Isolated Subtalar Arthrodesis: An Intraoperative Masterclass for Hindfoot Fusion
Key Takeaway
This masterclass guides fellows through isolated subtalar arthrodesis, a critical procedure for hindfoot conditions like post-traumatic arthritis. We cover comprehensive anatomy, meticulous preoperative planning, and step-by-step intraoperative execution from incision to hardware placement. Learn crucial pearls for joint preparation, bone graft harvesting, and internal fixation. Master complication avoidance and postoperative care to achieve optimal patient outcomes.
Comprehensive Introduction and Patho-Epidemiology
Welcome, colleagues and fellows, to the operating theater and to this definitive exploration of hindfoot reconstruction. Today, we are undertaking an isolated subtalar arthrodesis, a foundational and highly reliable procedure in the armamentarium of the foot and ankle surgeon. Our primary objective is to achieve a solid, unyielding osseous fusion of the talocalcaneal joint while meticulously preserving the kinematics of the adjacent transverse tarsal articulations. By successfully executing this procedure, we aim to eradicate the patient's chronic, debilitating pain and restore functional, plantigrade stability to the hindfoot.
Historically, the triple arthrodesis was considered the panacea for a multitude of hindfoot pathologies. However, our understanding of foot and ankle biomechanics has evolved significantly over the past few decades. We now recognize that fusing the talonavicular and calcaneocuboid joints unnecessarily sacrifices a tremendous amount of essential midfoot motion, leading to accelerated adjacent segment disease, particularly in the ankle and midfoot articulations. Consequently, the isolated subtalar arthrodesis has emerged as the procedure of choice when the pathologic process is strictly localized to the talocalcaneal joint. This paradigm shift underscores the modern orthopedic principle of joint preservation whenever anatomically and pathologically feasible.
The patho-epidemiology of subtalar joint destruction is diverse, encompassing both insidious degenerative processes and catastrophic traumatic events. Posttraumatic arthritis remains the most prevalent etiology, frequently presenting as a late sequela of intra-articular calcaneal fractures or severe talar neck/body fractures. These high-energy injuries often result in irreversible cartilage damage, joint incongruity, and altered hindfoot morphology, specifically a loss of calcaneal height and an increase in heel width. Beyond trauma, primary osteoarthritis, inflammatory arthropathies such as rheumatoid arthritis, and congenital anomalies like talocalcaneal coalitions represent significant cohorts within our patient population. Understanding the specific etiology is paramount, as it dictates not only the surgical indication but also the nuances of our intraoperative approach, particularly regarding deformity correction and bone graft requirements.
Detailed Surgical Anatomy and Biomechanics
A profound comprehension of subtalar anatomy and biomechanics is the bedrock upon which a successful arthrodesis is built. The subtalar, or talocalcaneal, joint is a complex, multi-faceted articulation anatomically divided into an anterior and a posterior compartment by the robust interosseous talocalcaneal ligament and the cervical ligament, which reside within the sinus tarsi and tarsal canal. The posterior facet is the largest and bears the majority of the axial load; it is convex on the calcaneal side and concave on the talar side. Conversely, the anterior and middle facets, which articulate with the talar head, are smaller and share a common synovial cavity with the talonavicular joint (the talocalcaneonavicular joint complex). Meticulous preparation of the posterior facet is generally sufficient for a robust fusion, though addressing the middle facet can enhance the fusion mass in selected cases.
Vascular anatomy is a critical consideration, particularly given the risk of avascular necrosis (AVN) of the talus or nonunion at the fusion site. The blood supply to the talus is notoriously tenuous, relying heavily on the artery of the tarsal canal (a branch of the posterior tibial artery) and the artery of the sinus tarsi (an anastomotic loop formed by branches of the perforating peroneal and anterior lateral malleolar arteries). Our lateral surgical approach must respect this vascular network. Overzealous dissection within the sinus tarsi or excessive stripping of the talar neck can compromise these vital vessels, precipitating catastrophic ischemic complications. Therefore, soft tissue handling must be deliberate, precise, and respectful of the local angiosomes.
Biomechanically, the subtalar joint acts as a complex torque converter, functioning akin to a mitered hinge, as famously described by Inman. It couples the internal and external rotation of the tibia with the pronation and supination of the foot, respectively. During the stance phase of gait, internal rotation of the tibia translates into subtalar eversion (pronation), unlocking the transverse tarsal joints and allowing the foot to accommodate uneven terrain. Conversely, external tibial rotation drives subtalar inversion (supination), locking the transverse tarsal joints and transforming the foot into a rigid lever for terminal stance and push-off. While an isolated subtalar fusion eliminates this critical inversion/eversion arc, classic cadaveric studies by Ouzounian and Shereff demonstrated that it preserves approximately 26% of talonavicular motion and 56% of calcaneocuboid motion. This residual motion is clinically vital, as it mitigates the rigid, peg-leg gait associated with triple arthrodesis and attenuates the sheer stresses transferred to the ankle mortise.
Exhaustive Indications and Contraindications
Patient selection is the ultimate determinant of surgical success. An isolated subtalar arthrodesis is a powerful intervention, but it must be applied judiciously and only after exhaustive conservative measures have been trialed and failed. The primary indication is intractable pain localized to the subtalar joint, accompanied by radiographic evidence of joint destruction, in a patient whose pathology does not extend significantly into the transverse tarsal joints.
Posttraumatic arthritis following a calcaneal fracture is perhaps the most classic indication. In these cases, we are often tasked not only with fusing the joint but also with restoring the three-dimensional anatomy of the hindfoot. This may require an in situ fusion if alignment is acceptable, or a bone-block distraction arthrodesis to restore calcaneal height, correct lateral impingement, and decompress the subfibular space. Other common indications include primary osteoarthritis, end-stage posterior tibial tendon dysfunction (Adult Acquired Flatfoot Deformity, Stage III), where the hindfoot has become rigidly deformed in valgus, and inflammatory arthritides that have selectively destroyed the talocalcaneal cartilage. Tarsal coalitions, particularly middle facet talocalcaneal coalitions that have become symptomatic and arthritic in adulthood, are also excellently managed with this procedure.
Conversely, we must be acutely aware of absolute and relative contraindications. Active local or systemic infection is an absolute contraindication, necessitating complete eradication prior to any elective arthrodesis. Severe peripheral vascular disease that precludes adequate soft tissue healing is another absolute barrier; a vascular surgery consultation and optimization are mandatory if arterial insufficiency is suspected. Charcot neuroarthropathy is a highly complex relative contraindication; while fusion can be performed to stabilize a disintegrating hindfoot, the nonunion rates are astronomically high, and the procedure requires specialized techniques, extended fixation, and prolonged non-weight-bearing protocols. Finally, uncorrectable rigid deformities in the forefoot or midfoot that would prevent a plantigrade foot post-hindfoot fusion must be addressed concurrently or staged appropriately.
Summary of Indications and Contraindications
| Category | Specific Conditions | Clinical Considerations |
|---|---|---|
| Primary Indications | Posttraumatic arthritis, Primary osteoarthritis | Gold standard for isolated talocalcaneal destruction. |
| Deformity/Instability | Stage III PTTD (Rigid flatfoot), Neuromuscular instability | Corrects rigid valgus/varus deformities; restores hindfoot lever arm. |
| Congenital/Inflammatory | Talocalcaneal coalition, Rheumatoid arthritis | Halts progressive autoimmune destruction; eliminates coalition pain. |
| Absolute Contraindications | Active infection, Severe peripheral arterial disease | High risk of catastrophic failure, osteomyelitis, or amputation. |
| Relative Contraindications | Charcot neuroarthropathy, Active smoking, Poor bone stock | Requires extensive counseling, smoking cessation, and possible orthobiologics. |
Pre-Operative Planning, Templating, and Patient Positioning
The success of a subtalar arthrodesis is largely predicated on meticulous preoperative planning. A comprehensive clinical examination must definitively localize the pain to the subtalar joint. Patients typically present with deep, aching pain in the hindfoot, exacerbated by walking on uneven ground. On physical exam, tenderness is exquisitely localized to the sinus tarsi. Range of motion testing will reveal restricted and painful inversion and eversion compared to the contralateral limb. To confirm the diagnosis and rule out adjacent joint pathology, a fluoroscopically guided diagnostic injection of local anesthetic into the subtalar joint is highly recommended. Complete, albeit temporary, amelioration of symptoms following the injection provides diagnostic certainty and prognostic reassurance for the surgical outcome.
Imaging is critical for templating and strategy formulation. Standard weight-bearing anteroposterior, lateral, and mortise radiographs of the ankle, alongside AP, lateral, and oblique views of the foot, are mandatory.

We specifically evaluate the lateral radiograph for loss of calcaneal pitch, talar declination, and the presence of subchondral sclerosis or cysts. The Broden's view is an excellent adjunct for visualizing the posterior facet in profile. Furthermore, a preoperative Computed Tomography (CT) scan has become the standard of care in my practice. A CT scan provides unparalleled detail regarding the extent of arthritis, the presence of subchondral cysts that may require bone grafting, and the exact three-dimensional morphology of any posttraumatic deformity. It is also indispensable for ruling out an occult tarsal coalition or assessing bone stock for screw purchase.
Patient Positioning and Fluoroscopy Setup
In the operating room, meticulous positioning is the first surgical step. The patient is placed supine on the operating table. A critical maneuver is placing a soft bump beneath the ipsilateral sacrum. This gently internally rotates the entire lower extremity, bringing the lateral aspect of the hindfoot into a direct, orthogonal view for the surgeon. We must ensure the bump is under the sacrum and not compressing the sciatic nerve in the gluteal region to prevent postoperative neuropathies. The foot must be positioned precisely at the end of the bed; this allows unrestricted access for the drill and screwdriver when placing our fixation from the heel to the talus.
A well-padded pneumatic tourniquet is applied to the proximal thigh to ensure a bloodless surgical field, inflated to approximately 100 mmHg above systolic pressure. The fluoroscopy unit (C-arm) is brought in from the contralateral side. Before prepping and draping, we perform a "dry run" with the C-arm to ensure we can effortlessly obtain perfect lateral and axial (Harris) heel views without having to awkwardly manipulate the patient's leg during the critical phases of reduction and fixation.
Step-by-Step Surgical Approach and Fixation Technique
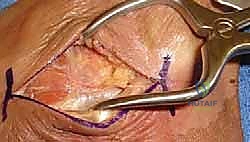
With the patient prepped and draped, we initiate the surgical approach. The classic lateral curvilinear incision remains the workhorse for this procedure. We begin approximately 1 cm distal to the tip of the lateral malleolus and extend the incision anteriorly and distally toward the base of the fourth metatarsal.

This trajectory follows the Langer lines of the skin and provides expansive access to the sinus tarsi and the posterior facet. During the superficial dissection, extreme vigilance is required to identify and retract the sural nerve and its branches, which course superficially in the inferior aspect of the wound. Injury to the sural nerve is a devastating complication that can result in a painful neuroma, often overshadowing a successful osseous fusion.
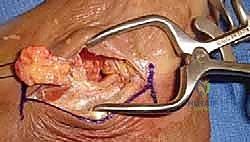
Once the subcutaneous tissues are carefully parted, we encounter the extensor digitorum brevis (EDB) muscle belly occupying the sinus tarsi. We elevate the EDB sharply off its calcaneal origin, reflecting it distally as a thick, protective flap. This exposes the deeper structures of the sinus tarsi, namely the cervical and interosseous talocalcaneal ligaments, and the dense fibrofatty tissue plug known as the Hoke's tonsil.

Using a rongeur and electrocautery, we perform a radical debridement of the sinus tarsi. This aggressive soft tissue clearance is non-negotiable; it is the only way to achieve unobstructed visualization of the anterior, middle, and posterior facets of the subtalar joint.
Joint Preparation: The Art of Denuding Cartilage
The preparation of the articular surfaces is the most critical determinant of a successful arthrodesis. Our objective is to remove all remnants of hyaline cartilage and breach the subchondral bone plate to expose the underlying, vascularized cancellous bone, creating an optimal biological environment for osteogenesis.
We begin on the lateral aspect of the posterior facet. Using a combination of sharp curettes, ring curettes, and small osteotomes, we meticulously peel the cartilage off the talar and calcaneal surfaces. It is imperative to maintain the natural, undulating contours of the posterior facet. Resist the temptation to use a saw to make flat cuts; flat cuts eliminate the inherent bony stability of the joint and make anatomical reduction significantly more challenging.

To access the deep, medial half of the joint, we must distract the articulation. A lamina spreader or a specialized joint distractor is carefully inserted into the lateral aspect of the posterior facet or the sinus tarsi.

As we gently open the joint, the medial cartilage becomes visible. We continue our meticulous debridement medially, ensuring no cartilage islands are left behind, as these will act as barriers to fusion.
Once the cartilage is entirely removed, we address the subchondral bone plate. This dense bone can inhibit vascular ingrowth. We use a high-speed burr, a sharp osteotome, or a drill to perform "fish-scaling" or "feathering" of the subchondral surfaces.

Multiple 2.0mm drill holes are placed across both the talar and calcaneal surfaces to encourage bleeding and the migration of osteoprogenitor cells from the marrow space into the fusion site. If there are large subchondral cysts, they must be aggressively curetted and packed with autogenous bone graft, allograft, or an orthobiologic substitute.

Reduction and Rigid Internal Fixation
With the biological bed prepared, we turn our attention to mechanical stability. The hindfoot must be reduced into an optimal biomechanical position: approximately 5 degrees of valgus, neutral dorsiflexion/plantarflexion, and appropriate medial/lateral translation to align the heel beneath the mechanical axis of the tibia. A hindfoot fused in varus is disastrous, leading to lateral column overload, fifth metatarsal stress fractures, and a rigid, painful gait.

Once the reduction is clinically perfect, we provisionally hold the joint with a stout threaded Steinmann pin or a guide wire for our cannulated screw system.
For definitive fixation, we utilize large-diameter (typically 6.5mm, 7.0mm, or 8.0mm) partially threaded cannulated screws. The classic trajectory is from the non-weight-bearing surface of the posterior calcaneal tuberosity, directed anteriorly, superiorly, and medially into the dense bone of the talar body and neck.

We typically place two screws to provide rotational stability and maximize compression, although a single large, robustly placed screw can be sufficient in certain anatomic constraints.

The first guide wire is driven under fluoroscopic guidance. We check the lateral and axial views to ensure the wire is centered in the talar neck and does not breach the talonavicular joint or the ankle mortise.

After measuring for depth, we overdrill the near cortex and insert the appropriate length screw, ensuring the threads entirely bypass the fusion site to allow for interfragmentary compression.

As the screw head engages the calcaneal cortex (often utilizing a washer to prevent subsidence in osteopenic bone), we observe the joint surfaces compressing tightly together.

A second screw is then placed parallel or slightly divergent to the first to lock the construct rotationally. Final fluoroscopic images in multiple planes confirm absolute joint apposition, correct hardware placement, and optimal hindfoot alignment.

Complications, Incidence Rates, and Salvage Management
Despite meticulous technique, subtalar arthrodesis is not immune to complications. The most dreaded complication is nonunion (pseudarthrosis), which historically occurs in 5% to 15% of cases. Risk factors for nonunion are well-documented and include active tobacco use, diabetes mellitus, prior trauma with avascular necrosis of the talus, and inadequate surgical technique (failure to remove all cartilage or insufficient compression). Patients with asymptomatic nonunions may be observed, but symptomatic pseudarthrosis requires revision surgery. Revision typically involves hardware removal, aggressive takedown of the fibrous nonunion, utilization of structural iliac crest bone graft or potent orthobiologics (such as BMP-2), and enhanced fixation, potentially including a blade plate or a hindfoot intramedullary nail.
Malunion is an entirely iatrogenic complication stemming from poor intraoperative reduction. As emphasized previously, a varus malunion is poorly tolerated, locking the transverse tarsal joints and causing severe lateral foot pain. Valgus malunion is slightly better tolerated but can lead to medial column collapse and impingement against the fibula. Correction of a symptomatic malunion is a formidable undertaking, requiring a corrective closing or opening wedge osteotomy through the solid fusion mass, a procedure fraught with high complication rates.
Nerve injuries, particularly to the sural nerve or the superficial peroneal nerve, occur in approximately 2% to 5% of cases. These are often related to overzealous retraction or direct laceration during the lateral approach. Management begins with conservative modalities, including gabapentinoids and desensitization therapy, but recalcitrant neuromas may require surgical excision and burying of the nerve stump into deep muscle or bone. Hardware prominence at the heel is another frequent complaint, occurring in up to 20% of patients, necessitating a minor outpatient procedure for screw removal once the fusion is radiographically and clinically solid (typically after 6 to 12 months).
Complication Profile and Management Strategies
| Complication | Estimated Incidence | Risk Factors | Prevention & Salvage Strategy |
|---|---|---|---|
| Nonunion | 5% - 15% | Smoking, AVN, Diabetes, Poor bone prep | Prevention: Meticulous joint prep, rigid compression. Salvage: Revision with ICBG/BMP and robust fixation. |
| Malunion (Varus) | 1% - 3% | Inadequate intraoperative fluoroscopic assessment | Prevention: Clinical and radiographic confirmation of 5° valgus. Salvage: Corrective calcaneal osteotomy. |
| Sural Nerve Injury | 2% - 5% | Poor incision placement, excessive retraction | Prevention: Careful subcutaneous dissection, gentle retraction. Salvage: Neuroma excision and implantation. |
| Hardware Prominence | 10% - 20% | Thin heel fat pad, backing out of screws | Prevention: Countersinking screw heads, using washers cautiously. Salvage: Elective hardware removal post-fusion. |
| Adjacent Segment Disease | 15% - 30% (Long-term) | Altered kinematics post-fusion | Prevention: Optimal alignment to minimize stress transfer. Salvage: Orthotics; rarely requires adjacent joint fusion. |
Phased Post-Operative Rehabilitation Protocols
The postoperative rehabilitation phase is as critical as the surgical execution. A premature return to weight-bearing can catastrophically disrupt the delicate osteogenic process, leading to hardware failure and nonunion. Therefore, a strict, phased protocol is mandatory.
Immediately postoperatively, the patient is placed in a bulky, well-padded posterior splint with a U-shaped stirrup to control swelling and immobilize the ankle and hindfoot in a neutral position. The patient is strictly non-weight-bearing (NWB) on the operative extremity. Elevation is paramount during the first two weeks to mitigate edema and promote wound healing. At the two-week mark, the patient returns to the clinic. The splint and sutures are removed. Assuming the incision has healed impeccably, the patient is transitioned into a short-leg fiberglass cast or a rigid, locked controlled ankle motion (CAM) boot.
The NWB status is rigorously maintained for a total of 6 to 8 weeks postoperatively. Around the 6-week mark, we obtain interval radiographs. If there is radiographic evidence of early trabecular bridging and the patient is clinically non-tender at the surgical site, we initiate a progressive weight-bearing protocol. This typically involves partial weight-bearing (25% body weight) in the CAM boot, advancing by 25% each week until full weight-bearing is achieved.
Physical therapy is initiated once weight-bearing begins. The focus is on restoring range of motion to the ankle (tibiotalar joint) and the midfoot, strengthening the gastroc-soleus complex, and intensive proprioceptive retraining. Patients are counseled that maximal medical improvement, including the complete resolution of swelling and the maturation of the fusion mass, may take up to a full year.
Summary of Landmark Literature and Clinical Guidelines
The principles of isolated subtalar arthrodesis are deeply rooted in landmark orthopedic literature. The foundational biomechanical studies by Inman in the 1970s elucidated the complex kinematics of the subtalar joint, conceptualizing it as the critical torque converter of the lower extremity. This understanding highlighted the profound functional consequences of arthrodesis. Subsequent cadaveric investigations by Ouzounian and Shereff in 1989 were pivotal; they quantitatively demonstrated that isolated subtalar fusion preserves significant motion in the talonavicular and calcaneocuboid joints, providing the definitive biomechanical rationale for choosing isolated fusion over triple arthrodesis whenever pathologically appropriate.
Clinically, the work of Easley et al. (2000) remains a cornerstone in understanding the risk factors for nonunion. Their extensive review identified smoking, prior trauma, and the presence of avascular necrosis as the most significant independent predictors of pseudarthrosis, shaping our modern preoperative counseling and patient optimization protocols. Furthermore, long-term outcome studies by Mann and others have consistently validated the durability and high patient satisfaction rates associated with this procedure, provided that anatomical alignment—specifically avoiding varus malposition—is meticulously achieved. These historical and contemporary studies collectively form the evidence-based foundation upon which we practice, ensuring that isolated subtalar arthrodesis remains a highly effective, joint-sparing solution for debilitating hindfoot pathology.
