Ace Your Trauma Oral: How to Section the Trauma for Success
Key Takeaway
Discover the latest medical recommendations for Ace Your Trauma Oral: How to Section the Trauma for Success. "Section the trauma" refers to a specific oral examination component in orthopedic medical training, designed to assess a candidate's understanding of trauma cases. This section typically employs various styles, including fast-moving radiographs, detailed questions on surgical approaches, or in-depth discussions on complex management issues encountered in fracture clinics, preparing candidates for exams like the FRCS (Tr & Orth).
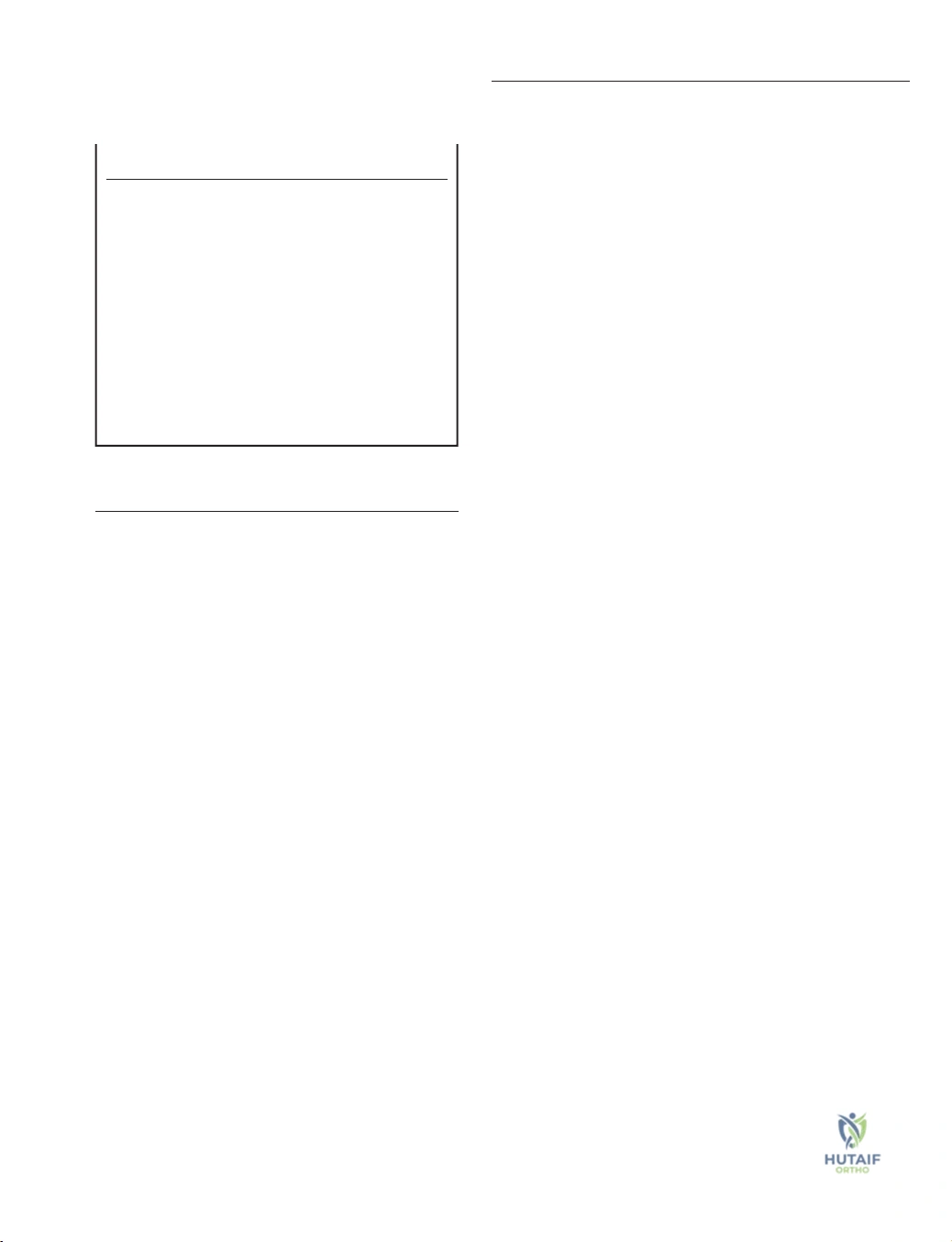
A 35-year-old male presents following a high-energy motorcycle accident. He is hemodynamically stable but has a severely deformed right lower limb. These are his initial trauma radiographs.
Describe your initial assessment and how you would classify this injury to guide your management.
Candidate: I would follow ATLS protocols to ensure no life-threatening injuries. Locally, I would perform a neurovascular assessment, document the skin condition using the Tscherne classification, and assess for compartment syndrome. I would then classify the fracture using the AO system and obtain CT imaging for surgical planning.
Candidates often jump straight to "I would put a nail in this" without mentioning the soft tissue envelope or the "Rule of 2s" (two views, two joints, two occasions). Failing to mention neurovascular status first is a safety-critical error that examiners will penalize immediately.
A structured, consultant-level response: "First, I confirm the patient is ATLS stable. I will perform a secondary survey to rule out occult injuries. Locally, I perform a thorough neurovascular exam, check for compartment syndrome, and grade the soft tissues (Tscherne classification for closed or Gustilo-Anderson for open). I will obtain orthogonal radiographs, and given the articular involvement visible, I would request a CT scan to assess the fracture morphology, particularly the degree of articular depression and comminution, which dictates the surgical approach and the need for structural bone graft."
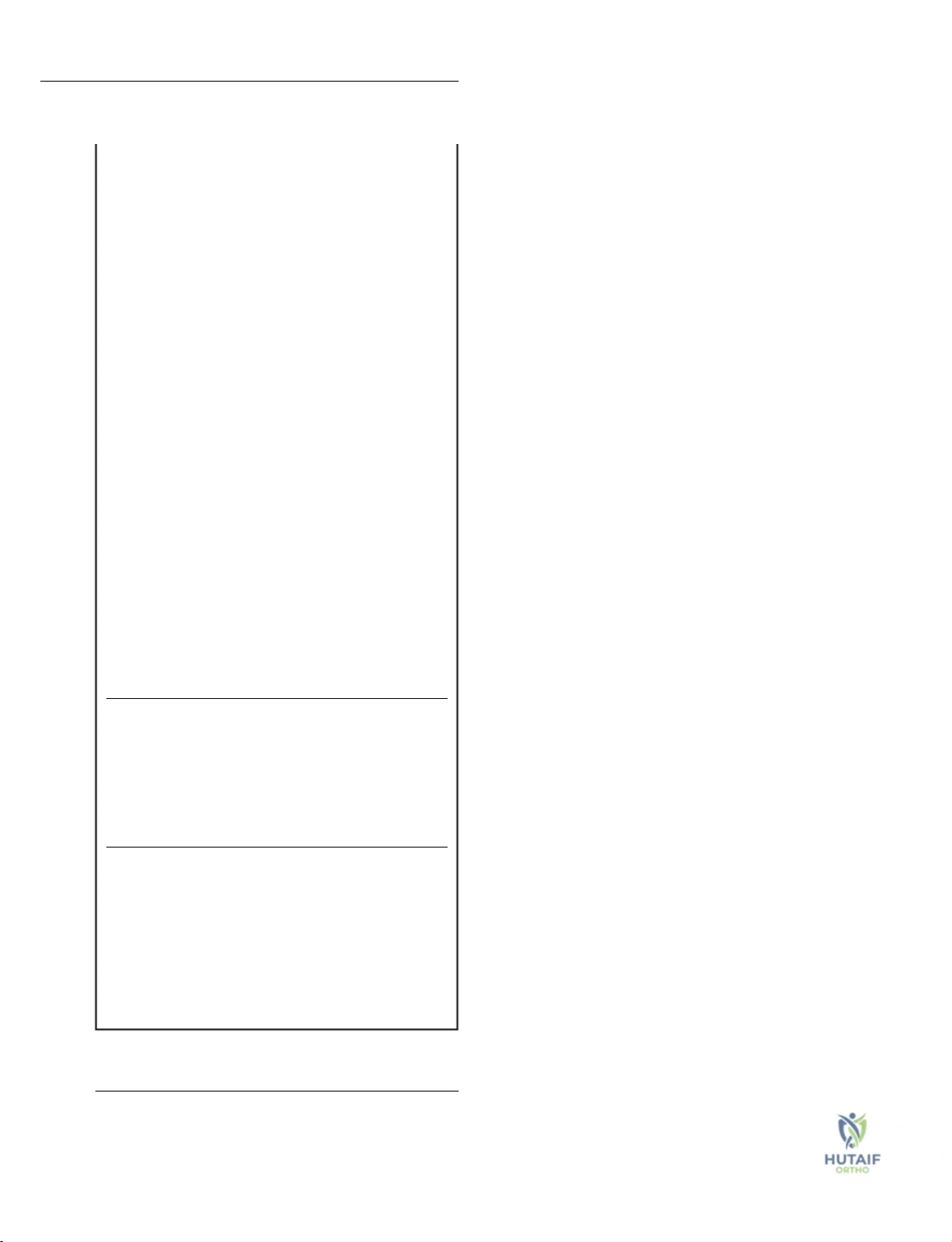
You have decided to proceed with surgery. Describe the biomechanical principles you will employ for the definitive fixation of this articular segment.
Candidate: I would aim for absolute stability. I would use lag screws to achieve interfragmentary compression across the joint surface and then apply a neutralization plate to protect the construct from shear and bending forces.
Candidates failing to mention the difference between absolute and relative stability or forgetting to mention the "neutralization" aspect of the plate. Another major error is ignoring the role of the metaphyseal-diaphyseal extension.
Explicitly reference Perren’s Strain Theory: "Articular fractures mandate absolute stability to achieve primary bone healing without callus, which would otherwise lead to joint incongruity. I will use interfragmentary lag screws to generate compression by gliding through the near cortex. I will then apply a plate in neutralization mode to prevent bending and shear. If there is significant comminution in the metaphysis, I must transition from absolute stability at the joint to relative stability (bridge plating) in the metaphysis to allow for secondary healing, carefully managing the working length of the plate to avoid fatigue failure."
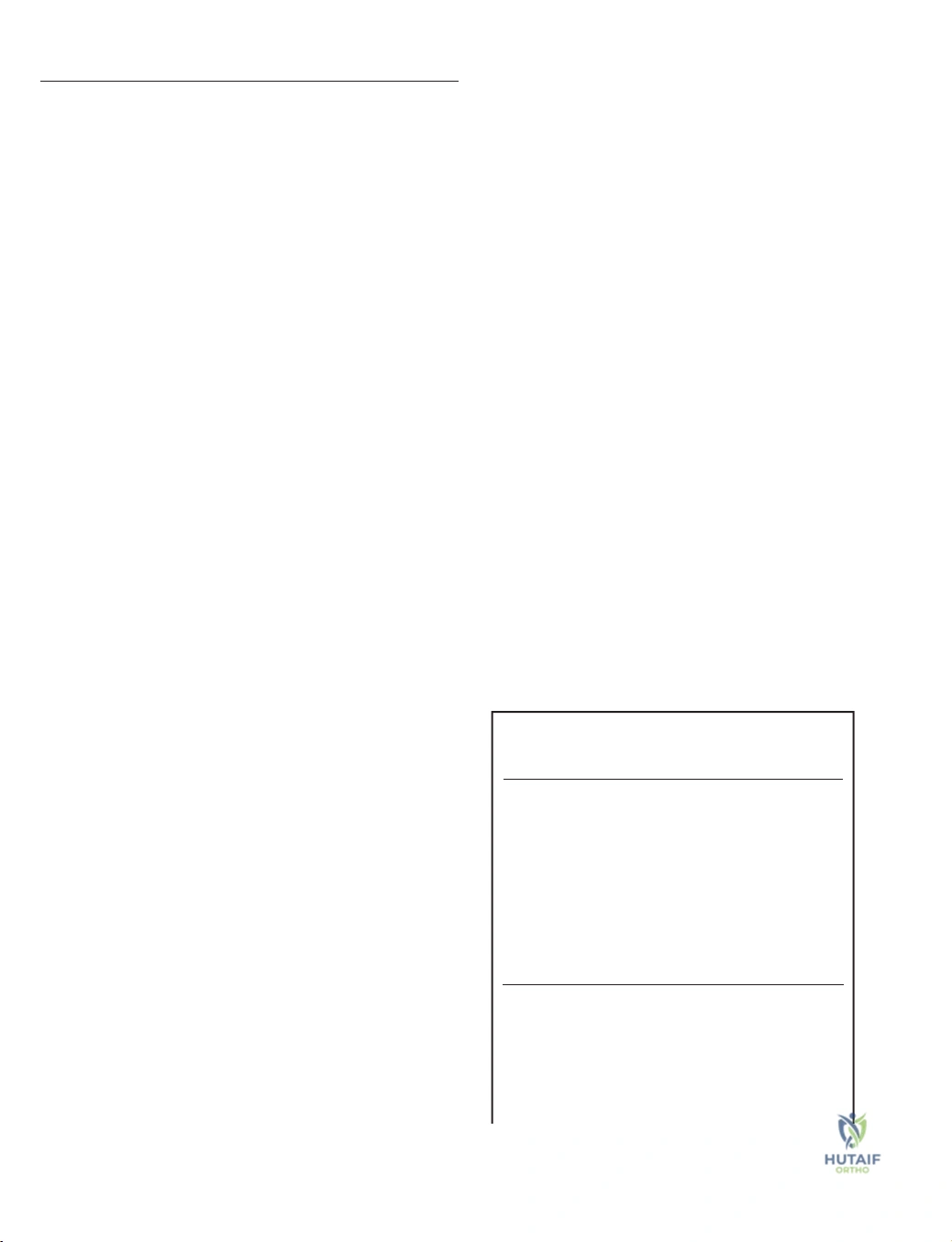
The surgery goes well, but at the 6-month follow-up, the patient presents with these findings.

What is your diagnosis and how would you manage this complication?
Candidate: The radiograph shows a non-union with hardware failure. I would suspect it is atrophic and would recommend revising the fixation and adding bone graft.
Jumping into a surgical plan without determining the *type* of non-union. If you don't rule out infection (e.g., blood markers, aspirate) first, you are deemed unsafe.
"First, I must rule out occult infection—I would perform clinical examination (sinus, erythema), inflammatory markers (CRP/ESR), and consider aspiration. Assuming it is sterile: I classify this as an atrophic non-union due to the lack of callus. My management is a biological and mechanical 'reset': I will perform a debridement of the non-union site, apply stable internal fixation (likely a larger or longer construct to address the mechanical failure), and add autologous bone graft (iliac crest or RIA) to promote biological healing. I would also consider BMP-2 if indicated by the patient's comorbidities."
