Operative Management of Elbow Contractures and Medial Epicondylitis
Key Takeaway
Elbow contractures significantly impair upper extremity function. While a normal elbow arc is 0 to 150 degrees, a functional range requires 30 to 130 degrees. Management begins with static progressive splinting, advancing to arthroscopic or open arthrolysis for refractory cases. This guide details the pathophysiology of elbow stiffness, risk factors for heterotopic ossification, and the step-by-step Nirschl surgical technique for medial epicondylitis.
ELBOW CONTRACTURES: PATHOPHYSIOLOGY AND BIOMECHANICS
The elbow is a highly constrained, complex hinge joint uniquely susceptible to post-traumatic and post-surgical stiffness. A normal range of elbow motion is 0 to 150 degrees of flexion, with 75 degrees of pronation and 85 degrees of supination. Due to the high congruency of the ulnohumeral articulation and the robust nature of the collateral ligaments, some loss of motion is associated with all but the most trivial of elbow injuries.
Fortunately, a full, anatomical range of elbow motion is unnecessary for the majority of activities of daily living (ADLs). Extensive biomechanical studies, pioneered by Morrey et al., have established that a functional range of motion consists of an arc from 30 to 130 degrees of flexion, alongside 50 degrees of pronation and 50 degrees of supination.
Clinical Pearl: A flexion contracture that exceeds 45 degrees markedly impairs the patient's ability to position the hand in space, severely limiting activities such as feeding, personal hygiene, and reaching overhead. Extension deficits are generally better tolerated than flexion deficits, provided they remain under 30 to 40 degrees.
Elbow contractures result from a diverse array of etiologies, broadly categorized into intrinsic (intra-articular) and extrinsic (extra-articular) causes. Common culprits include:
* Trauma: Fractures, dislocations, and crush injuries.
* Heterotopic Ossification (HO): Ectopic bone formation in the periarticular soft tissues.
* Burns: Severe thermal injuries leading to cutaneous and capsular contractures.
* Spasticity: Upper motor neuron lesions (e.g., cerebral palsy, stroke).
* Postoperative Scarring: Arthrofibrosis following open reduction and internal fixation (ORIF) or ligamentous reconstruction.
* Prolonged Immobilization: The only entirely preventable cause of elbow stiffness.
Non-Operative Management
The initial management of elbow contractures should almost universally be non-operative. The elbow joint capsule is highly responsive to low-load, prolonged stretch. Many contractures can be managed effectively with a rigorous regimen of physical therapy and dynamic or static progressive splinting.
Ulrich et al. demonstrated the efficacy of a static progressive stretching orthosis utilizing stress relaxation principles. By applying a constant displacement, the viscoelastic properties of the contracted capsular tissues undergo stress relaxation, leading to permanent plastic deformation and tissue elongation. This modality has been shown to result in a mean increase of 26 degrees in the flexion-extension arc. Our primary non-operative goal is to restore a functional range of motion (30 to 130 degrees) without the need for surgical intervention.
HETEROTOPIC OSSIFICATION ABOUT THE ELBOW
Heterotopic ossification (HO) is a devastating complication that can lead to complete bony ankylosis of the elbow. Understanding the risk factors is paramount for implementing prophylactic measures, such as non-steroidal anti-inflammatory drugs (e.g., Indomethacin) or localized radiation therapy.
Risk Factors for Developing Heterotopic Ossification (Box 46-4)
Trauma-Related Factors:
* Open elbow dislocations requiring extensive or multiple surgical debridements.
* Elbow dislocations associated with complex intra-articular fractures requiring ORIF (e.g., terrible triad injuries).
* Radial head fractures treated with surgical intervention delayed greater than 24 hours after the initial injury.
Surgical Factors:
* Distal biceps tendon repair (particularly via a single-incision technique where the radius is exposed to the ulna).
* Repeated surgical procedures utilizing improper or traumatic exposure techniques within the first 2 weeks of injury.
Central Nervous System (CNS) Injury:
* Traumatic brain injury (TBI) or spinal cord injury.
* Concomitant elbow trauma in patients with a severe TBI (carries the highest risk of massive, bridging HO).
Thermal Injuries (Burns):
* Third-degree burns covering over 20% of the total body surface area (TBSA).
* Third-degree burns directly overlying the elbow joint.
* Prolonged periods of bed confinement and immobility in burn units.
Genetic Conditions:
* Fibrodysplasia ossificans progressiva (FOP).
* A known personal history of heterotopic bone formation following previous surgeries.
SURGICAL MANAGEMENT OF ELBOW CONTRACTURES
When non-operative measures plateau after 3 to 6 months, surgical intervention is warranted. The goal of operative arthrolysis is to release contracted extrinsic structures (capsule, ligaments) and address intrinsic pathology (osteophytes, loose bodies, malunited articular segments).
Arthroscopic vs. Open Arthrolysis
We generally approach elbow contractures arthroscopically as a primary procedure, provided the surgeon possesses advanced elbow arthroscopy skills. Arthroscopic release allows for excellent visualization of the radiocapitellar and ulnohumeral joints, enabling precise capsulectomy and osteophyte excision with minimal soft-tissue morbidity.
However, open techniques remain the gold standard for severe contractures, cases with altered neurovascular anatomy (e.g., prior ulnar nerve transposition), or massive heterotopic ossification. We approach open release of elbow contractures using the column method outlined by Morrey, which allows sequential release of the lateral and medial structures while protecting the collateral ligaments.
Surgical Warning: Open elbow arthrolysis yields an average increase in the total arc of motion of 40 to 50 degrees. However, patients must be counseled that achieving a "normal" elbow is rare, and the primary goal is the restoration of functional motion.
The Role of Hinged External Fixation
Hinged external fixation is a powerful adjunct utilized after extensive contracture release. However, because it does not inherently improve the range of motion, carries a high complication rate (pin tract infections, pin loosening, radial nerve injury), and is expensive, its use is strictly delineated.
We reserve hinged external fixation for instances where:
1. Elbow stability is compromised (e.g., the lateral ulnar collateral ligament or medial collateral ligament complex is violated or excised during the release).
2. Joint distraction is required to protect newly resurfaced articular cartilage (e.g., interposition arthroplasty).
CORRECTION OF MEDIAL EPICONDYLITIS (GOLFER'S ELBOW)
Medial epicondylitis is a tendinopathy of the common flexor origin, primarily affecting the pronator teres and the flexor carpi radialis (FCR). Pathologically, it is characterized by angiofibroblastic hyperplasia—a non-inflammatory, degenerative process of the tendon microarchitecture. While most cases resolve with conservative management (rest, bracing, physical therapy, and judicious corticosteroid or PRP injections), refractory cases lasting beyond 6 to 12 months may require surgical intervention.
🔪 Surgical Technique 46-10: The Nirschl Procedure
The Nirschl technique for medial epicondylitis involves the meticulous excision of the pathological angiofibroblastic tissue while preserving the healthy surrounding tendon and the medial collateral ligament (MCL).
1. Patient Positioning and Anesthesia
* The patient is placed supine on the operating table with the operative arm extended on a hand table.
* Regional anesthesia (supraclavicular or axillary block) is preferred, supplemented with general anesthesia if necessary.
* A sterile tourniquet is applied high on the brachium.
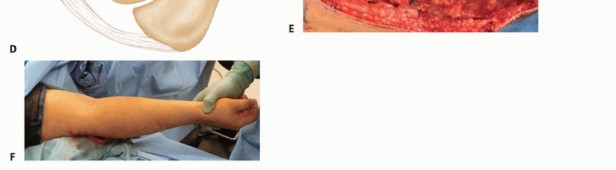
2. Surgical Approach
* Make a slightly curved 5-cm longitudinal incision starting approximately 1 cm proximal and just posterior to the medial epicondyle.
* Anatomical Pitfall: Placement of the incision slightly posteriorly is critical. This trajectory avoids the sensory branches of the medial antebrachial cutaneous (MABC) nerve, which arborize anterior and distal to the epicondyle. Neuroma formation of the MABC is a highly morbid complication that can ruin an otherwise successful surgery.
3. Exposure of the Common Flexor Origin
* Carefully retract the subcutaneous tissue and skin anteriorly over the medial epicondyle to expose the common flexor origin (pronator teres and FCR).
* Maintain strict hemostasis to allow for clear identification of the pathological tissue.
4. Identification and Excision of Pathological Tissue
* Make a longitudinal incision directly in the tendon origins, beginning at the tip of the medial epicondyle and extending distally for 3 to 4 cm.
* Retract the healthy superficial tendon fibers to expose the deeper pathological tissue. This tissue typically appears gray, friable, and edematous, lacking the normal glistening, striated appearance of healthy collagen.
* Excise the pathological tissue elliptically. If the underlying joint capsule is involved or contracted, it may be excised as well.
* Critical Step: Leave the normal tissue of the attachment to the medial epicondyle intact. Do not violate the anterior bundle of the medial collateral ligament (MCL), which lies directly deep to the flexor-pronator mass.
5. Epicondylar Decortication (Optional but Recommended)
* Many surgeons elect to lightly decorticate or drill the footprint of the medial epicondyle using a 2.0-mm drill bit or a rongeur. This stimulates bleeding from the cancellous bone, introducing marrow elements and growth factors to promote a robust healing response.
6. Ulnar Nerve Management
* Evaluate the ulnar nerve. Transpose the ulnar nerve (subcutaneous or submuscular) in patients who exhibit preoperative symptoms of cubital tunnel syndrome, or if pathological anatomy (e.g., subluxation of the nerve over the epicondyle during flexion) is found at the time of surgery.
7. Closure
* Close the elliptical defect in the common flexor origin with heavy absorbable sutures (e.g., #1 or 0 Vicryl) in a side-to-side fashion, ensuring a secure repair without excessive tension.
* Close the subcutaneous tissue with interrupted absorbable sutures.
* Close the skin with a running subcuticular suture to optimize cosmetic outcome.
Postoperative Care and Rehabilitation
Phase I: Immediate Postoperative Period (Weeks 0-1)
* Apply a sterile compressive dressing and a posterior plaster splint with the elbow immobilized in 90 degrees of flexion and neutral forearm rotation.
* The splint is removed 1 week after surgery in the clinic.
Phase II: Early Motion (Weeks 1-3)
* Initiate active and active-assisted elbow range-of-motion (ROM) exercises.
* Avoid passive stretching of the flexor-pronator mass to protect the surgical repair.
* Instruct the patient to avoid heavy lifting or forceful gripping.
Phase III: Strengthening (Weeks 3-12)
* Strengthening exercises are initiated only when a full, painless range of motion is achieved, typically around 3 weeks postoperatively.
* Begin with isometric exercises, progressing to concentric and eccentric strengthening of the wrist flexors and forearm pronators.
Phase IV: Return to Activity (Months 3+)
* Strenuous activity, heavy manual labor, and sports (e.g., golf, throwing) can resume when the patient achieves normal strength without pain, which is typically 3 months after surgery.
* Note on Ulnar Nerve Transposition: A longer period of initial immobilization (up to 2-3 weeks) and a slower, more conservative progression of rehabilitation are indicated in patients who underwent a concomitant ulnar nerve transposition to allow for adequate soft-tissue healing of the fascial slings or muscular flaps.
You Might Also Like