Orthopedic Pediatrics 2026 MCQs: Board Review Questions & Answers (Part 1)
Key Takeaway
Learn more about Orthopedic Pediatrics 2026 MCQs: Board Review Questions & Answers (Part 1) and how to manage it. Top-rated Orthopedic Pediatrics 2026 MCQs bank. Practice with clinical case questions, orthopedic surgery board review, and evidence-based answers updated for 2026.
Orthopedic Pediatrics 2026 MCQs: Board Review Questions & Answers (Part 1)
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
The inheritance of the deformity shown in Figure 1 is most commonly
Explanation
Question 2
Examination of a 12-year-old girl with bilateral anterior knee pain reveals excessive femoral anteversion and excessive external tibial torsion. The patient has no patellofemoral instability. Nonsurgical management consisting of muscle strengthening and nonsteroidal medication has failed to relieve the patient's pain. Treatment should now consist of
Explanation
Question 3
Which of the following patients with cerebral palsy is considered the ideal candidate for a selective dorsal rhizotomy?
Explanation
Question 4
A 3-year-old boy sustains a complete paralysis following a high thoracic spinal cord injury consistent with a SCIWORA-type injury (spinal cord injury without radiographic abnormality). Subsequent progressive spinal deformity will develop in what percent of patients with this injury?
Explanation
Question 5
A 12-year-old girl has progressive development of cavus feet. Examination reveals slightly diminished vibratory sensation on the bottom of the foot. Reflexes are 1+ at the knees and ankles. Motor examination shows that all muscles are 5/5 in the foot, except the peroneal and anterior tibial muscles are rated as 4+/5. Which of the following studies is considered most diagnostic?
Explanation
Question 6
A 2-year-old girl was born with the toe deformity shown in Figure 2. She has difficulty wearing shoes despite having adequate room in the toe box. Management at this time should consist of
Explanation
Question 7
Figure 3 shows the radiograph of an asymptomatic 10-year-old boy. Management should consist of
Explanation
Question 8
A 12-year-old girl has had lower back pain for the past 6 months that interferes with her ability to participate in sports. She denies any history of radicular symptoms, sensory changes, or bowel or bladder dysfunction. Examination reveals a shuffling gait, restriction of forward bending, and tight hamstrings. Radiographs show a grade III spondylolisthesis of L5 on S1, with a slip angle of 20 degrees. Management should consist of
Explanation
Question 9
Figures 4a through 4c show the clinical photographs and radiographs of a 12-month-old boy who has progressive difficulty wearing shoes because of the length of the second toe, as well as width of the forefoot. Management should consist of
Explanation
Question 10
Figures 5a and 5b show the radiographs of an 11-year-old boy who felt a pop and immediate pain in his right knee as he was driving off his right leg to jam a basketball. Examination reveals that the knee is flexed, and the patient is unable to actively extend it or bear weight on that side. There is also a large effusion. Management should include
Explanation
Question 11
A 2-year-old child has been referred for management of congenital kyphosis. Neurologic examination is normal, and radiographs show a type I congenital kyphosis. Which of the following anomalies is seen in the MRI scan shown in Figure 6?
Explanation
Question 12
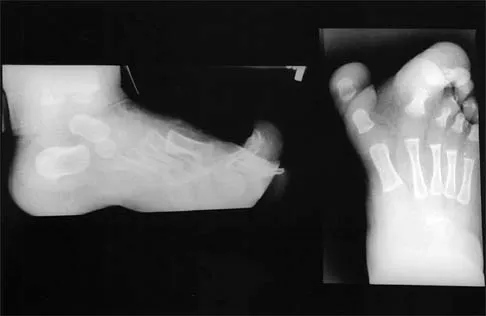
A 15-year-old boy with a type I hereditary sensory motor neuropathy (Charcot-Marie-Tooth disease) reports recurrent ankle sprains and significant pain in the hindfoot and midfoot despite orthotic management. Examination reveals that he walks with a drop foot and has dynamic clawing of the toes. Clinical photographs of the left foot are shown in Figure 7. Management should consist of
Explanation
Question 13
Figures 8a through 8d show the radiographs and CT scans of a 14-year-old girl who has a painful, rigid planovalgus foot. Management consisting of arch supports and anti-inflammatory drugs failed to provide relief. A below-knee walking cast resulted in pain resolution, but she now reports that the pain has recurred. Management should now consist of
Explanation
Question 14
Figures 9a and 9b show the spinal radiographs of a 3-year-old child with short limb dwarfism. The lateral radiograph is obtained with maximal lumbar extension. Management should consist of
Explanation
Question 15
A 10-year-old boy with severe hemophilia A (factor VIII) sustained an injury to his right forearm 2 hours ago when a classmate fell on his arm during a scuffle. Examination reveals moderate swelling in the forearm, decreased sensation in the distribution of the median and ulnar nerves, and pain on passive extension of the fingers. What is the most appropriate sequence of treatment?
Explanation
Question 16
Figures 10a and 10b show the radiographs of an athletic 9-year-old boy who has activity-related anterior knee pain with intact active knee extension. Examination reveals tenderness to palpation over the inferior pole of the patella. There is no effusion or ligamentous instability. Initial management should consist of
Explanation
Question 17
A 2-week-old infant has been referred for evaluation of nonmovement of the left hip. History reveals that the patient was delivered 6 weeks premature by cesarean section. Examination reveals no fever, and there is mild swelling of the thigh. Passive movement of the hip appears to elicit tenderness and very limited hip motion. A radiograph of the pelvis shows mild subluxation of the left hip. The next step in evaluation should consist of
Explanation
Question 18
Figure 11 shows the lateral radiograph of a 16-year-old boy who has been unable to participate in sports activities because of pain in the anterior aspect of the knee. He states that the pain is aching in nature and is located in the region of the tibial tuberosity. He denies having joint effusion or symptoms of instability. Management should consist of
Explanation
Question 19
A 10-lb, 2-oz infant who was born via a difficult breech delivery 12 hours ago is now being evaluated for hip pain. Although the infant is resting comfortably, examination reveals that the patient is not moving the right lower extremity and manipulation of the right hip causes the infant to cry. The Galeazzi sign is positive. An AP radiograph of the pelvis shows proximal and superior migration of the right proximal femoral metaphysis. What is the most likely diagnosis?
Explanation
Question 20
A 10-year-old girl has been referred for evaluation of a prominence at the lower cervical spine. The patient is asymptomatic, and the examination reveals no evidence of neurologic abnormality. A radiograph and CT scans are shown in Figures 12a through 12c. What is the most likely diagnosis?
Explanation
Question 21
Which of the following types of iliac osteotomy provides the greatest potential for increased coverage?
Explanation
Question 22
The mother of a 26-month-old boy reports that he has been unwilling to bear weight on his left lower extremity since he awoke this morning. She denies any history of trauma. He has a temperature of 99.4 degrees F (37.4 degrees C), and examination reveals that abduction of the left hip is limited to 30 degrees. Laboratory studies show a WBC of 11,000/mm3 and an erythrocyte sedimentation rate of 22 mm/h. A radiograph of the pelvis is shown in Figure 13. Management should consist of
Explanation
Question 23
A 10-year-old girl with a monoarticular pattern of juvenile rheumatoid arthritis (JRA) has had a 3-cm limb-length discrepancy since age 8 years when inflammation in the right knee came under good medical control. Because her right leg is longer, the patient states that she would like her legs to be close to equal in length in the future. A growth-remaining chart is shown in Figure 14. Management should consist of
Explanation
Question 24
A 14-year-old girl with polyarticular juvenile rheumatoid arthritis (JRA) has severe neck pain and reports the onset of urinary incontinence. A lateral radiograph and lateral tomogram of the cervical spine are shown in Figures 15a and 15b. An MRI scan of the upper cervical spine is shown in Figure 15c. Management should consist of
Explanation
Question 25
Figures 16a and 16b show the radiographs of an otherwise healthy 3 1/2-year-old boy who has an isolated deformity of the left leg. Definitive primary treatment of this condition should consist of
Explanation
Question 26
A 6-year-old boy presents with a Gartland type III supracondylar humerus fracture. The hand is pink but pulseless. After closed reduction and percutaneous pinning, the hand remains pink and pulseless. What is the most appropriate next step in management?
Explanation
Question 27
A 4-year-old child presents with untreated unilateral developmental dysplasia of the hip. Which of the following surgical interventions is most commonly required to achieve and maintain a stable reduction?
Explanation
Question 28
A 12-year-old obese boy presents with left knee pain and an antalgic gait. Radiographs reveal a severe slipped capital femoral epiphysis (SCFE) with a slip angle of 60 degrees. After in situ pinning of the left hip, which of the following is the most accepted indication for prophylactic pinning of the contralateral asymptomatic hip?
Explanation
Question 29
A 7-year-old boy is diagnosed with Legg-Calvé-Perthes disease. Radiographs demonstrate >50% loss of lateral pillar height. According to the Herring lateral pillar classification, what is the expected outcome without surgical intervention?
Explanation
Question 30
During the initial casting for an infant with a rigid idiopathic clubfoot using the Ponseti method, what is the first deformity that must be corrected?
Explanation
Question 31
A 6-year-old boy falls from monkey bars and sustains a Gartland Type III supracondylar humerus fracture. On examination, the radial pulse is absent, but the hand is warm, pink, and has a capillary refill of less than 2 seconds. After prompt closed reduction and percutaneous pinning, the pulse remains absent but the hand remains well-perfused. What is the most appropriate next step?
Explanation
Question 32
A 2-year-old child presents with bilateral genu varum. Radiographs reveal medial metaphyseal beaking of the proximal tibia. Which of the following radiographic measurements most reliably differentiates infantile Blount disease from physiologic bowing?
Explanation
Question 33
A 3-year-old boy with multiple recurrent fractures, blue sclerae, and dentinogenesis imperfecta is diagnosed with osteogenesis imperfecta. This condition is most commonly caused by a mutation affecting which of the following?
Explanation
Question 34
An infant with achondroplasia presents with central sleep apnea, hyperreflexia, and hypotonia. These clinical findings are most likely secondary to which of the following complications?
Explanation
Question 35
A 6-year-old child with spastic quadriplegic cerebral palsy has a migration percentage of 45% on an AP pelvis radiograph. He has pain with hip range of motion and limited abduction. What is the most appropriate surgical management?
Explanation
Question 36
A 3-year-old boy treated for idiopathic clubfoot with the Ponseti method presents with a recurrence of the deformity. Examination reveals dynamic supination of the foot during the swing phase of gait. Passive range of motion demonstrates fully correctable deformities. What is the most appropriate next step in management?
Explanation
Question 37
A 6-year-old boy sustains a completely displaced posterolateral supracondylar humerus fracture. Upon presentation, he has a pulseless but well-perfused (pink) hand. Closed reduction and percutaneous pinning are performed, achieving an anatomic reduction. Postoperatively, the hand remains pink but the radial pulse is still absent. What is the most appropriate management?
Explanation
Question 38
A 6-week-old female is undergoing treatment with a Pavlik harness for developmental dysplasia of the hip (DDH). During the follow-up visit, the parents report that the child has stopped moving her left leg. Examination reveals decreased active knee extension and an absent patellar reflex on the left side. What is the most likely cause of this finding?
Explanation
Question 39
An 11-year-old boy presents with a 4-week history of left groin pain and a limp. Radiographs confirm a mild, stable slipped capital femoral epiphysis (SCFE) of the left hip. The right hip is radiographically normal. Which of the following is the strongest indication for prophylactic pinning of the contralateral (right) hip?
Explanation
Question 40
A 10-year-old girl is evaluated for a leg length discrepancy following a distal femoral physeal fracture 2 years ago. A scanogram reveals the injured limb is 3 cm shorter than the normal limb. Based on the multiplier method, her predicted leg length discrepancy at maturity is 4.5 cm. Which of the following is the most appropriate surgical management plan?
Explanation
Question 41
A 7-year-old boy with spastic diplegic cerebral palsy with GMFCS level III presents with a progressive crouch gait. Physical examination reveals fixed knee flexion contractures of 15 degrees bilaterally. Which of the following interventions is most appropriate to address this specific deformity?
Explanation
Question 42
A 3-year-old girl is diagnosed with congenital scoliosis secondary to a fully segmented hemivertebra at T8. The curve is currently 35 degrees. Renal ultrasound and echocardiogram are normal. An MRI of the entire spine is obtained. What is the most common intraspinal anomaly associated with this condition?
Explanation
Question 43
A 6-year-old boy with Sillence Type III osteogenesis imperfecta presents with progressive anterolateral bowing of his bilateral femurs, leading to an inability to ambulate. He has been receiving IV pamidronate for 2 years. Which of the following surgical strategies is most appropriate?
Explanation
Question 44
A newborn male is noted to have unilateral foreshortening of the right lower extremity. Radiographs reveal complete absence of the fibula, a shortened tibia with anterior bowing, and a 3-ray foot. Which of the following knee anomalies is most commonly associated with this presentation?
Explanation
Question 45
A 10-year-old girl falls while skiing and sustains a Type III (completely displaced) tibial eminence fracture. Closed reduction under anesthesia is attempted but is unsuccessful in achieving an acceptable reduction. What is the most likely anatomic structure blocking the reduction?
Explanation
Question 46
A 4-year-old boy presents with right hip pain, a temperature of 38.8°C (101.8°F), inability to bear weight, and a WBC count of 14,000/mm3. ESR is 55 mm/hr. According to the Kocher criteria, what is the approximate probability that this child has septic arthritis rather than transient synovitis?
Explanation
Question 47
A 3-year-old boy presents to the emergency department with a spiral fracture of the midshaft femur. He was reportedly running and tripped over a rug. The parents delayed bringing him in for two days. Upon examination, there are multiple bruises in various stages of healing on his back. What is the next most appropriate step in management regarding the mechanism of injury?
Explanation
Question 48
A 7-year-old boy is diagnosed with early-stage Legg-Calvé-Perthes disease. He has a limp and restricted hip abduction. Which of the following factors at the time of presentation is considered the most significant indicator of a poor long-term prognosis?
Explanation
Question 49
A 14-year-old male gymnast presents with persistent lower back pain exacerbated by extension. Radiographs and an MRI confirm a bilateral L5 pars interarticularis defect with a Grade I spondylolisthesis. The pain has not improved after 6 months of rest, bracing, and physical therapy. What is the most appropriate surgical treatment?
Explanation
Question 50
A 12-year-old boy complains of recurrent left ankle sprains and lateral foot pain. On examination, he has a rigid, flat foot and lacks subtalar motion. Radiographs demonstrate a "C-sign" on the lateral view. A CT scan confirms a talocalcaneal coalition involving 25% of the posterior facet. Non-operative management has failed. What is the most appropriate surgical intervention?
Explanation
Question 51
A 4-year-old child with a history of idiopathic clubfoot treated successfully with the Ponseti method presents with a dynamic supination deformity during the swing phase of gait. Passive range of motion of the ankle and foot is full. What is the most appropriate management?
Explanation
Question 52
A 6-month-old girl with Developmental Dysplasia of the Hip (DDH) undergoes closed reduction and spica casting. Which of the following intraoperative positioning parameters is most strongly associated with an increased risk of avascular necrosis (AVN) of the femoral head?
Explanation
Question 53
A 13-year-old obese boy presents with sudden severe right hip pain and inability to bear weight after a minor fall. Radiographs confirm an unstable slipped capital femoral epiphysis (SCFE). What is the primary proposed benefit of performing an urgent capsulotomy and gentle reduction prior to pinning?
Explanation
Question 54
A 7-year-old boy is diagnosed with Legg-Calvé-Perthes disease. Radiographs show radiolucency and fragmentation. The lateral pillar of the femoral head maintains 40% of its original height. According to the Herring Lateral Pillar Classification, what is the grade and expected outcome without surgical containment?
Explanation
Question 55
A 3-year-old boy presents with progressive bilateral genu varum. Standing radiographs reveal metaphyseal-diaphyseal angles of 18 degrees bilaterally, with prominent medial metaphyseal beaking. What is the most appropriate initial management?
Explanation
Question 56
A 5-year-old girl with spastic quadriplegic cerebral palsy (GMFCS Level V) is evaluated for hip surveillance. Her migration percentage (MP) on an AP pelvis radiograph is 45%. Clinically, she has 20 degrees of hip abduction bilaterally. What is the most appropriate management?
Explanation
Question 57
A 6-year-old boy sustains a completely displaced (Gartland Type III) posteromedial supracondylar humerus fracture. On examination, the hand is pink and warm, but the radial pulse is absent. After anatomical closed reduction and percutaneous pinning, the hand remains pink and the pulse remains absent. What is the next best step?
Explanation
Question 58
A 14-year-old boy complains of recurrent ankle sprains and deep lateral hindfoot pain. On examination, he has rigid pes planus and absent subtalar motion. Radiographs demonstrate a continuous bony C-shaped ring on the lateral view. Which of the following is the most likely diagnosis?
Explanation
Question 59
A 14-month-old girl presents with refusal to bear weight on her right leg. She is afebrile with normal inflammatory markers. MRI shows early osteomyelitis in the distal tibial metaphysis. Given her age, what fastidious organism should be highly suspected, and how can its culture yield be optimized?
Explanation
Question 60
A 14-year-old gymnast presents with severe mechanical back pain and L5 radiculopathy. Radiographs reveal a Grade III L5-S1 isthmic spondylolisthesis with a slip angle of 55 degrees. Nonoperative management has failed. What is the most appropriate surgical treatment?
Explanation
Question 61
A 12-year-old premenarcheal girl with a Risser stage of 0 presents with a right thoracic adolescent idiopathic scoliosis (AIS). Her curve measures 30 degrees. Which of the following represents the most appropriate management?
Explanation
Question 62
A 5-year-old boy weighing 22 kg sustains a closed, length-stable diaphyseal transverse fracture of the femur. What is the standard of care for definitive management?
Explanation
Question 63
A 6-year-old girl with Osteogenesis Imperfecta Type III presents with a severely bowed femur and a new midshaft fracture. She has a history of multiple fractures. What is the most appropriate surgical management for this fracture?
Explanation
Question 64
An 8-month-old boy with achondroplasia presents with hypotonia, sleep apnea, and hyperreflexia. An MRI reveals severe stenosis at the foramen magnum with T2 signal changes in the upper cervical cord. What is the most appropriate next step?
Explanation
Question 65
A 12-year-old boy is diagnosed with a unilateral stable slipped capital femoral epiphysis (SCFE). Which of the following factors most strongly supports the decision for prophylactic pinning of the contralateral hip?
Explanation
Question 66
Which of the following is considered the most common extra-articular block to closed reduction in developmental dysplasia of the hip?
Explanation
Question 67
Which of the following factors at presentation is most strongly predictive of developing avascular necrosis following a slipped capital femoral epiphysis (SCFE)?
Explanation
Question 68
An infant with idiopathic clubfoot is being treated via the Ponseti casting method. The foot has been successfully abducted to 60 degrees, but dorsiflexion is limited to neutral. What is the most appropriate next step in management?
Explanation
Question 69
An 8-year-old boy presents with lateral pillar B/C border Legg-Calve-Perthes disease. According to current evidence-based guidelines, what is the most appropriate management?
Explanation
Question 70
A 6-year-old girl sustains a displaced Gartland III supracondylar humerus fracture. On examination, the radial pulse is absent, but the hand is warm, pink, and has capillary refill under 2 seconds. What is the most appropriate initial management?
Explanation
Question 71
A 7-year-old non-ambulatory child with spastic quadriplegic cerebral palsy has a Reimers migration index of 45 percent. Radiographs demonstrate significant coxa valga and acetabular dysplasia. What is the most appropriate surgical intervention?
Explanation
Question 72
A 13-year-old boy develops severe hip pain and progressive loss of motion six months after undergoing in situ single screw fixation for a stable SCFE. Radiographs show significant joint space narrowing. What is the most likely etiology of this complication?
Explanation
Question 73
Which of the following radiographic findings is recognized as one of Catterall's head-at-risk signs in Legg-Calve-Perthes disease?
Explanation
Question 74
A 3-year-old obese girl presents with unilateral genu varum. Radiographs reveal a metaphyseal-diaphyseal (Drennan) angle of 20 degrees. What is the diagnosis and best initial treatment?
Explanation
Question 75
A 2-year-old boy with neurofibromatosis type 1 develops a non-healing fracture of the tibia through an area of anterolateral bowing. Which surgical approach provides the highest union rate for this condition?
Explanation
Question 76
A 14-year-old premenarchal girl (Risser 0) presents with adolescent idiopathic scoliosis. Standing radiographs demonstrate a right thoracic curve of 35 degrees. What is the recommended treatment?
Explanation
Question 77
A 12-year-old boy presents with a rigid flatfoot and recurrent ankle sprains. CT imaging confirms an isolated calcaneonavicular coalition without arthritic changes. After conservative management fails, what is the most appropriate surgical intervention?
Explanation
Question 78
A child presents with short stature, rhizomelic limb shortening, frontal bossing, and a trident hand deformity. What is the most critical and life-threatening cervical spine abnormality associated with this skeletal dysplasia?
Explanation
Question 79
A healthy 3-year-old boy sustains a closed, length-stable, isolated midshaft femur fracture after a fall from a playground slide. What is the recommended definitive treatment?
Explanation
Question 80
A 14-year-old gymnast is diagnosed with an L5-S1 isthmic spondylolisthesis with a 60 percent slip (Grade III). She reports persistent mechanical back pain and L5 radiculopathy despite 6 months of rest and therapy. What is the most appropriate surgical management?
Explanation
Question 81
A 3-year-old girl refuses to bear weight on her right leg for 2 days. Her temperature is 38.8 C, ESR is 50 mm/hr, and peripheral WBC is 14,000. Ultrasound confirms a hip effusion. According to the Kocher criteria, what is the probability of septic arthritis?
Explanation
Question 82
When attempting to differentiate transient synovitis from septic arthritis of the pediatric hip, which laboratory value has been shown to be the strongest independent multivariate predictor for septic arthritis?
Explanation
Question 83
An 11-year-old boy with spastic diplegic cerebral palsy presents with an increasingly severe crouch gait. Examination reveals fixed knee flexion contractures of 20 degrees. What is the most appropriate surgical approach to address the crouch gait?
Explanation
Question 84
A 13-year-old boy has an osteochondritis dissecans (OCD) lesion of the medial femoral condyle. MRI shows a 1.5 cm lesion with intact overlying cartilage and no high T2 signal behind the fragment. His distal femoral physis is wide open. What is the best initial management?
Explanation
Question 85
A 15-year-old male basketball player lands forcefully and avulses his tibial tubercle (Ogden Type III fracture) with intra-articular extension. He undergoes surgical fixation. Which complication is most uniquely concerning in the immediate post-injury period for this specific fracture pattern?
Explanation
Question 86
A 4-month-old infant with developmental dysplasia of the hip has been treated with a Pavlik harness. At the 4-week follow-up, an ultrasound demonstrates that the hip remains dislocated. What is the primary risk of continuing the Pavlik harness in this patient for an additional 3 weeks?
Explanation
Question 87
An 11-year-old boy with a BMI in the 99th percentile presents with 3 weeks of knee pain and a limp. Examination reveals obligate external rotation of the hip with passive flexion. Radiographs confirm a stable slipped capital femoral epiphysis (SCFE). During in situ pinning, where should the single screw be positioned within the epiphysis?
Explanation
Question 88
A 6-year-old boy sustains a completely displaced extension-type supracondylar humerus fracture. On presentation, his hand is pale, pulseless, and cold. After rapid closed reduction and percutaneous pinning, his hand becomes warm and pink, with a capillary refill of 2 seconds, but the radial pulse remains absent. What is the most appropriate next step in management?
Explanation
Question 89
A 2-week-old infant with idiopathic clubfoot is undergoing serial casting using the Ponseti method. The first casting maneuver should primarily aim to correct the cavus deformity. Which of the following describes the correct technique for this initial step?
Explanation
Question 90
An 8-year-old boy presents with a painless limp. Radiographs demonstrate sclerosis and fragmentation of the left capital femoral epiphysis with lateral subluxation. According to the Herring lateral pillar classification, he has a Group B/C lesion. Which of the following factors is the strongest predictor of a poor long-term outcome in this patient?
Explanation
Question 91
A 4-year-old girl with a history of multiple fractures, blue sclerae, and normal dentition is diagnosed with Osteogenesis Imperfecta (OI) type I. Which of the following genetic mechanisms is most likely responsible for her condition?
Explanation
Question 92
A 7-year-old child presents with torticollis and severe neck stiffness one week after undergoing a tonsillectomy. A CT scan confirms atlantoaxial rotatory subluxation. What is the primary pathophysiologic mechanism of this condition (Grisel's syndrome)?
Explanation
Question 93
A 5-year-old girl falls on an outstretched hand and sustains a lateral condyle fracture of the humerus with 1 mm of displacement. She is treated in a long-arm cast. At her 4-week follow-up, radiographs show delayed union but no change in displacement. What is the most appropriate management?
Explanation
Question 94
A 6-year-old boy with spastic quadriplegic cerebral palsy (GMFCS level V) has progressive right hip subluxation with a migration percentage of 55%. He has pain during diaper changes and difficulty sitting. Which of the following surgical interventions is most appropriate?
Explanation
None
