Mastering Acute Joint Dislocations and Ligamentous Reconstruction
Key Takeaway
Acute joint dislocations require immediate, evidence-based intervention to restore biomechanical stability and prevent long-term sequelae such as post-traumatic osteoarthritis or avascular necrosis. This guide details the operative management of complex dislocations—including the patella, knee, hip, and acromioclavicular joints—while providing a step-by-step masterclass on the Liebolt technique for distal radioulnar joint (DRUJ) stabilization.
Comprehensive Introduction and Patho-Epidemiology
The management of acute joint dislocations represents a critical, high-stakes pillar of operative orthopaedics. From the foundational principles established by pioneers such as Böhler and Watson-Jones to the advent of modern arthroscopic and MRI-guided interventions, the primary objective remains unchanged: to achieve a concentric, perfectly stable reduction while minimizing iatrogenic soft-tissue trauma. Joint dislocations are rarely isolated osseous events; they are fundamentally devastating soft-tissue injuries that compromise the capsuloligamentous envelope, neurovascular structures, and articular cartilage. Failure to recognize subtle instability patterns or associated osteochondral shear injuries inevitably leads to chronic instability, post-traumatic arthrosis, and profound functional impairment that can permanently alter a patient's quality of life.
The patho-epidemiology of acute joint dislocations spans a broad spectrum of energy mechanisms. In the young, active population, we frequently encounter sports-related trauma resulting in acute patellar dislocations, acromioclavicular (AC) joint separations, and complex distal radioulnar joint (DRUJ) instability. These injuries are typically the result of indirect twisting forces or direct, localized blows. Conversely, high-energy trauma, such as motor vehicle collisions or falls from significant heights, precipitates catastrophic injuries like traumatic hip dislocations and multi-ligamentous knee injuries (MLKI). In these high-energy scenarios, the sheer force required to displace a major weight-bearing joint dictates that the surrounding soft-tissue envelope will sustain massive disruption, demanding a high index of suspicion for occult neurovascular compromise and compartment syndrome.
Understanding the temporal dynamics of joint reduction is paramount. The concept of the "golden window" dictates that the longer a joint remains dislocated, the higher the risk of irreversible complications. For instance, traumatic hip dislocations carry an exponentially increasing risk of avascular necrosis (AVN) of the femoral head if reduction is delayed beyond six hours. Similarly, the dislocated knee is a true vascular emergency; the popliteal artery's tethering points make it highly susceptible to intimal tearing or complete transection, where delayed revascularization invariably leads to limb amputation. Thus, the orthopaedic surgeon must operate with extreme urgency during the acute phase, seamlessly transitioning from acute resuscitation and reduction to meticulous, definitive ligamentous reconstruction.
This comprehensive masterclass synthesizes decades of peer-reviewed literature to provide a definitive, textbook-level guide on the management of complex joint dislocations. We will explore the nuanced biomechanics, evidence-based surgical indications, and advanced operative techniques required to address instability in the distal radioulnar joint (DRUJ), patellofemoral joint, knee, proximal tibiofibular joint, hip, and acromioclavicular (AC) joint. Mastery of these concepts is essential for any orthopaedic surgeon tasked with restoring anatomic stability and preserving joint longevity in the face of severe musculoskeletal trauma.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of joint-specific surgical anatomy and biomechanics is the absolute prerequisite for successful ligamentous reconstruction. In the upper extremity, the distal radioulnar joint (DRUJ) is a highly complex diarthrodial joint that relies heavily on both intrinsic and extrinsic stabilizers. The primary intrinsic stabilizer is the triangular fibrocartilage complex (TFCC), specifically the deep fibers (ligamentum subcruentum) that insert into the fovea at the base of the ulnar styloid. This foveal attachment represents the anatomic isometric point of the DRUJ, allowing the radius to rotate around the fixed ulna without significant changes in ligamentous tension. Extrinsic stability is provided by the extensor carpi ulnaris (ECU) subsheath, the pronator quadratus, and the interosseous membrane. Disruption of these structures alters the normal load transmission across the wrist, leading to ulnar-sided pain, weakness in grip strength, and progressive arthrosis.
The patellofemoral joint represents a complex interplay of static and dynamic stabilizers. The medial patellofemoral ligament (MPFL) is the primary static restraint to lateral patellar translation, contributing up to 60% of the restraining force from 0 to 30 degrees of knee flexion. The MPFL originates from a highly specific anatomic location on the medial femur, known as Schöttle's point, which is located anterior to the posterior femoral cortex line, proximal to the Blumensaat line, and distal to the medial epicondyle. It inserts onto the proximal two-thirds of the medial patellar border. Dynamically, the vastus medialis obliquus (VMO) provides active medial tracking during early flexion. Biomechanically, MPFL ruptures typically occur at the femoral origin, though mid-substance and patellar avulsions are also observed. Understanding the isometric behavior of the MPFL is critical; it is taut in full extension and early flexion, gradually relaxing as the patella engages the trochlear groove.
In the context of the knee and proximal tibiofibular joint, the anatomy is defined by its vulnerability to neurovascular injury. A true tibiofemoral dislocation involves the disruption of at least two, and often three or four, of the major knee ligaments (ACL, PCL, MCL, LCL/PLC). The paramount anatomic concern is the popliteal artery, which is rigidly tethered proximally at the adductor hiatus and distally at the soleus arch. This lack of mobility makes the artery exceptionally prone to traction injuries during hyperextension or posterior translation forces. Adjacent to this, the common peroneal nerve wraps around the fibular neck, placing it at high risk during posterolateral corner (PLC) injuries or proximal tibiofibular joint dislocations. The proximal tibiofibular joint itself is stabilized by anterior and posterior superior tibiofibular ligaments, and its dislocation (most commonly anterolateral) disrupts the complex biomechanical linkage between the knee and ankle.
Traumatic hip dislocations and acromioclavicular (AC) joint separations further highlight the importance of capsuloligamentous anatomy. The hip joint's profound intrinsic stability is derived from its deep bony acetabulum, the robust acetabular labrum, and the thickest capsular ligaments in the body (iliofemoral, pubofemoral, and ischiofemoral ligaments). Posterior dislocations, which account for 90% of cases, require massive force to rupture the posterior capsule and short external rotators, frequently injuring the adjacent sciatic nerve and disrupting the medial circumflex femoral artery's terminal branches, which supply the femoral head. Conversely, the AC joint relies on the acromioclavicular ligaments for horizontal stability (preventing anterior-posterior translation) and the robust coracoclavicular (CC) ligaments—the conoid and trapezoid—for vertical stability. The conoid ligament is medial and posterior, inserting on the conoid tubercle, while the trapezoid is lateral and anterior. Anatomic reconstruction of the AC joint must recreate these specific vectors to restore physiologic shoulder kinematics.
Exhaustive Indications and Contraindications
The decision-making process in acute joint dislocations requires a delicate balance between the risks of surgical intervention and the long-term consequences of chronic instability. While many simple dislocations can be managed non-operatively with closed reduction and structured rehabilitation, certain pathoanatomic patterns mandate urgent or elective surgical reconstruction. The following table outlines the definitive indications and contraindications for operative management across various major joints.
| Joint / Pathology | Primary Surgical Indications | Absolute & Relative Contraindications |
|---|---|---|
| DRUJ Instability | Chronic instability with non-reconstructable TFCC; symptomatic volar/dorsal subluxation; failed conservative management. | Advanced DRUJ arthrosis (requires salvage like Darrach); active infection; fixed carpal malalignment. |
| Patellar Dislocation | Intra-articular osteochondral loose body; massive medial disruption with grossly unstable patella in extension; recurrent dislocations; patellar "Bankart" lesion. | First-time dislocation without loose bodies (relative); severe uncorrected lower extremity malalignment (e.g., excessive valgus). |
| Knee Dislocation (MLKI) | Irreducible dislocation (e.g., "dimple sign"); concomitant vascular injury requiring repair; open dislocation; multi-ligamentous instability in an active patient. | Medically unstable polytrauma patient; severe peripheral vascular disease precluding reconstruction; active local infection. |
| Hip Dislocation | Irreducible by closed means; non-concentric reduction; retained intra-articular fragments; associated unstable posterior wall or femoral head (Pipkin) fractures. | Concentric stable reduction without retained fragments; medically unfit for major pelvic surgery. |
| AC Joint Separation | Types IV, V, and VI (severe displacement, skin tenting, muscle penetration); Type III in elite overhead athletes or heavy manual laborers. | Types I and II; Type III in low-demand or elderly patients; active skin infection over the shoulder. |
For the DRUJ, the Liebolt technique is specifically indicated when direct repair of the TFCC is impossible due to tissue attrition or chronicity. It relies on the presence of preserved articular cartilage; if advanced arthrosis is present, ligamentous reconstruction will only result in a stiff, painful joint, necessitating salvage procedures like the Sauvé-Kapandji or Darrach resections. In the patellofemoral joint, the presence of an osteochondral loose body is an absolute indication for acute arthroscopy. The sheer force of the patella relocating over the lateral femoral condyle frequently shears off articular cartilage, which must be excised or fixed to prevent third-body wear and early osteoarthritis.
The management of the dislocated knee is dictated primarily by vascular status. An irreducible posterolateral dislocation, characterized by the classic "dimple sign" (a transverse medial joint line skin furrow caused by the medial femoral condyle buttonholing through the medial capsule), is an absolute indication for emergent open reduction. Once vascularly stable, ligamentous reconstruction is typically delayed for 2 to 3 weeks to allow the capsular tissues to seal and the soft-tissue envelope to recover, thereby significantly reducing the risk of catastrophic postoperative arthrofibrosis.
In traumatic hip dislocations, the immediate goal is closed reduction. However, a post-reduction CT scan is mandatory. Any evidence of a non-concentric reduction, widened joint space, or incarcerated osteochondral fragments dictates urgent surgical intervention via surgical dislocation or arthroscopy to clear the joint and prevent rapid, irreversible chondral damage. For the AC joint, the Rockwood classification guides treatment. While Types I and II are universally managed non-operatively, and Types IV-VI universally require surgery, Type III remains highly controversial. Current evidence-based guidelines suggest a trial of non-operative management for the vast majority of Type III injuries, reserving acute surgical reconstruction for elite overhead athletes whose biomechanical demands exceed the capacity of a conservatively managed shoulder.
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous pre-operative planning is the cornerstone of successful ligamentous reconstruction. The process begins with advanced imaging modalities tailored to the specific joint and suspected pathology. Standard orthogonal radiographs are mandatory but often insufficient for complex reconstructions. For the DRUJ, bilateral CT scans in pronation, neutral, and supination are invaluable for assessing dynamic subluxation and evaluating the osseous architecture for tunnel placement. MRI is the gold standard for evaluating the TFCC and the ECU subsheath. When planning a Liebolt reconstruction, the surgeon must template the distal radius and ulna to ensure that drill tunnels will not violate the radiocarpal articular surface or compromise the structural integrity of the ulnar styloid.
In the setting of acute patellar dislocations, pre-operative MRI is essential to confirm the location of the MPFL tear (femoral vs. patellar) and to evaluate for osteochondral shear injuries. Furthermore, CT imaging is highly recommended to assess the tibial tubercle-trochlear groove (TT-TG) distance and patellar height (Caton-Deschamps index). An abnormal TT-TG distance (>20 mm) or severe patella alta may necessitate concomitant bony procedures, such as a tibial tubercle osteotomy, to normalize the biomechanical vectors before soft-tissue reconstruction. Patient positioning for MPFL reconstruction involves a supine position on a radiolucent table, allowing for unobstructed lateral fluoroscopy, which is critical for identifying Schöttle's point.
The dislocated knee requires the most rigorous pre-operative workup due to its limb-threatening nature. Following initial closed reduction, an Ankle-Brachial Index (ABI) must be measured. An ABI < 0.9 mandates an immediate CT angiogram to rule out popliteal artery injury. Once vascularly cleared, a high-resolution MRI is obtained to map the specific ligamentous injuries. Surgical planning for MLKI often involves staging the procedures or utilizing a multi-surgeon approach to minimize tourniquet time. The patient is positioned supine with a lateral post and a foot positioner to allow for dynamic assessment of the knee during the procedure. A sterile tourniquet is applied, but its use is minimized, particularly if vascular repair was previously performed.
For traumatic hip dislocations, a post-reduction 3D CT scan is the standard of care. This allows the surgeon to map the exact location of intra-articular fragments, assess the size and comminution of posterior wall fractures, and evaluate femoral head impaction (Pipkin) lesions. Depending on the pathology, the patient may be positioned lateral decubitus on a flat radiolucent table for a standard Kocher-Langenbeck approach, or supine on a fracture table if anterior approaches or specific fixation techniques are required. For AC joint reconstructions, patients are typically positioned in the beach-chair position with the operative arm completely free. This positioning allows for anatomic reduction of the clavicle to the coracoid by applying a superiorly directed force on the elbow while simultaneously pushing down on the distal clavicle.
Step-by-Step Surgical Approach and Fixation Technique
The operative execution of joint stabilization requires exacting precision. For chronic DRUJ instability, the Liebolt technique remains a historically significant and biomechanically sound method, utilizing a tendon graft to recreate the volar and dorsal radioulnar ligaments.
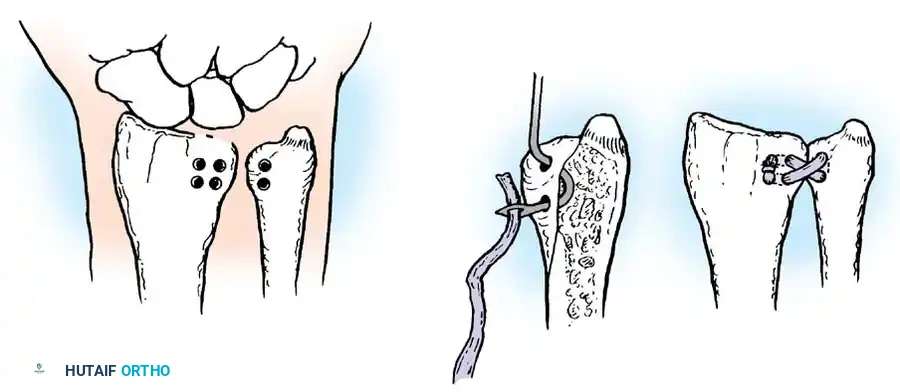
The patient is placed supine with the arm on a hand table. A dorsal longitudinal incision is made over the DRUJ, centered over the fifth extensor compartment. The extensor retinaculum is carefully incised, and the ECU is retracted to expose the distal ulna and radius. Careful fluoroscopic guidance is required to prepare the osseous tunnels, ensuring the radiocarpal joint is not violated. Drill holes are created in the distal radius and the distal ulna to anatomically mimic the origins and insertions of the radioulnar ligaments. A free palmaris longus autograft or a split strip of the ECU tendon is harvested and passed through these tunnels.
Fig. 57-24 Liebolt technique to stabilize distal radioulnar joint. A, Location of holes drilled in radius and ulna. B, Method of passing tendon. C, Appearance after joint has been stabilized.
A critical surgical pearl during this procedure involves the ulnar tunnel preparation. When drilling the ulnar tunnel (Fig. 57-24 A), the surgeon must ensure the entry point is exactly at the fovea—the anatomic isometric point of the DRUJ. Failure to locate the fovea will result in a non-isometric graft, leading to severe restriction of forearm rotation or recurrent laxity. The graft is then tensioned with the forearm in neutral rotation to prevent capturing the joint in fixed supination or pronation. Finally, the graft is sutured to itself or secured with small interference screws (Fig. 57-24 C), and the extensor retinaculum is repaired over the ECU to prevent subluxation.
For acute patellar dislocations requiring MPFL reconstruction, the procedure begins with a diagnostic arthroscopy to address any chondral shear injuries. A gracilis autograft is typically harvested. The femoral attachment is identified using strict fluoroscopic criteria to find Schöttle's point. A guide pin is placed, and a socket is reamed. On the patella, two small transverse tunnels or suture anchors are placed in the proximal two-thirds of the medial border. The graft is fixed to the patella, passed between the capsule and the vastus medialis obliquus (VMO), and docked into the femur. The most critical step is tensioning: the graft must be tensioned at 30 degrees of flexion with only enough force to restore a normal lateral glide (1-2 quadrants). Over-tensioning is a catastrophic error that leads to medial patellofemoral overload and rapid chondrolysis.
In the setting of an irreducible knee dislocation (the "dimple sign"), emergent open reduction is performed via a medial approach. The medial capsule is incised to release the incarcerated medial femoral condyle. Once reduced, definitive ligamentous reconstruction (ACL, PCL, PLC, MCL) is performed, typically utilizing allografts to minimize donor-site morbidity in a severely traumatized limb. Proximal tibiofibular joint dislocations that remain unstable after closed reduction require temporary open reduction and internal fixation (ORIF). A single syndesmotic screw is placed from the fibula to the tibia, taking extreme care to protect the common peroneal nerve.
For AC joint reconstructions, the modern anatomic approach has largely superseded the classic Weaver-Dunn procedure. An incision is made over the distal clavicle and coracoid process. Utilizing heavy non-absorbable sutures or suspensory cortical button devices, the clavicle is anatomically reduced to the coracoid. A free tendon graft (e.g., semitendinosus) is passed under the base of the coracoid and through osseous tunnels drilled in the distal clavicle. The graft is crossed in a figure-of-eight fashion to anatomically recreate both the conoid and trapezoid ligaments, providing robust vertical and horizontal stability.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, the management of acute joint dislocations carries a significant risk of complications, largely due to the severe nature of the initial trauma and the complex biomechanics of the reconstructed joints. The surgeon must be prepared to identify and manage these complications promptly.
| Complication | Associated Joint / Procedure | Estimated Incidence | Salvage Management / Resolution |
|---|---|---|---|
| Avascular Necrosis (AVN) | Traumatic Hip Dislocation | 10-15% (Increases >50% if reduction delayed >6 hrs) | Core decompression (early); Total Hip Arthroplasty (late/collapse). |
| Graft Over-tensioning / Chondrolysis | MPFL Reconstruction (Patella) | 5-10% | Arthroscopic release; revision MPFL reconstruction; patellofemoral arthroplasty. |
| Arthrofibrosis / Severe Stiffness | Knee Dislocation (MLKI) | 15-20% | Aggressive physical therapy; arthroscopic lysis of adhesions; manipulation under anesthesia (MUA). |
| Hardware Failure / Coracoid Fracture | AC Joint Reconstruction | 5-15% | Revision reconstruction with allograft; distal clavicle excision (Mumford) if chronically painful. |
| Loss of Forearm Rotation | DRUJ Reconstruction (Liebolt) | 10-20% | Hardware removal; tenolysis; salvage procedures (Sauvé-Kapandji or Darrach procedure). |
| Sciatic Nerve Palsy | Posterior Hip Dislocation | 10-20% | Observation (spontaneous recovery in 60-70%); Ankle-foot orthosis (AFO) for foot drop; nerve exploration if iatrogenic. |
In DRUJ reconstructions, the most common complication is a severe loss of pronosupination, usually resulting from non-isometric tunnel placement (missing the fovea) or over-tensioning the graft outside of neutral rotation. If aggressive hand therapy fails to restore motion, salvage procedures must be considered. The Darrach procedure (resection of the distal ulna) or the Sauvé-Kapandji procedure (distal radioulnar arthrodesis with proximal pseudoarthrosis) are reliable salvage options that eliminate DRUJ pain while restoring forearm rotation, though they sacrifice normal load-bearing biomechanics.
Following MPFL reconstruction, iatrogenic over-tensioning is the most feared complication. Surgeons must resist the urge to make the patella "tight." An over-tensioned graft pulls the patella forcefully into the medial trochlea, causing severe anterior knee pain, loss of flexion, and rapid, irreversible chondrolysis of the medial patellar facet. Salvage involves urgent surgical release of the graft; however, if advanced arthrosis has already developed, a patellofemoral arthroplasty may be the only viable solution for the older patient.
In the knee, the delicate balance between stability and motion often tips toward arthrofibrosis, particularly if surgery is performed too early (within the first week) during the acute inflammatory phase. If a patient fails to achieve 90 degrees of flexion by 6 weeks post-operatively, manipulation under anesthesia (MUA) and arthroscopic lysis of adhesions are indicated. Conversely, traumatic hip dislocations are a race against time. The incidence of AVN is directly correlated with the duration of the dislocation. If AVN progresses to subchondral collapse, joint-preserving procedures are futile, and the patient will require a Total Hip Arthroplasty (THA), which carries unique challenges in young, post-traumatic patients due to altered bony anatomy and retained hardware.
Phased Post-Operative Rehabilitation Protocols
The success of any ligamentous reconstruction is inextricably linked to a rigorous, phased post-operative rehabilitation protocol. The delicate balance between protecting the healing graft and preventing joint stiffness requires close collaboration between the orthopaedic surgeon and the physical therapy team.
Phase I: Maximum Protection (Weeks 0-6)
During the initial phase, the primary goal is to protect the surgical reconstruction while allowing for early biologic incorporation of the graft. For DRUJ reconstructions (Liebolt), the forearm is strictly immobilized in a long-arm cast or a Munster splint in neutral rotation for 4 to 6 weeks. No active or passive pronosupination is permitted. For MPFL reconstructions, the knee is placed in a hinged knee brace locked in extension for ambulation, but early passive range of motion (ROM) from 0 to 90 degrees is initiated immediately to prevent patellar scarring. In AC joint reconstructions, the shoulder is immobilized in a sling, with pendulum exercises and passive forward elevation limited to 90 degrees to prevent excessive stress on the healing coracoclavicular ligaments.
Phase II: Early Range of Motion and Neuromuscular Control (Weeks 6-12)
As the graft begins to heal, the focus shifts to restoring full, pain-free range of motion and re-establishing neuromuscular control. For the DRUJ, the splint is discontinued, and progressive active and active-assisted ROM exercises for pronation and supination are initiated. For the knee (post-MLKI or MPFL), the brace is unlocked, and patients work toward full flexion. Closed-chain kinetic exercises, such as mini-squats and leg presses, are introduced to stimulate the vastus medialis obliquus (VMO) without placing excessive shear stress on the patellofemoral joint. Proprioceptive training, such as single-leg stance on unstable surfaces, is critical during this phase.
Phase III: Strengthening and Functional Progression (Months 3-6)
Once full ROM is achieved, aggressive strengthening begins. For upper extremity reconstructions (DRUJ, AC joint), progressive resistance exercises targeting the rotator cuff, periscapular stabilizers, and forearm musculature are implemented. Heavy lifting and high-impact activities are strictly prohibited until the 4 to 6-month mark. For the lower extremity, advanced closed-chain exercises, plyometrics, and sport-specific agility drills are introduced. Isokinetic testing may be utilized to ensure limb symmetry before progressing to the final phase.
Phase IV: Return to Sport and Heavy Labor (Months 6-12+)
The final phase is tailored to the patient's specific occupational or athletic demands. Return to play is never dictated by time alone; it requires passing rigorous functional criteria. For MLKI and MPFL patients, this includes >90% limb symmetry on hop testing, full ROM, and no effusions. For overhead athletes recovering from AC joint reconstruction, a gradual throwing program is initiated, focusing on throwing mechanics and core stability. Patients must be counseled that maximal medical improvement following complex joint reconstructions often takes a full 12 to 18 months.
Summary of Landmark Literature and Clinical Guidelines
The contemporary management of acute joint dislocations is deeply rooted in landmark orthopaedic literature. Understanding these foundational studies provides the necessary context for modern surgical decision-making.
In the realm of patellofemoral instability, the work of Sallay et al. (1996) was revolutionary, demonstrating that the MPFL is torn in over 90% of acute lateral patellar dislocations, thereby establishing the MPFL as the primary anatomic target for reconstruction. This was further refined by Schöttle et al., who defined the radiographic landmarks for the femoral origin of the MPFL, ensuring reproducible, isometric graft placement and drastically reducing the rates of iatrogenic graft failure. Furthermore, Nietosvaara et al. (1994) established the absolute indication for acute surgical intervention in the presence of osteochondral loose bodies, highlighting the high incidence of chondral shear injuries during spontaneous relocation.
The management of the dislocated knee was fundamentally altered by Welling et al. (1981), who emphasized the catastrophic consequences of missed popliteal artery injuries. Their work established the mandate for aggressive vascular screening, leading to the modern use of the Ankle-Brachial Index (ABI) and CT angiography protocols. Twaddle et al. (1996) provided critical insights into the timing of MLKI reconstruction, demonstrating that delayed, single-stage reconstruction (at 2 to 3 weeks) yields superior functional outcomes and lower rates of arthrofibrosis compared to acute, immediate repair.
For traumatic hip dislocations, Epstein's classic classifications and outcome studies (1973) remain the gold standard, emphasizing the necessity of concentric reduction and the devastating impact of retained intra-articular fragments. Hougaard and Thomsen (1986) provided the definitive data on avascular necrosis, proving that reduction within 6 hours is the most critical prognostic factor for femoral head survival. Finally, in the management of AC joint injuries, the Rockwood classification (expanded from Bannister et al., 1992) continues to guide treatment algorithms. While the classic Weaver-Dunn procedure was once the standard, biomechanical studies by Copeland & Kessel (1980) and later clinical applications by Dumontier et al. (1995) paved the way for modern, anatomic coracoclavicular ligament reconstructions, utilizing free tendon grafts to restore both the conoid and trapezoid vectors. Adherence to these evidence-based principles ensures the highest standard of care in the operative management of complex joint dislocations.
