Orthopedic Prometric Exam Preparation MCQs - Part 3

Orthopedic Prometric Exam Preparation MCQs - Part 3
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 67-year-old woman sustained a cerebrovascular accident 18 months previously, and has problems with ambulation. She notes that the ankle buckles with ground contact. Upon examination, she ambulates with slight circumduction of one limb, and heel varus is present during the swing and heel strike phases of gait. The procedure that would stabilize her foot during ground contact is:
Explanation
Question 2
A 19-year-old man presents for treatment in the emergency department following a motorcycle accident. He sustained an isolated injury to his foot and ankle. The recommended treatment is:
Explanation
 necessary. Following open reduction and internal fixation, arthritis of the talonavicular joint may occur.
necessary. Following open reduction and internal fixation, arthritis of the talonavicular joint may occur.
Question 3
A 23-year-old man sustains an injury to his foot when falling off a ladder. The foot is grossly twisted inward, and the talonavicular joint is dislocated with the talar head penetrating through the extensor brevis muscle. The dislocation is reduced. The likelihood of this resulting in avascular necrosis of the talus is:
Explanation
Question 4
A 53-year-old diabetic patient presents with an ulcer on the plantar aspect of the foot that has been present for 2 years. There is mild serous drainage; bone is not exposed. The recommended treatment is:
Explanation

Question 5
Which of the following is not a feature of the foot deformity in C harcot- Marie-Tooth disease (C MT):
Explanation
Question 6
A 32-year-old woman was treated surgically for ankle instability 2 years ago. She notes that her ankle is stable, but over the past year, she has noted progressive difficulty with the use of her big toe. She finds that her toe no longer touches the ground. This is confirmed upon pedobarograph testing, because there is no contact between the first metatarsal and the ground, which is an abnormal finding compared to her opposite foot. The appearance of the foot is presented. The probable cause for this is:
Explanation
 the first metatarsal. The peroneus longus is no longer functioning, and first metatarsus elevatus is present.
the first metatarsal. The peroneus longus is no longer functioning, and first metatarsus elevatus is present.
Question 7
A 26-year-old woman presents for treatment of painful forefoot deformity. Hallux valgus is present, with a 35° angle, and arthritis of the metatarsophalangeal (MP) joint. The second and third lesser toe MP joints are dislocated with juxta-articular erosions of the fourth metatarsal head noted. The ideal surgical treatment is:
Explanation
Question 8
A 20-year-old collegiate football player sustains an injury to his big toe during a scrimmage game. He was pushing off when another player fell on his foot, resulting in the hallux being hyperextended. Two days later he has pain and swelling in the joint, limited motion, and normal radiographs. The recommended treatment is:
Explanation
Question 9
A 43-year-old patient presents with pain in the hallux metatarsophalangeal (MP) joint. Motion is limited in dorsiflexion and to some extent in plantarflexion, and mild arthritis is radiographically evident. If a cheilectomy is performed on this patient, what is the primary goal of the procedure in the management of hallux rigidus:
Explanation
Question 10
The most common complication after resection of a plantar fibromatosis is:
Explanation
Question 11
A 24-year-old man presents for treatment of a painful fifth toe deformity. He had the deformity for 10 years and notes that it is getting progressively worse. On examination, a claw toe deformity is present. There is 90° of fixed hyperextension of the metatarsophalangeal joint, 70° of flexion at the interphalangeal joint, and a painful corn on the distal tip of the phalanx. The patient would like surgical correction. Which procedure is most likely to give him relief of pain and correction of deformity:
Explanation
Question 12
A 22-year-old collegiate basketball player presents for treatment of a stress fracture of the base of the fifth metatarsal at the junction of the metaphysis and diaphysis. The fracture was treated operatively, and the patient returned to playing basketball. Three months later, it was apparent that a repeat fracture was present. The fracture was treated with screw removal and a repeat screw fixation. Four months later, after a successful basketball season, he sustained a repeat stress fracture of the metatarsal. On examination, he has a mild cavovarus foot configuration with normal ankle range of motion. Inversion is 15° and eversion is 5°. The base of the fifth metatarsal is prominent. The most likely cause for the repeat fracture is:
Explanation
Question 13
Which statement regarding the peroneal tendon(s) is incorrect:
Explanation
Question 14
A 41-year-old patient presents for treatment of a joint depression calcaneus fracture. A Sanders type IIA fracture is visible on a computerized tomography scan. After appropriate counseling, the patient elects nonoperative treatment. What is the most common complication of this injury that may subsequently occur in this patient:
Explanation
Question 15
A patient presents for treatment of a painful ankle 2 years after a hindfoot injury. He was treated nonsurgically for a calcaneus fracture that occurred when he fell. His symptoms include anterior ankle pain, weakness during pushing off, and pain along the lateral aspect of the hindfoot. On examination, he has pain to palpation at the tip of the fibula, absent inversion and eversion, 20° of plantarflexion, and no dorsiflexion. Plantarflexion strength appears adequate, and there is no compromise of the forefoot flexor function. The recommended surgical procedure is:
Explanation
Question 16
A patient presents for treatment of painful toes 1 year after open reduction and internal fixation of a calcaneus fracture. He notes difficulty with shoe wear and pain on ambulation. On examination, there are fixed claw toe deformities of the second, third, and fourth toes that are painful. The most likely cause of the toe deformities is:
Explanation
Question 17
A 56-year-old patient sustained an ankle fracture 3 years ago that was treated with closed reduction and cast immobilization. Since the injury, she has experienced pain upon ambulation and ankle stiffness. On examination, the range of motion of the ankle is 5° of dorsiflexion and 30° of plantarflexion. C repitus with motion is not present, but the patient does experience severe pain. A radiograph is presented (Slide). The recommended procedure to alleviate the patientâ s pain and improve function is:

Explanation
Question 18
A 43-year-old construction worker presents for treatment of ankle pain. The patient recounts a fall from a height that caused an ankle fracture 2 years ago. The fracture was treated with closed reduction and cast immobilization for 5 months. He experiences pain upon ambulation and is unable to work. On examination, the range of ankle motion is 5° dorsiflexion and 20° plantarflexion. There is no crepitus with motion, but severe pain is present. A radiograph is presented (Slide 1). The recommended procedure to alleviate pain and improve function is:
Explanation

Question 19
A 29-year-old patient has had pain in her foot for 1 year. She twisted her ankle and was treated for a sprain with a brace and therapy. She has persistent pain in her foot and pain on ambulation. On examination, slight pes planus is present, pain is noted on manipulation of the foot, and there is tenderness in the midfoot and hindfoot. A radiograph is presented (Slide). The most likely cause of the pain is:
Explanation
 Slight abduction of the tarsometatarsal joints is noted, along with arthritis of the medial and middle columns of the midfoot. This likely resulted from a tear of the ligament between the base of the second metatarsal and the medial cuneiform (Lisfranc ligament).
Slight abduction of the tarsometatarsal joints is noted, along with arthritis of the medial and middle columns of the midfoot. This likely resulted from a tear of the ligament between the base of the second metatarsal and the medial cuneiform (Lisfranc ligament).
Question 20
A 53-year-old man presents with a swollen foot. He does not recall any injury to the foot, and he has minimal pain. He does not have any pertinent medical history. The clinical and radiographic appearance of the foot is presented (Slide 1 and Slide 2). Based upon the information, the recommended treatment of this injury is:
Explanation
Question 21
A 49-year-old woman has had swelling in the posterior aspect of the ankle for 5 years (Slide). The pain is focal and does not radiate. She notes that pain is worse with activity, exercise, and shoe wear. Which of the following is not an acceptable treatment for this patient:

Explanation
Question 22
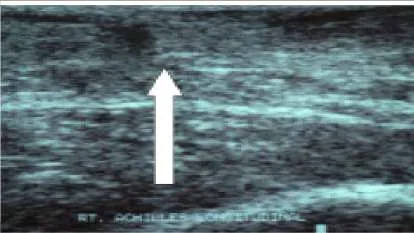
This slide (the arrow is pointing in the direction of the pathology) illustrates which of the following conditions of the Achilles tendon:
Explanation
Question 23
Which of the statements regarding paratendinitis of the Achilles tendon is true:
Explanation
Question 24
A 65-year-old woman presents for treatment of a painful flatfoot condition. On examination, the hindfoot is in marked valgus and a rupture of the posterior tibial tendon is noted. The recommended treatment is a transfer of the flexor digitorum longus tendon and a medial translational osteotomy of the calcaneus. The rationale for the osteotomy includes all of the following except:
Explanation
Question 25
Which of the following muscles has the largest cross-sectional diameter:
Explanation
Question 26
After surgery to the hallux, a patient complains of burning and numbness along the medial aspect of the first metatarsal. The numbness extends from the medial cuneiform distally to the midportion of the first metatarsal and junction of the plantar and dorsal skin. The nerve involved with the pain is the:
Explanation
Question 27
The most common complication after resection arthroplasty (Keller) of the base of the hallucal proximal phalanx for correction of hallux valgus is:
Explanation
Question 28
A patient sustains a fracture of the anterior process of the calcaneus. What ligament is responsible for avulsion of this bone:
Explanation
Question 29
The ball and socket ankle deformity shown (Slide) is associated with all of the following except:
Explanation
Question 30
A patient wants a below the knee amputation. As an alternative, you recommend a Syme amputation. What is the most relevant factor that would contraindicate performing a Syme amputation:
Explanation
Question 31
Which of the following statements regarding a fracture of the junction of the proximal metaphyseal and diaphyseal portion of the fifth metatarsal is false:
Explanation
Question 32
A foot is maximally dorsiflexed during this point of the gait cycle:
Explanation
Question 33
Which of the following structures is disrupted in patients with an acute medial subtalar dislocation:
Explanation
Question 34
An 8-year-old soccer player has had bilateral heel pain for 3 months. He has no constitutional complaints. Isolated tenderness to the posterior aspect of his calcaneal tuberosity is present. Recommended treatment is:
Explanation
Question 35
A 26-year-old recreational volleyball player presents with complaints of recurrent right ankle instability. She has undergone 3 months of peroneal strengthening and proprioceptive training without success. She has tried and failed ankle bracing. She has a positive anterior drawer finding on examination, and her hindfoot is in neutral alignment. The recommended surgical plan is:
Explanation
Question 36
A 65-year-old woman presents with pain along the posteromedial aspect of her right ankle. She has a clinical deformity of her foot with loss of normal arch height. Her hindfoot is in valgus but is passively correctable to neutral. She has weakness with inversion and cannot perform a single stance heel raise. She has not had any form of treatment. Recommended treatment includes:
Explanation
Question 37
After counseling a 22-year-old patient who is scheduled to undergo a triple arthrodesis, he wants to know the risk that he will develop ankle arthritis. You tell him:
Explanation
Question 38
A 57-year-old woman presents for treatment of a painful flatfoot deformity. She says that her foot has been painful for 4 years, but she does not recall any injury to the foot. The opposite foot is not bothersome. Upon examination, she has pain in the midfoot and hindfoot. Resisted inversion is strong and painful. She is able to perform a single and repetitive heel rise test. The most likely diagnosis is:
Explanation
Question 39
Which clinical examination is likely to confirm a suspected rupture of the posterior tibial tendon:
Explanation
Question 40
The most reliable indication of an interdigital neuroma in the second web space is:
Explanation
Question 41
A 68-year-old patient presents for evaluation of ankle pain. He is unable to walk more than 10 minutes without pain and stiffness. He has been treated with anti-inflammatory medication, intra-articular injection of steroid, and an ankle foot orthosis. He has 35° of clinical motion associated with crepitus and pain and there is no motion in the subtalar joint. Radiographs demonstrate large osteophytes in the anterior ankle, no joint space, and mild osteophytes of the talonavicular joint. The recommended surgical treatment is:
Explanation
Question 42
A 21-year-old recreational athlete presents for treatment of ankle weakness. She notes that she trips frequently, that the ankle feels unstable, particularly on uneven ground surfaces, and that she has experienced frequent sprains. On examination, the ankle appears to be unstable and radiographs demonstrate no instability on stress testing. The most likely diagnosis is:
Explanation
Question 43
The symptoms of a tarsal tunnel syndrome may become aggravated by:
Explanation
Question 44
A 56-year-old woman presents for evaluation and treatment of a painful hallux. She notes the pain over the dorsal surface of the hallux metatarsophalangeal (MP) joint and on the plantar aspect of the hallux interphalangeal (IP) joint. C linically, there is no range of motion in dorsiflexion of the hallux MP joint, pain upon attempted movement of the MP joint, and 20° of extension of the hallux IP joint. Radiographs demonstrate arthritis of the hallux MP joint and normal alignment of the first metatarsal. The surgical procedure that is likely to cause further mechanical problems for this patient is:
Explanation
Question 45
A 38-year-old woman presents for evaluation of painful hallux rigidus. Her clinical and radiographic images are shown (Slide 1 and Slide 2). Based upon her presentation, what is the likelihood that first metatarsus elevatus is responsible for her clinical condition:
Explanation
Surgeons cannot assume that an elevated first metatarsal is responsible for causing hallux rigidus. On a lateral radiograph, there may be notable elevation of the first metatarsal (as present in this patient), but the elevation may be a secondary result of the limited motion of the hallux metatarsophalangeal joint. Studies have demonstrated that there is no difference in the elevation of the first metatatarsal in patients with hallux rigidus.
Question 46
The patient shown in Slide 1 and Slide 2 underwent surgical correction of painful hallux rigidus. The purpose of the procedure on the hallux was:
Explanation
Question 47
Of the proximal first metatarsal osteotomies listed below, which has the least stability for dorsiflexion load:
Explanation
Question 48
A 54-year-old patient presents for correction of painful hallux valgus. She has a prominent medial eminence, pain on pressure over the metatarsophalangeal (MP) joint, increased elevation of the first metatarsal, and painful callosity under the second metatarsal. The recommended procedure is:
Explanation
Question 49
This patient was treated for metatarsalgia with an oblique osteotomy of the metatarsal head and neck (Weil osteotomy). Although the symptoms of metatarsalgia dissipated, she has continued complaints about the position of the toe (Slide 1 and Slide
Explanation
 Following an oblique osteotomy of the metatarsal head and neck (Weil osteotomy), the interosseous tendons shift dorsal to the axis of the metatarsal head. Instead of functioning as strong plantarflexors of the MP joint, they may now function as dorsiflexors, leading to the elevation of the toe off the ground and dorsal contracture.
Following an oblique osteotomy of the metatarsal head and neck (Weil osteotomy), the interosseous tendons shift dorsal to the axis of the metatarsal head. Instead of functioning as strong plantarflexors of the MP joint, they may now function as dorsiflexors, leading to the elevation of the toe off the ground and dorsal contracture.
Question 50
The strongest plantarflexor of the metatarsophalangeal (MP) joint of the lesser toes is the:
Explanation
Question 51
A 35-year-old male sustains an axial load injury to a plantarflexed foot. Radiographs reveal widening of the space between the first and second metatarsals. A "fleck sign" is also noted. The primary ligament injured in this condition originates from and inserts into which of the following structures?

Explanation
Question 52
A 45-year-old female presents after a high-speed motor vehicle collision with a Schatzker IV tibial plateau fracture. Which of the following neurovascular structures is at the highest risk of injury in this specific fracture pattern?
Explanation
Question 53
A 65-year-old male complains of worsening clumsiness in his hands and difficulty buttoning his shirts over the last 6 months. Examination reveals a positive Hoffman's sign bilaterally and hyperreflexia in the lower extremities. What is the most appropriate next step in management?
Explanation
Question 54
A 13-year-old obese male presents with a 3-week history of groin pain and a limp. On examination, there is obligatory external rotation of the hip during passive hip flexion. The pathology of this condition occurs primarily through which zone of the physis?
Explanation
Question 55
A 70-year-old female presents with recurrent posterior dislocations following a primary total hip arthroplasty. Radiographic evaluation shows the acetabular component is placed in 10 degrees of anteversion and 30 degrees of inclination. What is the most appropriate surgical intervention?
Explanation
Question 56
A 22-year-old female soccer player sustains a non-contact pivoting injury to her knee, hearing a loud "pop." Radiographs show an elliptic bone fragment avulsed from the lateral tibial plateau (Segond fracture). This fracture represents an avulsion of which structure?
Explanation
Question 57
A 24-year-old male falls on an outstretched hand and presents with anatomic snuffbox tenderness. Initial standard radiographs of the wrist are negative for fracture. What is the most appropriate next step in management to definitively rule out a fracture?
Explanation
Question 58
A 30-year-old male sustains a completely displaced femoral neck fracture (Pauwels type III) following a fall from a height. He is neurovascularly intact. What is the most appropriate definitive treatment?
Explanation
Question 59
A 40-year-old construction worker undergoes ORIF of a displaced intra-articular calcaneus fracture via an extensile lateral approach. The most common wound complication associated with this approach is necrosis of the flap apex. Which artery primarily supplies this flap?
Explanation
Question 60
A 6-month-old female is referred for asymmetric thigh folds and limited hip abduction. Which imaging modality is most appropriate to evaluate for developmental dysplasia of the hip (DDH) at this age?
Explanation
Question 61
A 15-year-old male presents with worsening distal femur pain. Radiographs reveal a mixed lytic/sclerotic lesion with a "sunburst" periosteal reaction. Staging studies are performed. What is the most common site of metastasis for this primary bone tumor?
Explanation
Question 62
A 68-year-old male is 5 years post-primary total knee arthroplasty and presents with a swollen, painful knee. Aspirate reveals 65,000 WBC/hpf with 95% polymorphonuclear cells. What is the most widely accepted surgical treatment for this chronic periprosthetic joint infection?
Explanation
Question 63
A 28-year-old male sustains an open midshaft tibia fracture. There is a 12 cm laceration with severe periosteal stripping, and the wound cannot be closed primarily, requiring a rotational muscle flap for coverage. What is the correct Gustilo-Anderson classification?
Explanation
Question 64
A 72-year-old female presents with bilateral leg pain and heaviness that worsens with walking and improves when leaning over a shopping cart. At which spinal level does the pathology causing this condition most frequently occur?
Explanation
Question 65
A closed tibia fracture is treated with a long leg cast. The fracture heals primarily through callus formation. This type of bone healing relies fundamentally on which cellular process?
Explanation
Question 66
A 25-year-old male presents with recurrent anterior shoulder instability. Advanced imaging reveals 25% anterior glenoid bone loss and a large, engaging Hill-Sachs lesion. Which surgical procedure is most appropriate to prevent recurrence?
Explanation
Question 67
A 42-year-old man presents in hemorrhagic shock following a severe crush injury to his pelvis. Pelvic radiograph shows a 4 cm pubic symphysis diastasis with disruption of the sacroiliac joints. Following 1L of crystalloid fluid, his blood pressure remains 75/40 mmHg. The most appropriate immediate next step in management is:
Explanation
Question 68
A 12-year-old boy presents with left hip pain and an obligate external rotation of the hip with flexion. Radiographs confirm a mild left slipped capital femoral epiphysis (SCFE). Which of the following is the strongest indication for prophylactic pinning of the contralateral asymptomatic hip?
Explanation
Question 69
A 55-year-old man with poorly controlled diabetes presents with a swollen, warm, and erythematous right foot. Radiographs reveal prominent bone fragmentation, subluxation at the tarsometatarsal joints, and joint debris.
According to the Eichenholtz classification, what is the current stage and most appropriate management?
Explanation
Question 70
A 62-year-old woman undergoes an uncomplicated total hip arthroplasty using a ceramic-on-ceramic bearing surface. Two years postoperatively, she complains of an audible 'squeaking' sound from her hip during walking. What surgical factor is most strongly associated with this phenomenon?
Explanation
Question 71
A 68-year-old man presents with deteriorating handwriting and frequent falls. Examination reveals hyperreflexia in both lower extremities and a positive Hoffmann's sign. He exhibits the 'finger escape sign' when asked to hold his fingers extended and adducted. This sign is most commonly associated with compression of which of the following spinal cord tracts?
Explanation
Question 72
A 28-year-old carpenter sustains a laceration over the volar aspect of the proximal phalanx of his index finger. Examination reveals the inability to actively flex the proximal and distal interphalangeal joints. This injury occurred in which flexor tendon zone, and what is the optimal timing for primary repair?
Explanation
Question 73
A 22-year-old female soccer player undergoes anterior cruciate ligament (ACL) reconstruction using a bone-patellar tendon-bone (BPTB) autograft. Compared to the native ACL, what is the ultimate tensile load of a 10 mm wide BPTB graft?
Explanation
Question 74
A 15-year-old boy is diagnosed with a conventional high-grade intramedullary osteosarcoma of the distal femur. He undergoes neoadjuvant chemotherapy followed by wide surgical resection. Which of the following is the most important prognostic factor for his overall survival?
Explanation
Question 75
A 31-year-old man falls from a height and sustains a displaced fracture of the talar neck with subluxation of the subtalar joint, but the tibiotalar joint remains congruous.
According to the Hawkins classification, what is the expected rate of avascular necrosis (AVN) of the talar body for this injury?

Explanation
Question 76
A 45-year-old man undergoes open reduction and internal fixation of a transverse radial shaft fracture using a dynamic compression plate providing absolute stability. Which of the following histologic processes predominantly characterizes the bone healing in this scenario?
Explanation
Question 77
A 2-week-old infant is being treated for idiopathic congenital talipes equinovarus using the Ponseti method. After sequential correction of the cavus, adductus, and varus deformities over several weeks, the foot remains in significant equinus. What is the next appropriate step in management?
Explanation
Question 78
A 24-year-old man falls onto an outstretched hand and complains of anatomic snuffbox tenderness. MRI confirms a nondisplaced fracture of the proximal pole of the scaphoid. What is the primary arterial supply to the proximal pole of the scaphoid that places it at high risk for nonunion and avascular necrosis?
Explanation
Question 79
A 70-year-old woman who underwent a primary total knee arthroplasty 4 years ago presents with a sudden inability to actively extend her knee after a fall. Radiographs reveal a normal-appearing prosthesis but superior displacement of the patella. What is the most appropriate surgical management for this acute injury?
Explanation
Question 80
A 35-year-old male presents to the emergency department after a high-speed motor vehicle collision. Radiographs demonstrate a butterfly fragment of the pubic rami and widening of the sacroiliac joint. During the secondary survey, blood is noted at the urethral meatus. What is the most appropriate next step in management?
Explanation
Question 81
A 16-year-old female soccer player sustains a non-contact pivoting injury to her knee. MRI confirms an isolated rupture of the anterior cruciate ligament (ACL). Which of the following anatomic factors is most strongly associated with an increased risk for this specific injury pattern?
Explanation
Question 82
A 65-year-old woman undergoes a primary total hip arthroplasty via a posterior approach. Six weeks postoperatively, she presents to the emergency department with a posterior dislocation that occurred while rising from a low toilet seat. Which of the following component positions is most likely responsible for this instability?
Explanation
Question 83
A 13-year-old obese male presents with a 4-week history of right groin pain and a worsening limp. Physical examination reveals an obligate external rotation of the hip during passive flexion. Radiographs demonstrate posterior and inferior displacement of the proximal femoral epiphysis. What is the standard of care for this condition?
Explanation
Question 84
A 22-year-old man falls on an outstretched hand and complains of severe radial-sided wrist pain. Examination reveals marked tenderness within the anatomic snuffbox.
Initial PA and lateral radiographs are interpreted as negative. What is the most appropriate initial management?
Explanation
Question 85
A 15-year-old boy presents with severe knee pain that awakens him at night. Plain radiographs reveal a mixed lytic and sclerotic lesion in the distal femoral metaphysis with a prominent 'sunburst' periosteal reaction. Core biopsy confirms high-grade intramedullary osteosarcoma. What is the standard sequence of treatment?
Explanation
Question 86
A 70-year-old man complains of dropping objects and difficulty buttoning his shirts, along with a stiff, broad-based gait. Physical examination demonstrates a positive Hoffmann sign bilaterally, hyperreflexia in the lower extremities, and an inverted supinator reflex. What is the most likely diagnosis?
Explanation
Question 87
A 28-year-old man sustains a closed tibial shaft fracture during a football tackle. Twelve hours post-injury, he develops excruciating leg pain that is out of proportion to the injury and unrelieved by intravenous opioids. His pain is exacerbated by passive stretch of the hallux. Pulses are palpable. What is the definitive treatment?
Explanation
Question 88
A 55-year-old man with a 15-year history of poorly controlled type 2 diabetes presents with a swollen, warm, and erythematous right foot. He denies fever, chills, or any open wounds. Plain radiographs show midfoot osteopenia and early subluxation of the tarsometatarsal joints. Inflammatory markers are only mildly elevated. What is the most appropriate initial management?
Explanation
Question 89
A basic science researcher is studying the mechanics of fracture healing.
Under conditions of absolute stability, such as rigid compression plating where the fracture site experiences less than 2% interfragmentary strain, which biological process predominantly dictates bone healing?
Explanation
None
