Comprehensive Surgical Management of Benign Hand Tumors: Soft Tissue and Osseous Lesions

Key Takeaway
Benign tumors of the hand encompass a diverse spectrum of soft tissue and osseous lesions, including lymphangiomas, schwannomas, glomus tumors, and osteoid osteomas. Accurate diagnosis relies on clinical examination, advanced imaging, and histopathology. Surgical management generally involves meticulous marginal excision or intralesional curettage, prioritizing the preservation of neurovascular structures and hand biomechanics. Recurrence rates vary by tumor histology, necessitating tailored postoperative protocols and realistic patient expectations.
INTRODUCTION TO BENIGN TUMORS OF THE HAND
The evaluation and management of benign tumors of the hand require a profound understanding of upper extremity anatomy, biomechanics, and histopathology. While these lesions lack malignant potential, their presence in the tightly compartmentalized spaces of the hand can lead to significant morbidity, including pain, neurovascular compromise, and functional impairment.
Surgical intervention must be meticulously planned. The primary goals are accurate diagnostic confirmation, complete eradication of the lesion to minimize recurrence, and the absolute preservation of hand function. The use of loupe magnification, microsurgical instruments, and a bloodless field via pneumatic tourniquet are mandatory principles in the operative management of these pathologies.
LYMPHANGIOMA OF THE UPPER EXTREMITY
Pathophysiology and Clinical Presentation
Lymphangiomas are rare, benign soft tissue tumors characterized by an abnormal, hamartomatous proliferation of lymphatic vessels and associated lymphoid tissue. In the upper extremity, they are exceptionally uncommon. These lesions typically manifest during infancy or early childhood and often grow commensurately with the child.
Clinically, lymphangiomas present as soft, compressible, and often painless masses, though they can become acutely painful and swollen secondary to intralesional hemorrhage or localized infection. Because they lack a true anatomical capsule, they tend to infiltrate surrounding subcutaneous tissues, fascial planes, and occasionally muscle, making them notoriously difficult to manage.
Surgical Management and Pitfalls
The management of hand lymphangiomas is fraught with challenges. Their tendency to recur after excision, combined with the pain associated with the condition, makes them especially troublesome for the patient, the parents, and the treating surgeon.
Surgical Warning: Lymphangiomas have no malignant potential. Overly aggressive surgical resection aimed at achieving wide margins must be strictly avoided, as it frequently results in severe hypertrophic scarring, joint contractures, and devastating functional loss.
Parents and surgeons must establish realistic expectations prior to intervention. The goal of surgery is rarely complete eradication; rather, excisional biopsy is recommended for diagnostic confirmation and symptomatic tumor debulking.
Operative Steps for Debulking:
* Positioning: Supine with the arm extended on a radiolucent hand table.
* Incision: Carefully planned Brunner (zigzag) or mid-axial incisions to prevent postoperative scar contractures.
* Dissection: Meticulous separation of the lymphatic malformation from critical neurovascular bundles using tenotomy scissors and bipolar electrocautery.
* Closure: Primary closure without tension. If skin is resected, full-thickness skin grafting may be required.
NEUROFIBROMA AND PERIPHERAL NERVE SHEATH TUMORS
Neurofibromas are benign nerve sheath tumors that can present as solitary lesions or as part of the systemic syndrome Neurofibromatosis Type 1 (NF1). Unlike schwannomas, neurofibromas are intimately intertwined with the nerve fascicles.
FIGURE 77-7 A: Café au lait spot, a hallmark cutaneous manifestation of Neurofibromatosis Type 1.

FIGURE 77-7 B: Multiple palmar neurofibromas demonstrating the diffuse, nodular nature of the disease in the hand.
Because the tumor cells (a mixture of Schwann cells, fibroblasts, and perineurial cells) grow within and expand the nerve itself, surgical excision almost always necessitates the sacrifice of the involved nerve segment. Therefore, asymptomatic solitary neurofibromas are generally observed. Surgery is reserved for lesions causing severe pain, rapid growth, or suspected malignant peripheral nerve sheath tumor (MPNST) transformation.
NEURILEMOMA (SCHWANNOMA)
Histopathology and Diagnosis
Neurilemomas, or schwannomas, arise directly from Schwann cells (the myelin-producing cells of the peripheral nervous system). Despite being the most common solitary tumor of the peripheral nerves, they are relatively rare in the hand.
Proliferation begins around a single nerve fascicle, resulting in an eccentric or centrally located encapsulated tumor that displaces, rather than invades, the remaining normal fascicles. Histologically, schwannomas exhibit a biphasic pattern:
1. Antoni A Areas: Hypercellular regions composed of spindle cells arranged in palisades. The parallel arrays of nuclei are known as Verocay bodies.
2. Antoni B Areas: Hypocellular, myxomatous regions with a loose meshwork of cells and microcysts.
Clinically, these tumors present as slow-growing, mildly tender masses. A classic diagnostic hallmark is that they are mobile at right angles to the course of the nerve, but tethered in line with the nerve. A positive Tinel's sign may be elicited upon percussion. They are frequently misdiagnosed as simple ganglions.
Surgical Enucleation Technique
With careful microsurgical technique, schwannomas can almost always be dissected free from the surrounding nerve, preserving neurological function. Malignant degeneration is exceedingly rare, and marginal excision is curative.

FIGURE 77-10: Gross specimen of a neurilemoma (schwannoma) excised from the terminal branch of a digital nerve, demonstrating its encapsulated, nodular appearance.
Step-by-Step Enucleation:
1. Exposure: Utilize an extensile incision over the course of the nerve. Identify the normal nerve trunk proximally and distally before approaching the tumor mass.
2. Neurolysis: Under loupe or microscopic magnification, perform a longitudinal epineurotomy in a relatively avascular area opposite the main fascicular bundles.
3. Dissection: Gently sweep the normal nerve fascicles off the tumor capsule using micro-freer elevators or fine tenotomy scissors.
4. Excision: Enucleate the tumor intact. If a single, non-functional fascicle is entering and exiting the tumor, it may be sacrificed.
5. Closure: The epineurium does not require formal repair. Close the soft tissues in standard fashion.
Clinical Pearl: If the mass cannot be dissected free from the nerve trunk or appears highly adherent and infiltrative to adjacent tissue, an alternative diagnosis (such as neurofibroma) or malignancy (MPNST) must be strongly considered. In such situations, an incisional biopsy is indicated rather than nerve sacrifice.
GLOMUS TUMORS
Glomus tumors are painful, benign hamartomas arising from the neuromyoarterial glomus body—a specialized thermoregulatory arteriovenous shunt located in the reticular dermis. They most commonly occur in the subungual region of the digits.
Clinical Evaluation
Patients classically present with a triad of symptoms:
1. Severe, paroxysmal pain.
2. Point tenderness (elicited by Love’s pin test, using the head of a pin to localize the exact point of maximum pain).
3. Cold hypersensitivity.
Hildreth's test is highly specific: inflation of a proximal tourniquet relieves the pain, which immediately returns upon tourniquet deflation. Visually, a faint bluish discoloration or nail plate deformity may be observed.
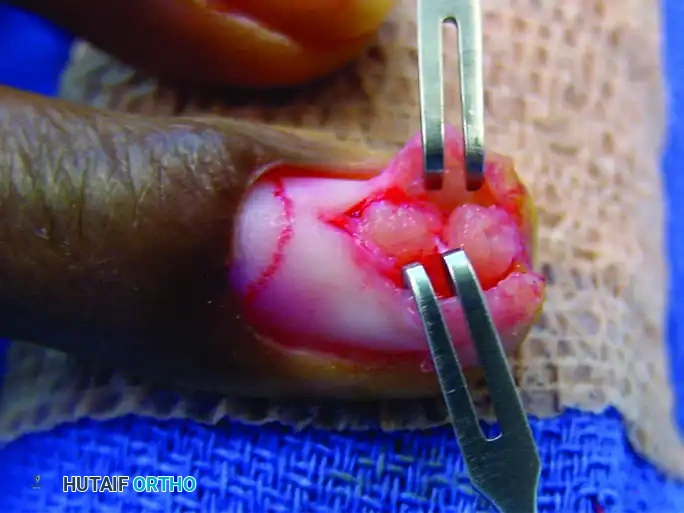
FIGURE 77-8 A: Subungual glomus tumor presenting with characteristic bluish discoloration beneath the nail plate.
Transungual Surgical Excision
Complete surgical excision is curative and provides immediate pain relief. The transungual approach is the gold standard for subungual lesions.
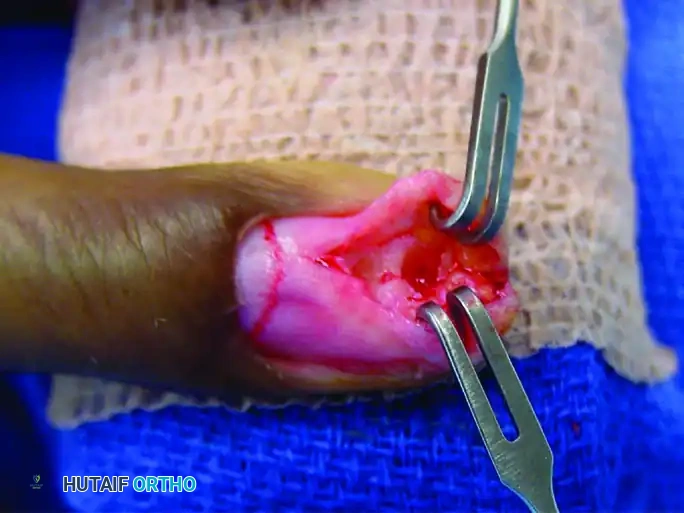
FIGURE 77-8 B: The nail plate is carefully removed, and the nail bed is incised longitudinally to expose the underlying glomus tumor.
Surgical Steps:
1. Nail Plate Avulsion: Elevate and remove the nail plate using a Freer elevator.
2. Nail Bed Incision: Make a strictly longitudinal incision through the sterile matrix directly over the bluish mass. Avoid transverse incisions, which lead to severe nail deformities.
3. Tumor Excision:

FIGURE 77-8 C: The glomus tumor is meticulously excised as a distinct, encapsulated pearl-like mass, with strict preservation of the surrounding nail bed.
4. Nail Bed Repair:

FIGURE 77-8 D: The nail bed is precisely reapproximated and sutured using 6-0 or 7-0 absorbable chromic or plain gut sutures to prevent synechiae and ensure a smooth nail growth trajectory.
5. Stenting: The native nail plate (or a silicone substitute) is replaced under the eponychial fold to stent the matrix open.
OSTEOID OSTEOMA OF THE HAND AND CARPUS
Pathophysiology and Imaging
Osteoid osteomas are benign, bone-forming tumors characterized by a highly vascularized core of osteoid tissue (the nidus) surrounded by a zone of reactive sclerotic bone. The nidus secretes high levels of prostaglandins (specifically PGE2), which mediate the classic clinical presentation: deep, aching pain that gradually increases from mild to severe, is characteristically worse at night, and is dramatically relieved by aspirin or nonsteroidal anti-inflammatory drugs (NSAIDs).
In the upper extremity, more than half of osteoid osteomas occur in the wrist and hand. The lesion occurs twice as often in men as in women, with an average age at diagnosis of 19 years (range 4 to 40 years). Interestingly, some osteoid osteomas of the phalanges present atypically; they may be painless, presumably due to a lack of nerve fibers trapped within the tumor in certain anatomical sub-regions. Generalized swelling of the involved digit and localized tenderness to pressure are frequent findings. The carpus, especially the scaphoid, is a common site of involvement.
Radiographically, the appearance depends heavily on the anatomical zone of bone involved.

FIGURE 77-11: Radiographic appearance of an osteoid osteoma. A small oval or round radiolucent nidus is surrounded by a dense halo of reactive sclerotic bone.
Lesions located in cortical bone or near the cortex may exhibit extreme, dense sclerosis that completely obscures the underlying nidus on standard plain radiographs. In such cases, fine-cut Computed Tomography (CT) is the imaging modality of choice to pinpoint the exact location of the nidus. A triphasic technetium-99m bone scan will also show intense focal uptake and can be helpful in confirming the diagnosis.
Surgical Excision
While radiofrequency ablation (RFA) has become popular for appendicular skeleton lesions, the close proximity of neurovascular structures and extensor tendons in the hand often necessitates open surgical management.
Operative Technique:
* Localization: Intraoperative fluoroscopy or pre-placed CT-guided wire localization is critical to ensure the exact site is approached.
* Cortical Window: A high-speed burr is used to create a precise cortical window directly over the lesion.
* Nidus Excision: The nidus (which appears as a hyperemic, cherry-red, granular tissue) must be completely removed via curettage.
* Validation: Recurrence is highly likely if excision is incomplete. Intraoperative imaging or sending the specimen for immediate frozen section can confirm the presence of the nidus.
* Bone Grafting: Depending on the size of the defect and the structural integrity of the remaining bone, the cavity may be packed with cancellous bone graft.
ENCHONDROMA AND CHONDROMATOUS LESIONS
Enchondromas are benign, intramedullary hyaline cartilage tumors and represent the most common primary bone tumor of the hand. They arise from displaced fragments of the physeal growth plate that fail to undergo normal endochondral ossification.
Clinical Presentation and Pathologic Fracture
Most enchondromas remain asymptomatic until they weaken the cortical bone sufficiently to cause a pathologic fracture following minimal trauma.

FIGURE 77-13: Radiograph demonstrating multiple enchondromas with significant cortical thinning and expansile remodeling of the phalanges, characteristic of Ollier disease.
Radiographically, they appear as well-circumscribed, central radiolucent lesions within the metaphysis or diaphysis of the phalanges or metacarpals. They often exhibit endosteal scalloping and may contain stippled or punctate calcifications (the "rings and arcs" pattern of chondroid matrix).
Surgical Pitfall: When a patient presents with an acute pathologic fracture through an enchondroma, immediate tumor excision is generally contraindicated. The fracture should be immobilized and allowed to heal first. Attempting curettage in the setting of an acute fracture risks severe comminution, loss of bone length, and dissemination of tumor cells into the surrounding soft tissues.
Surgical Curettage and Defect Management
Once the fracture has healed (typically 4 to 6 weeks), definitive tumor management can proceed.
Operative Steps:
1. Approach: A mid-axial or dorsal approach is utilized to expose the lateral aspect of the involved phalanx or metacarpal.
2. Cortical Window: A rectangular window is created in the cortex using a burr or osteotome.
3. Intralesional Curettage: The soft, blue-gray, friable cartilaginous material is thoroughly curetted. High-speed burring of the cavity walls is recommended to extend the margin and remove microscopic rests of cartilage.
4. Adjuvant Treatment: Chemical adjuvants such as phenol, alcohol, or electrocautery may be applied to the cavity walls to reduce recurrence rates.
5. Defect Filling: While some small lesions may heal by secondary intention after curettage alone, filling the cavity is preferred to restore immediate structural integrity. Options include:
* Autologous cancellous bone graft (e.g., from the distal radius).
* Allograft bone chips.
* Calcium phosphate bone cement.
6. Fixation: If the cortical integrity is severely compromised, prophylactic stabilization with Kirschner wires or a miniature plate may be required.
Syndromic Enchondromatosis
While malignant degeneration of an isolated, solitary enchondroma in the hand is exceptionally rare (<1%), the risk increases significantly in patients with multiple enchondromatosis.
* Ollier Disease: Characterized by multiple, asymmetric enchondromas. The risk of sarcomatous degeneration (chondrosarcoma) is approximately 25-30%.
* Maffucci Syndrome: Characterized by multiple enchondromas associated with multiple soft tissue hemangiomas. The risk of malignant transformation is even higher, approaching 100% over the patient's lifetime, necessitating vigilant, long-term clinical and radiographic surveillance. Amputation (ray resection) may ultimately be necessary if massive recurrence, malignant transformation, or complete loss of useful finger function occurs.
===
You Might Also Like


