Orthopedic Prometric Exam Preparation MCQs - Part 13

Orthopedic Prometric Exam Preparation MCQs - Part 13
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Arthroscopic resection/debridement posterior to the midline of the radio- capitellar joint can result in damage to __ ligament, resulting in ______ instability.
Explanation
Question 2
The muscle that flexes the interphalangeal joint of the thumb is innervated by which roots of the brachial plexus:
Explanation
Question 3
The anterior interosseous nerve (AIN) originates from the median nerve at what distance from the medial epicondyle:
Explanation
Question 4
man presents to the emergency department with a 6-week history of difficulty writing and pain after playing tennis. She also reports a recent inability to abduct and adduct her fingers. What is the mechanism of her symptoms:
Explanation
Question 5
What is the innervation of the indicated muscle in the image (Slide):
Explanation
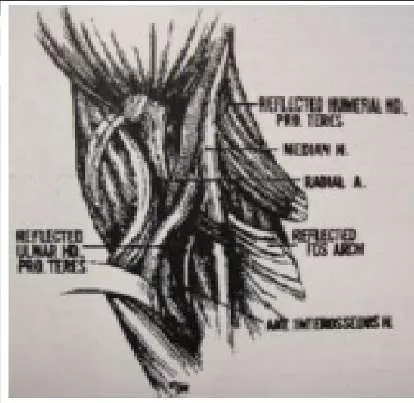 The arrow in the photograph (Slide) is pointing to the pronator teres â one of the most common sites for compression of the anterior interosseous nerve. The pronator teres is innervated by the median nerve.
The arrow in the photograph (Slide) is pointing to the pronator teres â one of the most common sites for compression of the anterior interosseous nerve. The pronator teres is innervated by the median nerve.
Question 6
Sites of potential compression of the median nerve include all of the following except:
Explanation
Question 7
What position of the wrist most commonly produces scaphoid fractures:
Explanation
Question 8
Which of the following blood vessels supplies the majority of the scaphoid:
Explanation
Question 9
During a posterior (dorsal) approach to percutaneous screw fixation for a scaphoid fracture, many structures are close to the guidewire insertion location and are at risk for injury. Which of the following structures is the closest to the guidewire insertion location according to a recent cadaveric study:
Explanation
Question 10
Which of the following is a concerning risk factor for a dorsal open approach to the scaphoid:
Explanation
Question 11
A volar approach to the scaphoid is ideal in which of the following fractures:
Explanation
Question 12
Which finger is most commonly involved in a flexor digitorum profundus (FDP) avulsion injury:
Explanation
Question 13
Which type of flexor digitorum profundus (FDP) avulsion is considered the most severe:
Explanation
Question 14
When performing pollicization to correct a hypoplastic thumb, the surgeon should rotate the index finger:
Explanation
Question 15
For which types of thumb hypoplasia is pollicization the best option:
Explanation
Question 16
What is the most critical step in pollicization to create a normal-looking thumb:
Explanation
Question 17
All of the following may be present in a child with type IIIA hypoplasia except:
Explanation
Question 18
The main 3-4 viewing portal for wrist arthroscopy lies in between which two tendons:
Explanation
Question 19
C omplications after wrist arthroscopy occur in what percentage of patients:
Explanation
Question 20
C omplications after wrist arthroscopy occur in what percentage of patients:
Explanation
Question 21
The fracture fragment in Bennettâ s fracture is located in which of the following areas of the hand:
Explanation
Question 22
Which of the following two main soft tissue forces are disrupted by Bennets fracture subluxation:
Explanation
Question 23
The greatest amount of step-off that is well-tolerated in a Bennettâ s fracture is:
Explanation
Question 24
When fracture step-off is greater than the accepted limits, which of the following complications is the most common:
Explanation
Question 25
C linically, what is the upper limit of acceptable fracture angulation for a fifth metacarpal neck fracture:
Explanation
Question 26
In cadaveric models, when does the biomechanics of fifth finger flexion consistently change in relationship to metacarpal neck fracture angulation:
Explanation
Question 27
Up to how much angulation can be tolerated in the small finger metacarpal shaft fracture:
Explanation
Question 28
If a metacarpal shaft fracture shortens 4 mm, what will the theoretical amount of extensor lag be at the metacarpophalangeal joint:
Explanation
Question 29
In a short oblique metacarpal shaft fracture without comminution or bone loss, what is usual amount of maximal shortening that will occur:
Explanation
Question 30
Which of the following statements is true regarding metacarpophalangeal joint anatomy:
Explanation
Question 31
Which of the following fracture patterns and mechanisms is incorrectly paired:
Explanation
Question 32
Giant cell tumor of tendon sheath commonly occurs in which of the following age groups:
Explanation
Question 33
Which of the following clinical features is common in giant cell tumor of tendon sheath:
Explanation
Question 34
After plain radiographs of giant cell tumor of tendon sheath are obtained, the following imaging study should be obtained:
Explanation
Question 35
Which of the following cell types is not typically found in giant cell tumors of tendon sheath:
Explanation
Question 36
A 25-year-old, right-hand-dominant male truck driver presents to the emergency department (Slide 1, Slide 2). The tip of his left ring finger was amputated in a bicycle accident 2 weeks prior. The amputated piece was â sewn back onâ in the emergency department immediately after the accident, but â turned blackâ over the next week. There is no evidence of infection. He states that the appearance of his finger is embarrassing, and he would like it taken care of as soon as possible. Which of the following procedures is the most appropriate:
Explanation
Question 37
A 52-year-old, right-hand-dominant watchmaker arrives at the emergency department 30 minutes after the volar soft tissue of his right thumb and index finger was avulsed while using a bandsaw. Physical examination shows 2 cm 3 2 cm wounds involving the distal phalanx of each affected digit. No exposed tendon or bone is present, and no involvement of the joints is noted. The patient requests a treatment option that will retain the most sensation so he can effectively continue in his occupation. Which of the following options is the most appropriate management of this patientâ s wounds:
Explanation
Question 38
Which of the following is not considered a part of the triangular fibrocartilage complex:
Explanation
Question 39
Which of the following arterial branches does not supply the peripheral 25% of the triangular fibrocartilage complex:
Explanation
Question 40
Which of the following statements is true:
Explanation
Question 41
Which of the following parameters is not a determinant of the Palmer classification of triangular fibrocartilaginous complex injuries:
Explanation
Question 42
What are the components of a Galeazzi fracture-dislocation:
Explanation
Question 43
Who are the most common athletes to get medial epicondylitis of the elbow:
Explanation
Question 44
Indications for replantation include:
Explanation
Question 45
An amputation through the wrist is an indication for attempted replantation.
Explanation
Question 46
Care of an amputated part prior to replantation includes:
Explanation
Question 47
Replants are monitored by:
Explanation
Question 48
C omplications post-replantation include:
Explanation
Question 49
Placing some tension on a flexor tendon repair increases the ultimate tensile strength of the repair.
Explanation
Question 50
Flexor tendon nutrition is derived from:
Explanation
Question 51
A 35-year-old carpenter presents with an inability to make an "OK" sign with his thumb and index finger. A diagnosis of Anterior Interosseous Nerve (AIN) syndrome is suspected. Which of the following muscles will have NORMAL function in this patient?
Explanation
Question 52
During an in situ ulnar nerve decompression at the elbow, the surgeon releases the tissue spanning the two heads of the flexor carpi ulnaris (FCU). Which anatomical structure forms the primary roof of the cubital tunnel in this region?
Explanation
Question 53
The radial nerve is at risk during a lateral approach to the distal humerus. At approximately what distance proximal to the lateral epicondyle does the radial nerve pierce the lateral intermuscular septum to transition from the posterior to the anterior compartment?
Explanation
Question 54
A 24-year-old athlete undergoes posterior cruciate ligament (PCL) reconstruction. The surgeon must understand the biomechanics of the PCL's two primary bundles. Which bundle is most taut in knee flexion?
Explanation
Question 55
A patient with refractory lateral epicondylitis undergoes open surgical debridement. The primary pathological tissue targeted during this procedure is the origin of which of the following structures?
Explanation
Question 56
A 45-year-old typist complains of aching pain in the proximal forearm and numbness in the radial three and a half digits. Which physical examination finding most reliably distinguishes pronator syndrome from carpal tunnel syndrome?
Explanation
Question 57
The 'terrible triad' of the elbow is notoriously difficult to manage due to profound instability. This injury pattern typically involves a posterior elbow dislocation, a radial head fracture, and a fracture of which of the following structures?
Explanation
Question 58
A 42-year-old male undergoes a single-incision anterior approach for the repair of an acute distal biceps tendon rupture. Postoperatively, he complains of numbness along the lateral aspect of his forearm. Which nerve was most likely injured?
Explanation
Question 59
During shoulder arthroscopy for instability, the surgeon identifies a Buford complex. This normal anatomical variant is defined by a thickened, cord-like middle glenohumeral ligament and the absence of which structure?
Explanation
Question 60
A 6-year-old child sustains a displaced extension-type supracondylar humerus fracture.
Based on typical displacement patterns, what is the most common neurological deficit associated with this specific injury?
Explanation
Question 61
A 50-year-old male sustains a displaced femoral neck fracture. Which artery is the primary contributor to the blood supply of the adult femoral head, placing it at high risk for avascular necrosis in this injury?
Explanation
Question 62
In an anterior cruciate ligament (ACL) reconstruction, positioning the femoral tunnel is critical for restoring rotational stability. For a right knee, placing the tunnel at which clock face position optimally mimics the native anatomical footprint?
Explanation
Question 63
A 13-year-old obese boy presents with an insidious onset of knee pain and a limp. A pelvic radiograph is obtained.
Which of the following radiographic lines is most appropriate to evaluate for Slipped Capital Femoral Epiphysis (SCFE)?
Explanation
Question 64
A 4-month-old infant is being treated with a Pavlik harness for Developmental Dysplasia of the Hip (DDH). The mother notes that the child has stopped kicking the affected leg. On exam, the child lacks active knee extension. Which nerve is most likely compressed due to hyperflexion?
Explanation
Question 65
During a posterior approach to the shoulder, the axillary nerve is visualized emerging through the quadrangular space. Which muscle forms the inferior border of this anatomical space?
Explanation
Question 66
Flexor tendon injuries in 'Zone 2' of the hand are historically referred to as 'no man's land' due to the high risk of adhesion formation. What are the anatomical boundaries of Zone 2?
Explanation
Question 67
A 22-year-old male sustains a scaphoid waist fracture. Which of the following best describes the predominant arterial supply to the scaphoid, explaining its propensity for proximal pole avascular necrosis?
Explanation
Question 68
A 28-year-old manual laborer presents with dorsal wrist pain. Radiographs reveal sclerosis and fragmentation of the lunate (Kienbock's disease). Which of the following radiographic anatomical variants is most highly associated with this condition?
Explanation
Question 69
A patient undergoes a radiograph 8 weeks after an undisplaced talar neck fracture. A subchondral radiolucent band is seen in the talar dome (Hawkins sign). What does this finding signify?
Explanation
Question 70
During hip arthroscopy, establishing the anteroinferior portal carries the highest risk of injury to which of the following neurological structures?
Explanation
Question 71
A 25-year-old male sustains a high-energy trauma resulting in the hip injury shown.
During the surgical approach for fixation, understanding the vascular anatomy is critical to prevent avascular necrosis. The deep branch of the medial femoral circumflex artery (MFCA) consistently runs between which two structures?
Explanation
Question 72
An 8-year-old child presents with an extension-type supracondylar humerus fracture as shown.
If the distal fragment demonstrates significant posteromedial displacement, which nerve is at the greatest risk of injury due to tethering across the fracture site?
Explanation
Question 73
Highly cross-linked ultra-high-molecular-weight polyethylene (UHMWPE) is widely used in total hip arthroplasty to reduce volumetric wear. Which step in its manufacturing process significantly reduces the risk of in vivo oxidation but comes at the cost of decreasing the ultimate tensile strength?
Explanation
Question 74
A 19-year-old male presents with severe, aching pain in his mid-tibia that classically worsens at night. He reports complete relief of symptoms within 30 minutes of taking aspirin. Radiographs reveal a cortical lucency surrounded by sclerosis. The central nidus of this lesion predominantly secretes high levels of which biochemical mediator?
Explanation
Question 75
A 24-year-old athlete undergoes a posterolateral corner (PLC) reconstruction of the knee utilizing a fibular-based technique. The surgeon isolates a nerve that winds posterior to the biceps femoris tendon. A motor deficit resulting from injury to this specific nerve would manifest primarily as weakness in which muscle?
Explanation
Question 76
A 35-year-old male falls from a ladder and sustains an L2 burst fracture. Imaging shows 40% canal compromise. He is neurologically intact, and MRI confirms an intact posterior ligamentous complex. According to the Thoracolumbar Injury Classification and Severity Score (TLICS), what is his total score and the generally recommended management?
Explanation
Question 77
A hypotensive trauma patient is diagnosed with an Anteroposterior Compression Type III (APC-III) pelvic ring disruption. A pelvic binder is applied, and the patient undergoes immediate pre-peritoneal pelvic packing. This intervention primarily aims to tamponade bleeding from which of the following anatomic structures?
Explanation
Question 78
A 45-year-old male presents with recurrent posterolateral rotatory instability (PLRI) of the elbow. During surgical reconstruction of the lateral ulnar collateral ligament (LUCL), the isometric point on the lateral epicondyle must be identified for graft placement. Where is this point anatomically located?
Explanation
Question 79
A patient presents with an inability to make an "OK" sign with their thumb and index finger following a forearm injury. Which of the following muscles is primarily innervated by the affected nerve?
Explanation
Question 80
A 32-year-old female fell on an outstretched hand and sustained the injury shown in the radiograph.
Assuming this is a "terrible triad" injury of the elbow, which of the following is the standard evidence-based surgical sequence for management?
Explanation
Question 81
During an electrodiagnostic evaluation for suspected cubital tunnel syndrome, a Martin-Gruber anastomosis is identified. This anatomical variant involves a neural connection between which two structures?
Explanation
Question 82
An obese 13-year-old boy presents with left knee pain and an obligate external rotation of the hip during flexion. The radiograph is shown below.
When treating this condition with in situ percutaneous pinning, what is the most significant iatrogenic risk factor for the development of chondrolysis?
Explanation
Question 83
A 28-year-old pitcher complains of right upper extremity heaviness, fatigue, and numbness in the ulnar digits after throwing. Examination reveals a positive Adson's test and reproduction of symptoms with hyperabduction. If neurogenic thoracic outlet syndrome is confirmed, the neurovascular bundle is most commonly compressed between which structures?
Explanation
Question 84
A 22-year-old soccer player sustains a twisting knee injury. Radiographs reveal a small avulsion fracture of the lateral tibial plateau (Segond fracture). This pathognomonic finding is an avulsion of the capsule and the anterolateral ligament (ALL). It is most highly associated with a tear of which other structure?
Explanation
Question 85
A 6-month-old infant with developmental dysplasia of the hip (DDH) failed Pavlik harness treatment and is scheduled for a closed reduction and spica casting. During the procedure, the surgeon assesses the "safe zone" of Ramsey. How is this zone defined?
Explanation
Question 86
A 45-year-old male sustains a C5-C6 bilateral interfacetal dislocation from a motor vehicle accident. He is awake, alert, cooperative, and has a complete C5 spinal cord injury (ASIA A). What is the most appropriate initial step in management before surgical stabilization?
Explanation
Question 87
During secondary fracture healing, the cartilaginous soft callus is eventually replaced by hard woven bone. Which of the following transcription factors is most essential for the initial differentiation of multipotent mesenchymal stem cells into the osteoblastic lineage?
Explanation
None
