Floating Knee Injuries: Comprehensive Review of Etiology, Anatomy, and Management
Key Takeaway
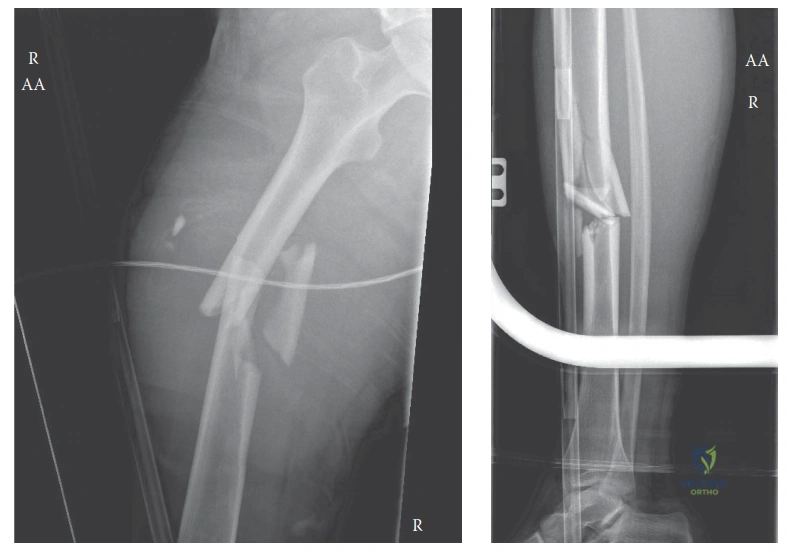
A floating knee injury involves severe ipsilateral fractures of the femur and tibia, typically from high-energy trauma. Classified by Fraser, these complex injuries demand meticulous assessment due to inherent instability, extensive soft tissue damage, and high rates of neurovascular compromise. Management is primarily operative, often via damage control orthopedics, to restore alignment and prevent complications.
A 32-year-old male is brought to the trauma bay following a high-speed motorcycle collision. He is hemodynamically stable. Examination of the left lower limb shows gross deformity of the thigh and proximal leg, with significant swelling. There is a 3cm laceration at the level of the tibial tuberosity. The distal foot is pale and pulseless. How do you approach the initial assessment and stabilization of this patient?
Candidate: I would follow ATLS protocols to ensure systemic stability. Given the pulseless foot, this is a limb-threatening emergency. I would perform an immediate reduction and splinting of the limb to restore perfusion. If pulses remain absent, I would request an urgent vascular surgery consult, order a CT angiogram, and prepare for theatre for fracture stabilization and vascular repair.
Failing to emphasize the urgency of the vascular status by jumping straight to radiographic classification (Fraser/Schatzker). Candidates often forget that a pulseless limb is an emergency that overrides standard workup—delay for "standard" imaging can result in irreversible ischemia.
I would approach this as a limb-threatening emergency. 1. Systemic Assessment: Confirm ATLS primary survey to rule out polytrauma. 2. Vascular Triage: A pulseless limb requires emergent restoration of perfusion. I would perform immediate manual traction and reduction to potentially restore flow (relieving kinking of the popliteal artery). 3. Immediate Decision: If pulses return, I proceed to emergent formal assessment (CTA). If they remain absent, the patient goes to the OR for urgent vascular exploration and skeletal stabilization (Damage Control Orthopedics). 4. Documentation: Meticulous neurovascular charting is mandatory before and after any manipulation.
The patient has been stabilized. You are now planning definitive internal fixation for this "floating knee" (ipsilateral femur and tibia fracture). What factors influence your choice of sequence and fixation strategy?
Candidate: I would usually fix the femur first because it restores the mechanical axis and soft tissue tension, which helps in reducing the tibia. For the femur, I would prefer an intramedullary nail, and for the tibia, I would use an IM nail or a plate depending on the articular involvement.
Providing a "one-size-fits-all" answer. Failing to distinguish between Fraser Type I (extra-articular) and Fraser Type II (intra-articular) injuries. A borderline candidate will fail to mention that the articular fragments dictate the need for plates vs. nails.
My strategy is dictated by the Fraser Classification: 1. Sequence: Femoral fixation first allows for tensioning of the soft tissue sleeve, facilitating tibial reduction. 2. Fixation Selection: For diaphyseal fractures, intramedullary nailing is the gold standard (load-sharing). For Fraser Type II intra-articular injuries, I prioritize anatomical reconstruction of the joint surface using lag screws and buttress plates. 3. Damage Control: If the patient is physiologically "borderline," I would utilize external fixation as a damage control bridge to avoid the "second hit" of prolonged surgery, delaying definitive fixation for 3-10 days.
The patient is 6 months post-fixation. He presents with persistent knee stiffness and radiographic evidence of post-traumatic arthritis in the tibial plateau. How do you discuss the prognosis and management with him?
Candidate: I would tell him that stiffness is very common after these injuries. I would refer him for aggressive physiotherapy and hydrotherapy. If the arthritis becomes unbearable, I might discuss a total knee replacement in the future, although it is a difficult surgery due to the previous hardware.
Focusing only on the end-stage (TKA) and ignoring the joint-preserving options or the reality of the patient's functional deficit. Candidates often fail to address the psychosocial aspect of a young patient facing a long-term disability.
I would adopt a structured, long-term approach: 1. Counseling: Acknowledge that the "floating knee" is a major life-altering injury with high rates of long-term morbidity (up to 50% post-traumatic arthritis). 2. Staged Management: - Short-term: Focus on stiffness with arthrolysis or manipulation under anesthesia if therapy plateaus. - Medium-term: Activity modification, pain management, and intra-articular injections. 3. Long-term: If symptomatic arthritis progresses, we consider joint-preserving osteotomy if malalignment is present, or total knee arthroplasty (TKA). I would warn him that TKA after high-energy trauma is challenging due to scarring, hardware, and potentially compromised soft tissues, necessitating a multidisciplinary approach.
