteristic of scapholunate instability is:
Explanation
Question 32
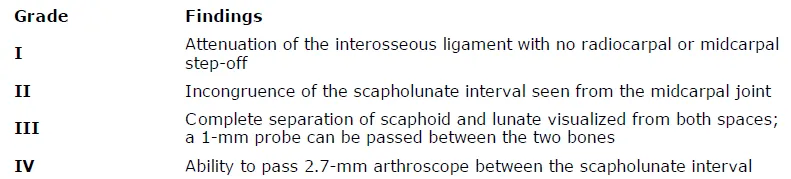
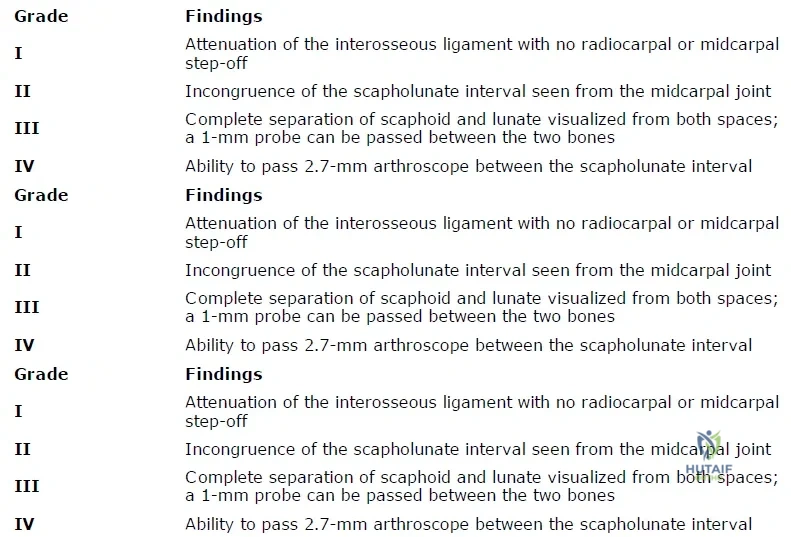
A 40-year-old woman with radial sided wrist pain for the last 2 years presents to the clinic. Plain radiographs are normal. Because of continued discomfort despite conservative therapies and occasional â clickingâ of the wrist, she is taken to the operating room for diagnostic arthroscopy. At the time, fraying of the membranous portion of the scapholunate (SL) ligament is seen, with mild incongruity from the midcarpal joint. The surgeon is unable to pass a 1-mm probe through the defect. This is most consistent with:
Explanation
Question 33
A 33-year-old woman with a history of a traumatic fall onto her wrist and tenderness over the scapholunate (SL) interval presents to the clinic. Radiographs are normal, and magnetic resonance imaging reveals a partial tear of the SL ligament. The remaining wrist ligaments are normal. If conservative therapy is attempted, then it should consist of:
Explanation
Conservative management includes a period of splinting and activity modification, followed by proprioception training of the flexor carpi radialis to act as a dynamic scaphoid stabilizer.
Question 34
Congenital thumb duplication:
Explanation
Question 35
Complete bifurcation of two distal phalanges articulating with a wide epiphysis of a single proximal phalanx is classified as:
Explanation
Question 36
One of the more common complications of congenital thumb duplication reconstruction is:
Explanation
Question 37
Ultrasound therapy delivers superficial heat to the tissue and has a penetration depth of 5 mm.
Explanation
Question 38
Thermal ultrasound is used for all of the following purposes EXC EPT:
Explanation
Question 39
Phonopheresis is:
Explanation
Question 40
Iontophoresis delivers medications such as analgesics or steroids through the skin using an electrical charge.
Explanation
Question 41
Iontophoresis has been effectively used in all of the following EXC EPT:
Explanation
Question 42
Types of nerve tissues surrounding the axons include all of the following EXC EPT:
Explanation
Question 43
The Seddon grades of nerve injury include all of the following EXC EPT:
Explanation
Question 44
Younger age is associated with worse outcomes with nerve repair.
Explanation
Question 45
Optimum conditions for nerve healing after direct repair include:
Explanation
Question 46
Gunshot or missile wounds can frequently cause neuropraxic injuries to peripheral nerves.
Explanation
Question 47
The anatomic location of the pathologic lesion of lateral epicondylitis is the:
Explanation
Question 48
Which of the following injectable substances have shown benefit in the treatment of lateral epicondylitis:
Explanation
Question 49
The nerve most at risk during arthroscopic debridement of lateral epicondylitis is the:
Explanation
Question 50
Common concomitant intra-articular pathology that can be found and addressed at arthroscopy for lateral epicondylitis include all of the following, except:
Explanation
Question 51
A 45-year-old male presents with a terrible triad injury of the elbow after a fall on an outstretched hand.
According to standard surgical protocols, what is the most appropriate sequence of repair to restore elbow stability?
Explanation
Question 52
A 6-year-old child sustains an extension-type supracondylar fracture of the humerus. On examination, the child is unable to form an "A-OK" sign with the thumb and index finger. Which nerve is most likely injured?
Explanation
Question 53
During an open reduction and internal fixation of a complex, intra-articular distal humerus fracture (OTA 13C3), an olecranon osteotomy is planned. At which specific anatomical location should the osteotomy be directed to minimize articular damage?
Explanation
Question 54
Medial epicondylitis is primarily associated with tendinosis and microtearing of the origin of which of the following muscle groups?
Explanation
Question 55
A patient is undergoing in situ decompression for cubital tunnel syndrome. Which of the following structures forms the roof of the cubital tunnel and must be released?
Explanation
Question 56
According to the Bado classification, a Type III Monteggia fracture-dislocation is characterized by a proximal ulna fracture with which associated radial head displacement?
Explanation
Question 57
A 28-year-old male sustains a Galeazzi fracture. Following rigid plate fixation of the radial shaft, the distal radioulnar joint (DRUJ) is noted to be highly unstable in supination but stable in pronation. What is the most appropriate next step in management?
Explanation
Question 58
The primary blood supply to the scaphoid, which accounts for the high rate of avascular necrosis in proximal pole fractures, enters the bone through which surface?
Explanation
Question 59
A 35-year-old manual laborer presents with Lichtman Stage IIIB Kienbock's disease (lunate collapse, fixed scaphoid rotation, no extensive arthritic changes). Radiographs reveal an ulnar minus variance of 3 mm. Which of the following is the most appropriate surgical treatment?
Explanation
Question 60
In the classification of flexor tendon injuries of the hand, Zone II (often referred to historically as "no man's land") extends anatomically from:
Explanation
Question 61
Stenosing tenosynovitis (trigger finger) most commonly results from thickening and nodule formation associated with which of the following pulleys?
Explanation
Question 62
When performing a surgical release for De Quervain's tenosynovitis, the surgeon must ensure complete decompression of the first dorsal compartment. Which two tendons run within this compartment?
Explanation
Question 63
A patient presents with paresthesias in the median nerve distribution of the hand. Which of the following clinical findings most reliably differentiates Pronator Syndrome from Carpal Tunnel Syndrome (CTS)?
Explanation
Question 64
A Holstein-Lewis fracture is a specific fracture pattern of the distal third of the humeral shaft. It carries a particularly high risk of injury to which of the following nerves?
Explanation
Question 65
An intra-articular fracture of the distal radius is identified on radiographs. The volar rim of the radius is fractured and displaced proximally and volarly, carrying the carpus with it. This injury pattern is classically defined as a:
Explanation
Question 66
During a single-incision anterior approach for the repair of an acute distal biceps tendon rupture, which of the following nerves is at the highest risk of iatrogenic injury?
Explanation
Question 67
The Essex-Lopresti injury is a complex upper extremity trauma characterized by a highly specific triad. Which of the following defines this triad?
Explanation
Question 68
In a patient developing acute compartment syndrome of the forearm following a crush injury, which muscles are typically the most severely affected due to their deep central location and specific blood supply?
Explanation
Question 69
A patient is diagnosed with an acute complete rupture of the ulnar collateral ligament (UCL) of the thumb (Skier's thumb). A Stener lesion is suspected, which mandates surgical intervention. A Stener lesion occurs when the torn UCL displaces superficial to the:
Explanation
Question 70
The ulnar collateral ligament (MCL) complex of the elbow provides critical valgus stability. Which specific anatomical bundle of this complex is the primary restraint to valgus stress at 90 degrees of elbow flexion?
Explanation
Question 71
A 4-month-old infant is treated with a Pavlik harness for developmental dysplasia of the hip. At the 2-week follow-up, the infant is noted to have decreased active knee extension on the affected side. What is the most appropriate next step in management?
Explanation
Question 72
A 24-year-old male sustains a proximal pole scaphoid fracture. The high risk of avascular necrosis in this fracture pattern is primarily due to the retrograde blood supply derived from which of the following arteries?
Explanation
Question 73
A 45-year-old male presents with acute onset saddle anesthesia, bilateral lower extremity weakness, and urinary retention following a heavy lifting injury. To maximize the chance of complete neurologic recovery, surgical decompression should ideally be performed within what timeframe from symptom onset?
Explanation
Question 74
A 22-year-old soccer player sustains a twisting injury to the knee. Radiographs reveal a small vertical avulsion fracture of the lateral tibial plateau (Segond fracture). This radiographic finding is virtually pathognomonic for an injury to which primary intra-articular structure?
Explanation
Question 75
A 60-year-old male undergoes a primary total hip arthroplasty using a ceramic-on-ceramic bearing surface. Three years postoperatively, he complains of an audible squeaking sound during ambulation. What is the most likely biomechanical cause of this phenomenon?
Explanation
Question 76
In healthy articular cartilage, which structural component is primarily responsible for providing compressive stiffness and drawing water into the extracellular matrix?
Explanation
Question 77
A 6-year-old boy falls on an outstretched hand and sustains a fracture. Radiographs and clinical presentation are consistent with a posterolaterally displaced extension-type supracondylar humerus fracture.
Which of the following nerve injuries is most commonly associated with this specific direction of displacement?
Explanation
Question 78
In Zone II flexor tendon injuries of the hand, the blood supply to the flexor tendons within the digital synovial sheath is primarily provided by which of the following structures?
Explanation
Question 79
According to the Young-Burgess classification, an Anteroposterior Compression Type II (APC II) pelvic ring injury is characterized by an open-book symphysis disruption along with the rupture of which specific posterior ligaments?
Explanation
Question 80
A 14-year-old boy presents with a destructive metaphyseal lesion of the distal femur with a sunburst periosteal reaction. Biopsy confirms conventional osteosarcoma. Following neoadjuvant chemotherapy, what is the most significant prognostic factor for long-term survival?
Explanation
Question 81
A 28-year-old male sustains a crush injury to his foot. Radiographs reveal a 'fleck sign' in the first intermetatarsal space. This radiographic sign represents an avulsion of the Lisfranc ligament from its attachment on which of the following bones?
Explanation
Question 82
A 26-year-old professional volleyball player presents with insidious onset of posterior shoulder pain and isolated, profound weakness in external rotation. MRI reveals a paralabral cyst. In which anatomical location is the cyst most likely compressing the suprascapular nerve?
Explanation
Question 83
According to Perren's strain theory, absolute stability and primary bone healing require the interfragmentary strain at the fracture gap to be maintained below what critical threshold?
Explanation
Question 84
A 65-year-old male presents with deteriorating handwriting, difficulty buttoning his shirt, and frequent stumbling. Physical examination reveals a positive Hoffmann sign and hyperreflexia in both lower extremities. What is the most sensitive imaging modality for diagnosing the underlying etiology?
Explanation
Question 85
A patient complains of a painful popping and catching sensation at the anterior aspect of the knee when extending from a flexed position, 8 months after a posterior-stabilized total knee arthroplasty. What is the most likely etiology of this condition?
Explanation
Question 86
Which of the following clinical provocative tests has the highest reported sensitivity for diagnosing carpal tunnel syndrome?
Explanation
Question 87
A 32-year-old male sustains a closed tibia fracture and complains of severe pain out of proportion to the injury. Which of the following pressure measurements is considered an absolute indication for emergency four-compartment fasciotomy?
Explanation
Question 88
A 13-year-old obese male presents with a 3-week history of right groin pain and a slight limp. On physical examination, as the right hip is passively flexed, it obligatorily deviates into external rotation. What is the eponymous name of this clinical sign?
Explanation
Question 89
A 35-year-old patient falls on an outstretched hand and presents with severe elbow pain and instability. Radiographs confirm a posterior elbow dislocation, a comminuted radial head fracture, and a Type II coronoid fracture.
If operative intervention is indicated, what is the most widely accepted surgical sequence for addressing this 'terrible triad' injury?
Explanation
Question 90
A 45-year-old carpenter with chronic medial elbow pain that worsens with resisted forearm pronation and wrist flexion has failed 6 months of conservative treatment. During surgical debridement of the common flexor origin, which of the following nerves is most at risk of iatrogenic injury?
Explanation
Question 91
A 40-year-old male weightlifter feels a sudden 'pop' in his anterior elbow during a heavy deadlift. Clinical examination reveals a proximal retraction of the biceps muscle belly and significant weakness in forearm supination. If the surgeon chooses a traditional two-incision surgical approach for the repair, what complication is classically most associated with this specific technique?
Explanation
Question 92
A patient with long-standing cubital tunnel syndrome presents with weakness in their pinch grip. During evaluation, the patient forcefully flexes the interphalangeal joint of the thumb when attempting to hold a piece of paper between the thumb and index finger. What is the name of this clinical sign?
Explanation
Question 93
A 50-year-old presents with a fluctuant olecranon mass, erythema, and fever. Initial aspiration yields fluid with a WBC count of 65,000/mm3. After 48 hours of appropriate intravenous antibiotics and serial aspiration, the erythema continues to expand and the drainage becomes frankly purulent. What is the most appropriate next step in management?
Explanation
Question 94
A 6-year-old child sustains a severely displaced extension-type supracondylar humerus fracture. On presentation, the hand is pink but the radial pulse is absent. Following urgent closed reduction and percutaneous pinning, the hand remains pink with brisk capillary refill, but the radial pulse is still not palpable. What is the most appropriate next step?
Explanation
Question 95
A 7-year-old boy sustains a Bado Type I Monteggia fracture-dislocation. Closed reduction of the ulnar shaft fracture is successfully achieved, but the radial head remains anteriorly dislocated despite appropriate maneuvers. What is the most common anatomic structure blocking the reduction of the radial head in this scenario?
Explanation
Question 96
A 40-year-old female presents with severe elbow pain after a fall. Radiographs demonstrate an isolated, large fracture of the capitellum involving the articular surface with significant posterior displacement (Type I Hahn-Steinthal fracture). Which surgical approach provides the most optimal visualization for open reduction and internal fixation of this fracture?
Explanation
Question 97
An adult patient undergoes rigid plate fixation of the radial shaft for a Galeazzi fracture. Intraoperatively, following radius fixation, the distal radioulnar joint (DRUJ) is tested and found to be grossly unstable in all forearm positions (pronation, neutral, and supination). What is the most appropriate next step in management?
Explanation
Question 98
A 5-year-old child presents to the emergency department after an elbow injury. The orthopedic resident reviews the elbow radiographs to assess for any avulsion fractures. According to the normal sequential ossification of the pediatric elbow (CRITOE), at what age does the medial epicondyle ossification center typically appear?
Explanation
None
