Orthopedic Pediatrics 2026 MCQs: Board Review Questions & Answers (Part 4)
Key Takeaway
Your ultimate guide to Orthopedic Pediatrics 2026 MCQs: Board Review Questions & Answers (Part 4) starts here. Top-rated Orthopedic Pediatrics 2026 MCQs bank. Practice with clinical case questions, orthopedic surgery board review, and evidence-based answers updated for 2026.
Orthopedic Pediatrics 2026 MCQs: Board Review Questions & Answers (Part 4)
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
The mother of a 24-month-old girl reports that the child cannot rotate her right forearm. She also notes delayed development, with the child first walking at 18 months. The child has a five-word vocabulary and has not begun using simple phrases. Examination reveals that the right forearm is fixed in 80 degrees of pronation. The remainder of the examination of both upper extremities is otherwise normal. A radiograph is shown in Figure 41. Which of the following studies will best aid in diagnosis?
Explanation
Question 2
Figure 42 shows the radiograph of a patient with spinal muscular atrophy. Examination reveals good upper extremity function, and she can tie her shoes and propel a manual wheelchair. Posterior instrumentation and fusion may result in
Explanation
Question 3
A 2-week-old infant has had diminished movement of the right upper extremity since birth. Examination reveals weakness of shoulder abduction and external rotation, elbow flexion, and forearm supination. Both pupils are equally round and responsive to light. The remainder of the examination is normal. Radiographs of the upper limb show a healing middle-third clavicle fracture. Management should consist of
Explanation
Question 4
Progressive paralysis is most likely to be seen in association with what type of congenital vertebral abnormality?
Explanation
Question 5
A 9-year-old child has right groin pain after falling from a tree. Examination reveals that the right leg is held in external rotation, and there is significant pain with attempts at passive range of motion. Radiographs are shown in Figures 43a and 43b. Management should consist of
Explanation
Question 6
An 8-year-old boy with moderate factor VIII hemophilia played kickball earlier in the day and now reports progressively severe groin pain and is unable to walk. Examination reveals marked paresthesias over the medial aspect of the distal tibia. What is the most likely diagnosis?
Explanation
Question 7
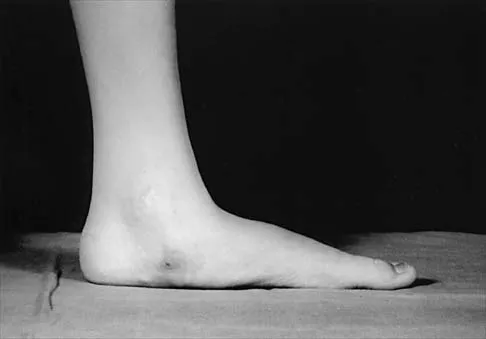
The patient shown in Figure 44 reports that her toes hurt when she walks. Management should consist of
Explanation
Question 8
Figures 45a and 45b show the AP and lateral radiographs of a 15-year old patient who is undergoing surgery to add 3 cm of length to the femur. Based on the radiographic findings, what is the next most appropriate step in management?
Explanation
Question 9
Examination of a 9-year-old boy reveals a right thoracic prominence on forward flexion. Neurologic examination is normal, and no other abnormalities are noted. AP radiographs reveal a 30-degree right thoracic curve. Initial management should consist of
Explanation
Question 10
A 13-year-old boy is comatose and has irregular breathing after being struck by a car while riding his bicycle. Auscultation suggests a pneumothorax on the right side and swelling about the right arm and leg. Initial management should consist of
Explanation
Question 11
Overgrowth of a limb in a patient with neurofibromatosis type 1 (NF1) is most likely associated with the presence of
Explanation
Question 12
A 14-year-old girl with a right thoracic curve from T4 through L2 measuring 78 degrees is scheduled to undergo posterior spinal fusion for scoliosis. The surgical plan is to fuse from T3 through L2, using pedicle screws at L2 and about the apex at T8. What neural monitoring modality is most likely to identify a reversible neurologic deficit during surgery?
Explanation
Question 13
Figure 46 shows the radiograph of an obese 12-year-old boy who has had left hip pain for the past 3 months. What is the best course of action?
Explanation
Question 14
A 7-year-old boy sustained a head contusion and small bowel injuries in a motor vehicle accident in which he was wearing a lap belt. He subsequently required a bowel resection. Six weeks after the accident, his parents note a painful mass in his lower back. His neurologic examination is normal. A radiograph and CT scans are shown in Figures 47a through 47c. Definitive management should now consist of
Explanation
Question 15
A 5-month-old girl with arthrogryposis has a limb-length discrepancy. Examination and radiographs reveal unilateral hip dislocation. Management should consist of
Explanation
Question 16
A 10-year-old boy who has had progressive low back and right buttock pain for the past 3 days is now unable to bear weight on the right side secondary to pain. He has a temperature of 101.3 degrees F (38.5 degrees C). Examination reveals full hip range of motion; but he reports pain on the right side with external rotation. Pain is elicited with compression of the iliac wings and with direct palpation of the right sacroiliac (SI) joint. An MRI scan of the pelvis shows no abscess, but there is inflammation of the SI joint. Management should consist of
Explanation
Question 17
Figures 48a and 48b show the elbow radiographs of a 5-year-old boy who fell from a tree after dinner. Examination reveals that he is unable to extend his wrist. Management should consist of immediate
Explanation
Question 18
In addition to the radiographic features seen in Figures 49a and 49b, this patient will most likely have which of the following findings?
Explanation
Question 19
A biopsy of the involved physis in a patient with slipped capital femoral epiphysis (SCFE) would most likely reveal
Explanation
Question 20
A 12-year-old girl has a 4-cm limb-length discrepancy following a fracture of the left distal femur 2 years ago. Examination reveals 18 degrees of genu valgum on the involved side, with 7 degrees of genu valgum on the opposite side. Radiographs show that the left distal femoral growth plate is now closed; however, the tibial growth plate is still open. Her bone age matches her chronologic age. Management should consist of
Explanation
Question 21
The parents of a previously healthy 3-year-old child report that she refused to walk on awakening. Examination later in the day reveals that the patient can walk but with a noticeable limp. She has a temperature of 99.5 degrees F (37.5 degrees C). Range of motion measurements are shown in Figure 50. An AP pelvis radiograph is normal. Laboratory studies show a WBC count of 9,000/mm3 and an erythrocyte sedimentation rate of 10 mm/h. Management should consist of
Explanation
Question 22
A 12-year-old boy with hemophilia A and no known inhibitors sustains a tibia fracture and has pain with passive motion of the deep toe flexors. Appropriate management should consist of
Explanation
Question 23
A 10-year-old boy with spastic diplegic cerebral palsy walks in a crouched position with the hips and knees flexed. Maximum knee flexion is 15 degrees during early swing phase. Instrumented gait analysis shows quadriceps activity from terminal stance throughout swing phase. Treatment should consist of
Explanation
Question 24
A 4-year-old boy with arthrogryposis has little active motion of his knees or elbows. Both elbows are in full extension with good triceps strength, but he is unable to bring his hand to his face or feed himself. Management should consist of
Explanation
Question 25
A 14-year-old competitive gymnast has had activity-related low back pain for the past month. Examination reveals no pain with forward flexion, but she has some discomfort when resuming an upright position. She also has pain with extension and lateral bending of the spine. The neurologic examination is normal. Popliteal angles measure 20 degrees. AP, lateral, and oblique views of the lumbar spine are negative. What is the next most appropriate step in management?
Explanation
Question 26
A 6-year-old boy falls on an outstretched hand and sustains a supracondylar humerus fracture. A radiograph reveals a completely displaced extension-type (Gartland Type III) fracture.
On physical examination in the emergency department, an anterior interosseous nerve (AIN) palsy is diagnosed. Which of the following clinical findings is most likely present to confirm this diagnosis?

Explanation
Question 27
A 6-year-old girl with spastic quadriplegic cerebral palsy (GMFCS level V) is evaluated for hip pain and difficulty with perineal hygiene. An anteroposterior pelvis radiograph reveals a migration percentage of 45% on the right hip and 40% on the left hip, with moderate acetabular dysplasia.
What is the most appropriate surgical management for this patient?

Explanation
Question 28
A 6-week-old female infant is undergoing treatment with a Pavlik harness for developmental dysplasia of the left hip. During the 2-week follow-up visit, the mother notes that the child has stopped kicking her left leg. On physical examination, the infant exhibits an absent patellar reflex on the left side and decreased active knee extension. Sensibility appears intact. What is the most appropriate next step in management?
Explanation
Question 29
A 4-year-old boy presents with a relapsed left idiopathic clubfoot. The deformity was initially treated successfully in infancy with the Ponseti method. The parents report he is now walking on the outside of his foot. Gait analysis demonstrates dynamic supination of the foot during the swing phase. Physical examination reveals an easily correctable deformity with completely passive plantigrade positioning. What is the most appropriate surgical treatment?
Explanation
Question 30
An 8-year-old boy presents with a 3-month history of a painless limp and right hip stiffness. Radiographs demonstrate fragmentation of the capital femoral epiphysis. Measurements reveal that exactly 40% of the lateral pillar height is maintained.
According to the Herring Lateral Pillar Classification, what group does this patient fall into, and what is the typical outcome associated with surgical containment for his age and classification?

Explanation
Question 31
A 14-year-old boy complains of vague midfoot pain and recurrent ankle sprains for the past 6 months. Physical examination reveals bilateral flatfeet with significantly decreased subtalar motion and peroneal spasticity. A lateral radiograph of the right foot demonstrates the 'anteater nose' sign. Which of the following statements regarding his condition is correct?
Explanation
Question 32
A 6-year-old girl with Osteogenesis Imperfecta (Sillence Type III) is referred to the orthopedic clinic after sustaining her fourth diaphyseal femur fracture in two years. She is currently undergoing cyclic intravenous bisphosphonate therapy.
Which of the following surgical interventions is the gold standard for managing recurrent diaphyseal femur fractures in this patient population?

Explanation
Question 33
A 13-year-old female competitive gymnast presents with progressive low back pain and bilateral radicular symptoms radiating to the posterior thighs. Examination reveals a palpable 'step-off' at the lumbosacral junction, a crouched gait, and severe hamstring tightness. Standing lateral radiographs reveal a Meyerding Grade III isthmic spondylolisthesis at L5-S1 with a slip angle of 45 degrees. What is the most appropriate definitive management?
Explanation
Question 34
A newborn male is evaluated in the nursery for a significant right upper extremity deformity. The forearm is shortened and bowed volarly, and the hand is in fixed radial deviation. Radiographs confirm an absent radius and an absent thumb. Before addressing the orthopedic deformity, which of the following systemic evaluations is most critical?
Explanation
Question 35
A 2-year-old boy presents with a 3-day history of right knee swelling, a mild limp, and a low-grade fever (37.9°C). Initial laboratory work reveals a WBC count of 11,000/mm3, an ESR of 30 mm/hr, and a CRP of 2.5 mg/dL. Synovial fluid aspiration yields 65,000 WBCs/mm3 with 80% neutrophils. Gram stain is negative, and routine aerobic solid cultures show no growth at 48 hours. Which of the following pathogens is the most likely culprit, and what specific diagnostic technique is required to identify it?
Explanation
Question 36
A 13-year-old obese male presents with an inability to bear weight on the right leg after a minor fall. He reports having had a mild, aching knee pain for 2 months prior to the fall. Radiographs reveal a severe posterior and inferior displacement of the proximal femoral epiphysis. If an open reduction and internal fixation via a surgical dislocation approach (modified Dunn procedure) is planned, preservation of which of the following vessels is most critical to prevent osteonecrosis of the femoral head?
Explanation
Question 37
A 3-year-old girl is evaluated for bilateral bowing of the lower extremities. Her BMI is above the 95th percentile. Standing radiographs demonstrate a metaphyseal-diaphyseal angle (Drennan's angle) of 18 degrees bilaterally, with prominent medial beaking of the proximal tibia. What is the most appropriate initial management?
Explanation
Question 38
A 6-week-old female is being treated with a Pavlik harness for a dislocated left hip. At the 2-week follow-up, an ultrasound confirms the hip remains dislocated. The examiner also notes that the infant has decreased spontaneous extension of the left knee, though she vigorously kicks the right leg. What is the most likely cause of this new clinical finding?
Explanation
Question 39
A 6-year-old boy falls from the monkey bars and sustains a completely displaced, extension-type supracondylar humerus fracture. On arrival, his hand is pink but the radial pulse is absent. Capillary refill is brisk (< 2 seconds). Following closed reduction and percutaneous pinning, the hand remains pink with brisk capillary refill, but the radial pulse remains unpalpable. What is the next best step in management?
Explanation
Question 40
An 8-year-old boy presents with a limp and right hip pain of several months' duration. Radiographs demonstrate sclerosis and early fragmentation of the proximal femoral epiphysis.
Which of the following is considered the most significant prognostic factor for the development of early osteoarthritis in patients with this condition?
Explanation
Question 41
A 7-year-old with spastic quadriplegic cerebral palsy (GMFCS Level V) presents for routine hip surveillance. An AP pelvis radiograph demonstrates a migration percentage (Reimer's index) of 45% on the right and 15% on the left. Clinically, the right hip can be abducted to 20 degrees. What is the most appropriate management for the right hip?
Explanation
Question 42
A 3-month-old infant is undergoing serial casting for idiopathic congenital talipes equinovarus using the Ponseti method. During the casting process, the physician attempts to correct the equinus deformity by dorsiflexing the foot before the heel varus and forefoot adductus are fully corrected. This technical error is most likely to result in which of the following iatrogenic deformities?
Explanation
Question 43
A 4-year-old girl is evaluated for recurrent fractures following minimal trauma. Clinical examination reveals blue sclerae and evidence of dentinogenesis imperfecta. Genetic testing confirms a mutation in COL1A1. Which of the following mechanisms best describes the action of the medical therapy most commonly used to decrease fracture burden in this patient?
Explanation
Question 44
A newborn is evaluated for a shortened right lower extremity. Physical examination reveals an anteromedial bowing of the tibia, a dimple over the anterior mid-tibia, and an absent lateral ray (3-ray foot).
Which of the following is the most common associated skeletal anomaly found in the ipsilateral limb of patients with this specific condition?

Explanation
Question 45
A 14-year-old male presents with rigid, painful flatfeet and a history of recurrent ankle sprains. Examination shows significantly restricted subtalar motion and peroneal spasticity. A CT scan confirms a middle facet talocalcaneal coalition involving 60% of the posterior facet area, accompanied by early degenerative changes in the talonavicular joint. What is the most appropriate definitive surgical intervention?
Explanation
Question 46
A 9-year-old boy presents with left knee pain and an obligatory external rotation of the left lower extremity with hip flexion. Radiographs demonstrate a severe, chronic slipped capital femoral epiphysis (SCFE) on the left. The patient's medical history is significant for chronic kidney disease and secondary hyperparathyroidism. Following in situ pinning of the left hip, what is the most appropriate management for the asymptomatic right hip?
Explanation
Question 47
A 6-week-old female infant is undergoing treatment with a Pavlik harness for a dislocated right hip (developmental dysplasia of the hip). During a follow-up visit after 1 week, the parents report that the infant is no longer extending her right knee spontaneously. On examination, the knee extension is absent, and the patellar reflex is diminished. This complication is most likely the result of which of the following positioning errors in the harness?
Explanation
Question 48
An 18-month-old girl presents with bilateral genu varum. Standing full-length lower extremity radiographs reveal a metaphyseal-diaphyseal angle (Drennan's angle) of 18 degrees bilaterally, along with beaking of the medial proximal tibial metaphysis. What is the most appropriate initial management?
Explanation
Question 49
A 7-year-old boy with spastic quadriplegic cerebral palsy (GMFCS Level IV) is evaluated during a routine hip surveillance clinic. Anteroposterior pelvis radiographs demonstrate a migration percentage of 55% in the right hip, with breaking of Shenton's line. The hip is reducible on physical examination. What is the most appropriate surgical intervention?
Explanation
Question 50
An orthopaedic surgeon is treating a 2-week-old infant with idiopathic congenital clubfoot using the Ponseti method. When applying the first cast to correct the cavus deformity, which specific manipulative maneuver is required?
Explanation
Question 51
A 6-year-old boy sustains a Gartland type III extension-type supracondylar humerus fracture. On initial evaluation in the emergency department, the hand is pink and warm with brisk capillary refill, but the radial pulse is not palpable. After emergent closed reduction and percutaneous pinning in the operating room, the fracture is anatomically aligned, but the radial pulse remains absent. The hand remains warm and pink. What is the most appropriate next step in management?
Explanation
Question 52
An 8-year-old boy is diagnosed with Legg-Calvé-Perthes disease of the right hip. Which of the following radiographic findings is considered the most significant poor prognostic indicator, predictive of a poor long-term outcome (Stulberg class IV or V)?
Explanation
Question 53
A healthy 3-year-old boy weighing 15 kg sustains an isolated, closed, spiral fracture of the middle third of the right femur after falling off a trampoline. There is 2 cm of shortening and no neurovascular deficits. What is the standard of care for definitive management?
Explanation
Question 54
A 14-year-old boy presents with chronic, vague hindfoot pain and a history of recurrent ankle sprains. Physical examination reveals bilateral rigid, flat feet with markedly decreased subtalar motion and peroneal spasticity. A 45-degree internal oblique radiograph of the foot demonstrates an elongated anterior process of the calcaneus bridging to the navicular, often referred to as the 'anteater nose' sign. What is the most likely diagnosis?
Explanation
Question 55
A 5-year-old girl with Osteogenesis Imperfecta (Type III) has a history of recurrent long bone fractures and progressive bowing deformities. She is receiving cyclical intravenous pamidronate therapy. This pharmacological agent decreases the incidence of fractures primarily through which of the following cellular mechanisms?
Explanation
Question 56
A 12-year-old obese boy presents with a 4-week history of left groin pain and a new inability to bear weight on the left leg for the past 48 hours. On examination, his left lower extremity is externally rotated, and attempts at hip flexion result in obligate external rotation. Radiographs demonstrate a left slipped capital femoral epiphysis (SCFE). He undergoes in situ percutaneous pinning. Which of the following factors presents the highest risk for the development of avascular necrosis (AVN) of the femoral head in this patient?
Explanation
Question 57
A 6-year-old boy falls from the monkey bars and sustains a widely displaced, extension-type supracondylar humerus fracture.
On presentation in the emergency department, his hand is pink and warm, but the radial pulse is not palpable. He is taken emergently to the operating room. After successful closed reduction and percutaneous pinning, the hand remains pink with brisk capillary refill, but the radial pulse is still absent on Doppler ultrasound. What is the most appropriate next step in management?
Explanation
Question 58
A 4-year-old boy with a history of idiopathic clubfoot, initially treated successfully with the Ponseti method, presents to the clinic with his parents who report he is 'walking on the outside of his foot'. Gait analysis reveals a dynamic supination deformity during the swing phase. Physical examination shows his ankle passively dorsiflexes to 15 degrees beyond neutral with the knee extended. What is the most appropriate surgical management for this relapse?
Explanation
Question 59
A 13-year-old girl complains of frequent right ankle sprains and midfoot pain that worsens with activity. On examination, she has a rigid pes planovalgus foot and significantly limited subtalar motion. Radiographs reveal an elongated anterior process of the calcaneus (the 'anteater nose' sign).
Initial nonoperative management with a short leg cast fails to alleviate her symptoms. What is the most appropriate surgical intervention?

Explanation
Question 60
A 7-year-old child with spastic quadriplegic cerebral palsy is evaluated for progressive bilateral hip subluxation. His Gross Motor Function Classification System (GMFCS) level is V. Anteroposterior pelvis radiographs show a Reimers migration percentage of 55% bilaterally. There are no degenerative changes of the femoral head or acetabulum. What is the most appropriate treatment to achieve durable hip stability?
Explanation
Question 61
A 6-month-old girl with a dislocated left hip is brought to the operating room for a closed reduction and spica casting. An intraoperative arthrogram is performed to assess the adequacy of reduction.
On the arthrogram, the surgeon identifies a radiolucent block traversing the inferior aspect of the acetabulum, preventing concentric seating of the femoral head. Which of the following anatomical structures is most likely causing this specific block to reduction?
Explanation
Question 62
A 2.5-year-old girl is evaluated for severe bilateral bowing of her legs. She is at the 95th percentile for weight. Standing radiographs show a metaphyseal-diaphyseal angle of 18 degrees bilaterally, with prominent medial metaphyseal beaking of the proximal tibias. What is the most appropriate initial management?
Explanation
Question 63
A 9-year-old boy presents with a 6-month history of a painless snapping sensation in his lateral right knee. He recently began experiencing pain and an inability to fully extend the knee. MRI reveals a discoid lateral meniscus. During arthroscopy, the meniscus is found to lack the normal posterior coronary ligament attachments and is hypermobile. Which specific variant of discoid meniscus does this presentation describe?
Explanation
Question 64
A 4-year-old child with a known history of recurrent fractures and blue sclerae is being treated with intravenous bisphosphonate therapy (pamidronate).
Radiographs of the long bones demonstrate multiple dense horizontal bands ('zebra lines') in the metaphyses. What is the primary mechanism by which this medication produces these radiographic findings?

Explanation
Question 65
An 8-year-old boy is diagnosed with Legg-Calvé-Perthes disease of the right hip. Anteroposterior and frog-leg lateral radiographs taken during the fragmentation stage demonstrate a >50% depression of the lateral pillar height of the capital femoral epiphysis. According to the Herring lateral pillar classification, what is his classification and the expected clinical prognosis?
Explanation
Question 66
A 7-year-old child with spastic quadriplegic cerebral palsy (GMFCS level IV) presents with progressive bilateral hip displacement. Recent radiographs show a migration percentage of 55% bilaterally with increased femoral anteversion and coxa valga, but no significant degenerative joint changes. She has painful hips and difficulty with perineal care. What is the most appropriate surgical management?
Explanation
Question 67
A 30-month-old girl is evaluated for bilateral severe bowing of her legs. She has a BMI in the 95th percentile and achieved independent ambulation at 10 months of age. Radiographs reveal a varus deformity centered at the proximal tibia with metaphyseal beaking. Langenskiöld stage II changes are present.
What is the most appropriate initial management?
Explanation
Question 68
A 5-year-old boy sustains a widely displaced, extension-type supracondylar humerus fracture. On presentation, his hand is pink and warm, but the radial pulse is absent.
The patient undergoes emergent closed reduction and percutaneous pinning. Postoperatively, the hand remains well-perfused with brisk capillary refill (under 2 seconds) and normal oxygen saturation, but the radial pulse remains absent. What is the most appropriate next step in management?
Explanation
Question 69
A 13-year-old boy with a BMI of 38 presents to the emergency department unable to bear weight on his left leg after stumbling on a step. Radiographs confirm a severe, displaced slipped capital femoral epiphysis (SCFE). He is unable to walk even with crutches. Which of the following complications is most specifically associated with this patient's acute presentation compared to a patient who is able to bear weight?
Explanation
Question 70
A 3-year-old girl is evaluated for a painless limp and leg length discrepancy. Examination reveals a positive Galeazzi sign and asymmetric thigh folds. Anteroposterior pelvis radiograph shows a dislocated right hip with significant acetabular dysplasia, a false acetabulum, and increased femoral anteversion. What is the most appropriate definitive surgical intervention?
Explanation
Question 71
A 4-year-old boy who was successfully treated for an idiopathic right clubfoot as an infant using the Ponseti method now presents with a relapsed deformity. His parents note recurrent intoeing and that he walks on the lateral border of the foot. Physical examination shows dynamic supination of the foot during the swing phase of gait and fixed equinus of 10 degrees. What is the most appropriate treatment strategy?
Explanation
Question 72
A 3-year-old boy presents with a noticeable spinal curvature. Standing full-spine radiographs demonstrate a unilateral unsegmented bar spanning from T8 to T10, with a contralateral fully segmented hemivertebra at T9.
What is the expected natural history of this specific spinal anomaly if left untreated?

Explanation
Question 73
A 6-year-old boy with Osteogenesis Imperfecta (OI) type III presents with progressive anterolateral bowing of bilateral femurs, causing pain and difficulty with ambulation. He has a history of multiple low-energy fractures. What is the preferred surgical intervention to address the severe long bone deformities and minimize the risk of recurrent fractures?
Explanation
Question 74
A 9-year-old boy is diagnosed with Legg-Calvé-Perthes disease (LCPD) of the right hip. Radiographs in the fragmentation stage demonstrate collapse of more than 50% of the lateral pillar of the femoral head (Herring Lateral Pillar Class C). Which of the following factors in this patient is most strongly associated with a poor radiographic and functional outcome at skeletal maturity?
Explanation
Question 75
A 13-year-old boy with Duchenne Muscular Dystrophy (DMD) presents for evaluation. He lost the ability to ambulate 18 months ago and is wheelchair-dependent. Examination reveals poor sitting balance and a progressive spinal deformity. Radiographs demonstrate a neuromuscular scoliosis of 45 degrees extending from T4 to the pelvis. His current forced vital capacity (FVC) is 40% of predicted. What is the most appropriate management for his spinal deformity?
Explanation
Question 76
A 6-year-old boy is brought to the emergency department after falling from monkey bars. Radiographs demonstrate a completely displaced extension-type supracondylar humerus fracture. On examination, the child's hand is pink and warm, but the radial pulse is absent. He is taken to the operating room for closed reduction and percutaneous pinning. Following anatomic reduction and secure pinning, the hand remains pink, warm, and well-perfused with brisk capillary refill, but the radial pulse remains absent. What is the most appropriate next step in management?
Explanation
Question 77
A 7-year-old child with spastic diplegic cerebral palsy undergoes comprehensive 3D gait analysis. The kinematic data reveals a characteristic stiff-knee gait with significantly decreased peak knee flexion during the swing phase. Spasticity and overactivity of which of the following muscles is primarily responsible for this gait abnormality?
Explanation
Question 78
A 6-week-old infant with developmental dysplasia of the hip is being treated with a Pavlik harness. During a routine follow-up visit at 2 weeks post-application, the mother notes that the child is no longer actively kicking the affected leg. Examination reveals decreased active extension of the knee on the affected side, though sensory responses appear intact. Which of the following is the most appropriate next step in management?
Explanation
Question 79
A 13-year-old obese boy presents with severe right groin pain after a minor slip. He is unable to bear weight on the affected limb, even with the assistance of crutches. Radiographs demonstrate a right slipped capital femoral epiphysis (SCFE) with a 45-degree slip angle. According to the Loder classification, what specific clinical factor in this patient is associated with the highest risk of developing avascular necrosis (AVN) of the femoral head?
Explanation
Question 80
An 8-year-old boy presents with a painless limp of 3 months duration. Radiographs show sclerosis and fragmentation of the femoral head consistent with Legg-Calvé-Perthes disease.
According to the Herring lateral pillar classification, which of the following radiographic findings determines the poorest prognosis for subsequent femoral head sphericity?
Explanation
Question 81
A 3.5-year-old boy who was successfully treated in infancy for bilateral idiopathic clubfoot using the Ponseti method presents with a recurrent deformity. On physical examination, he demonstrates dynamic supination of the foot during the swing phase of gait. Passive range of motion demonstrates that the foot is fully correctable without fixed equinus or cavus. What is the most appropriate next step in management?
Explanation
Question 82
A 4-year-old otherwise healthy boy sustains an isolated midshaft transverse femur fracture after a fall from a trampoline. He weighs 16 kg (35 lbs). Shortening is measured at 1.5 cm on initial radiographs. What is the most appropriate definitive management for this patient?
Explanation
Question 83
A 2-year-old girl is evaluated for multiple recurrent fractures after minimal trauma. On clinical examination, she has blue sclerae and evidence of dentinogenesis imperfecta. Genetic testing confirms a mutation in the COL1A1 gene. The pathophysiologic basis of her condition primarily involves a quantitative or qualitative defect in the synthesis of which of the following?
Explanation
Question 84
A 4-year-old boy with a BMI in the 99th percentile presents with progressively worsening severe bowing of his left leg. Radiographs demonstrate an abrupt angulation at the proximal medial tibial metaphysis with a metaphyseal-diaphyseal angle (Drennan angle) of 18 degrees.
The radiographic appearance is consistent with a Langenskiöld stage III lesion. Observation over the last year has shown clear progression. What is the most appropriate surgical management?
Explanation
Question 85
A 14-year-old boy presents with recurrent right ankle sprains and deep, aching midfoot pain that worsens with sporting activities. On physical examination, he has pes planus, a rigid subtalar joint, and valgus heel alignment. When asked to stand on his tiptoes, his right heel fails to invert. Lateral radiographs reveal an elongated anterior process of the calcaneus (the 'anteater nose' sign). Which of the following plain radiographic views is most specifically diagnostic for confirming the suspected condition?
Explanation
Question 86
A 6-week-old female is currently being treated with a Pavlik harness for a dislocated left hip. During a follow-up visit after 2 weeks of treatment, the mother reports that the infant is not kicking her left leg as vigorously as the right. Physical examination reveals decreased active extension of the left knee, while ankle and toe movements remain symmetric and normal. What is the most likely cause of this physical finding?
Explanation
Question 87
A 12-year-old obese boy presents to the emergency department with acute left hip pain and an inability to bear weight after a minor fall 2 days ago. Radiographs demonstrate a severe, displaced slipped capital femoral epiphysis (SCFE) on the left side. He is completely unable to bear weight even with crutches. According to the Loder classification, this specific presentation is associated with a significantly increased risk of which of the following complications?
Explanation
Question 88
A 6-year-old boy falls from the monkey bars and sustains a widely displaced, extension-type supracondylar humerus fracture. Upon initial presentation, his hand is pink and warm, with a capillary refill of less than 2 seconds, but the radial pulse is not palpable. He undergoes immediate closed reduction and percutaneous pinning. Post-operatively in the recovery room, his hand remains pink and warm, but the radial pulse is still absent. What is the most appropriate next step in management?
Explanation
Question 89
A 9-year-old boy with spastic diplegic cerebral palsy is evaluated for a worsening crouch gait. He has a history of prior bilateral Achilles tendon lengthenings performed at age 5. Physical exam reveals bilateral knee flexion contractures of 15 degrees. Which of the following findings is most likely to be seen on three-dimensional computerized gait analysis?
Explanation
Question 90
A 3-year-old girl is evaluated for severe bilateral bowlegs. She has a BMI in the 98th percentile. Standing radiographs show an abrupt varus angulation at the proximal tibial metaphysis with a metaphyseal-diaphyseal angle (MDA) of 18 degrees, consistent with Langenskiöld stage II.
What is the most appropriate initial management for this patient?
Explanation
Question 91
A 4-year-old boy treated with the Ponseti method for idiopathic right clubfoot presents with relapsed deformity. The parents report he has been compliant with the bracing protocol. Examination reveals dynamic supination of the foot during the swing phase of gait. Passive range of motion shows completely correctable hindfoot varus and forefoot adduction. Which of the following is the most appropriate surgical intervention?
Explanation
Question 92
A 13-year-old boy presents with severe ankle pain after an external rotation injury while skateboarding. Radiographs reveal a Salter-Harris III intra-articular avulsion fracture of the anterolateral aspect of the distal tibial epiphysis (Tillaux fracture). The fracture pattern observed is directly related to the normal physiological pattern of physeal closure in the distal tibia. In what sequence does the distal tibial physis normally close?
Explanation
Question 93
A 14-year-old boy complains of worsening distal femur pain for 3 months, predominantly occurring at night and unassociated with activity. Radiographs demonstrate a mixed lytic and sclerotic lesion in the distal femoral metaphysis with a distinct 'sunburst' periosteal reaction.
In addition to securing a core needle biopsy, understanding the genetic basis is crucial. Which of the following genetic alterations is most strongly associated with the pathogenesis of this patient's likely diagnosis?

Explanation
Question 94
A 12-year-old boy presents with frequent ankle sprains and chronic vague foot pain. Examination reveals rigid, flat feet bilaterally with severely restricted subtalar motion. The peroneal tendons are noted to be spastic. Lateral radiographs reveal an elongated anterior process of the calcaneus (the 'anteater nose' sign).
Which of the following represents the most appropriate initial management for this condition?

Explanation
Question 95
An 8-year-old boy presents with a 4-month history of a painless limp. Examination shows restricted hip abduction and internal rotation. AP and frog-leg lateral pelvis radiographs show sclerosis, flattening, and fragmentation of the right femoral head.
Which of the following clinical or radiographic factors indicates the worst prognosis for this patient?

Explanation
Question 96
A 12-year-old obese boy presents with sudden inability to bear weight on the left leg after a minor fall. He had been experiencing vague left thigh pain for 3 weeks prior to the fall. On physical examination, the left hip is held in external rotation and he is entirely unable to ambulate even with crutches. Radiographs show a severe posterior and inferior displacement of the proximal femoral epiphysis. He undergoes urgent in-situ pinning with a single cannulated screw. Based on his presentation, which of the following complications is he at the highest risk for developing compared to a patient who is able to bear weight?
Explanation
Question 97
A 5-year-old girl falls from monkey bars and sustains a Gartland type III supracondylar humerus fracture
. On presentation to the emergency department, her hand is pink and well-perfused with a capillary refill of 2 seconds, but the radial pulse is not palpable. She undergoes emergent closed reduction and percutaneous pinning. In the recovery room, her hand remains pink and warm, but the radial pulse remains absent on palpation and Doppler ultrasound. What is the most appropriate next step in management?
Explanation
Question 98
A 4-week-old female infant is being treated with a Pavlik harness for developmental dysplasia of the left hip (DDH). At her 1-week follow-up visit, the mother reports that the infant is no longer kicking her left leg. On examination, the hip remains successfully reduced, but there is absent active extension of the left knee. Sensation to a light pinprick on the anterior thigh appears diminished compared to the contralateral side. What is the most appropriate management of this complication?
Explanation
Question 99
A 3-year-old boy presents with a history of 4 low-energy fractures. Physical examination reveals blue sclerae, joint hyperlaxity, and mild dentinogenesis imperfecta. Genetic testing confirms a mutation in the COL1A1 gene. The patient is initiated on intravenous pamidronate therapy. Which of the following best describes the expected radiographic changes following treatment and the specific cellular mechanism of this medication?
Explanation
Question 100
A 7-year-old boy with spastic quadriplegic cerebral palsy (GMFCS Level IV) is evaluated for bilateral hip pain that interferes with seating and perineal hygiene. An anteroposterior pelvic radiograph demonstrates a right hip Reimers migration percentage of 55%, a broken Shenton's line, and an acetabular index of 35 degrees. The left hip shows a migration percentage of 20% with normal acetabular parameters. What is the most appropriate surgical management for the right hip?
Explanation
None
