Comprehensive Management of Distal Radioulnar and Ulnocarpal Joint Injuries
Key Takeaway
Distal radioulnar joint (DRUJ) and ulnocarpal joint injuries frequently present as ulnar-sided wrist pain. The triangular fibrocartilage complex (TFCC) is the primary stabilizer. Management depends on Palmer's classification, differentiating traumatic tears from degenerative ulnocarpal abutment. Treatment ranges from conservative immobilization to arthroscopic debridement, TFCC repair, and ulnar shortening osteotomy, aiming to restore biomechanical stability and pain-free forearm rotation.
Anatomy and Biomechanics of the Distal Radioulnar Joint
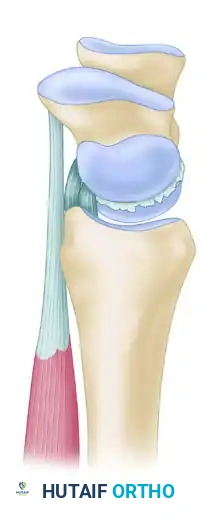
The evaluation and management of ulnar-sided wrist pain—often colloquially referred to as the "low back pain of the wrist"—requires a profound understanding of the complex anatomical and biomechanical relationships of the distal radioulnar joint (DRUJ) and the ulnocarpal articulation. The primary structures responsible for stability and load transfer in this region comprise the ligamentous and cartilaginous network known as the triangular fibrocartilage complex (TFCC), originally detailed by Werner and Palmer.
The Triangular Fibrocartilage Complex (TFCC)
The TFCC is a multifaceted structure that includes:
* Dorsal and Volar Radioulnar Ligaments: The primary stabilizers of the DRUJ.
* Ulnar Collateral Ligament (UCL): Provides medial carpal stability.
* Meniscal Homologue: A fibrous reflection bridging the radius and the ulnar carpus.
* Articular Disc (Triangular Fibrocartilage): The central, avascular cushioning structure.
* Extensor Carpi Ulnaris (ECU) Subsheath: Intimately blended with the dorsal capsule.
The TFCC originates on the ulnar margin of the lunate fossa of the distal radius. It traverses ulnarward to insert onto the fovea at the base of the ulnar styloid and the ulnar head. Distally, it extends to insert onto the triquetrum, hamate, and the base of the fifth metacarpal.
DRUJ Kinematics and Load Distribution
The osseous architecture of the DRUJ offers minimal inherent stability. The shallow sigmoid notch of the radius accounts for only about 20% of DRUJ stability, permitting approximately 1 cm of dorsopalmar translation when the forearm is in a neutral position.
During forearm rotation, the kinematics of the ulnar head within the sigmoid notch are complex. In full pronation, the ulnar head translates dorsally and distally; in full supination, it translates proximally and palmarly. This dynamic translation necessitates robust soft-tissue restraints, primarily the dorsal and palmar radioulnar ligaments.
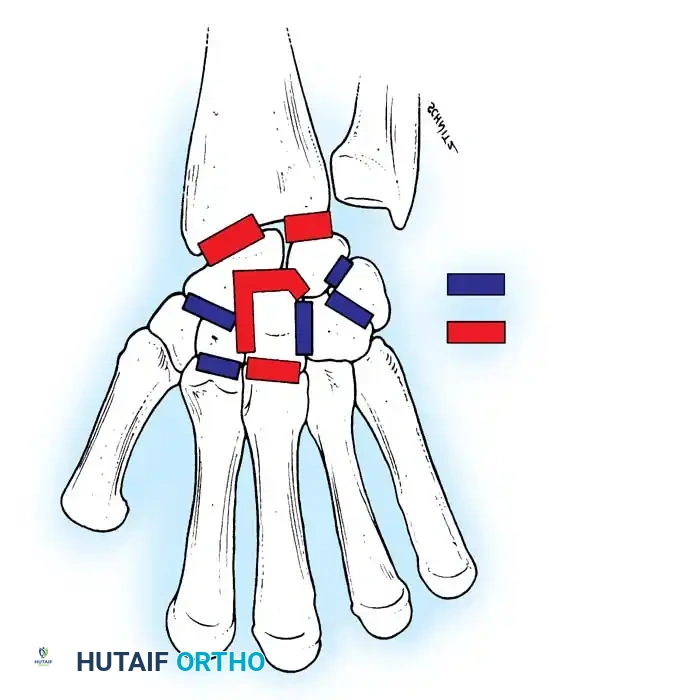
Clinical Pearl: The thickness of the central articular disc is inversely proportional to ulnar variance. In ulnar-positive wrists, the disc is thinner and more susceptible to degenerative perforation, whereas in ulnar-negative wrists, it is thicker and more resilient.
Biomechanical cadaveric studies by Palmer et al. demonstrated that axial loads applied to the wrist are distributed asymmetrically: approximately 80% of the load is transmitted through the distal radius, and 20% is transmitted through the ulna and the TFCC. Alterations in ulnar variance (e.g., following distal radius fractures) drastically shift this load distribution, predisposing the joint to ulnocarpal abutment.
Clinical Evaluation and Diagnostic Imaging
Accurate localization of ulnar-sided wrist pain is paramount. The clinical examination must differentiate between DRUJ instability, TFCC pathology, lunotriquetral ligament tears, and ECU tendinopathy.
Radiographic Assessment
Standardized radiography is critical for assessing ulnar variance and DRUJ congruity.
* Zero-Variance PA View: To accurately assess radioulnar variance, a "neutral position" posteroanterior (PA) radiograph is mandatory. The patient is positioned with the shoulder abducted 90 degrees, the elbow flexed 90 degrees, the wrist in neutral flexion-extension, and the forearm flat on the cassette.
* True Lateral View: Obtained with the arm adducted to the side, elbow flexed 90 degrees, and wrist neutral. This assesses dorsal or volar subluxation of the ulnar head.
Advanced Imaging
- Computed Tomography (CT): The gold standard for evaluating osseous congruity of the DRUJ, particularly in the setting of sigmoid notch fractures or subtle dynamic instability. Axial cuts in pronation, neutral, and supination are highly informative.
- Magnetic Resonance Imaging (MRI): High-resolution MRI (often with intra-articular contrast) is the modality of choice for visualizing the TFCC, lunotriquetral ligaments, and chondral surfaces.
- Arthroscopy: Remains the definitive diagnostic and therapeutic gold standard. It allows direct visualization of central disc perforations, peripheral detachments, and chondromalacia that may evade MRI detection.
Palmer Classification of TFCC Abnormalities
Palmer revolutionized the understanding of TFCC pathology by categorizing lesions into traumatic (Class 1) and degenerative (Class 2) groups.
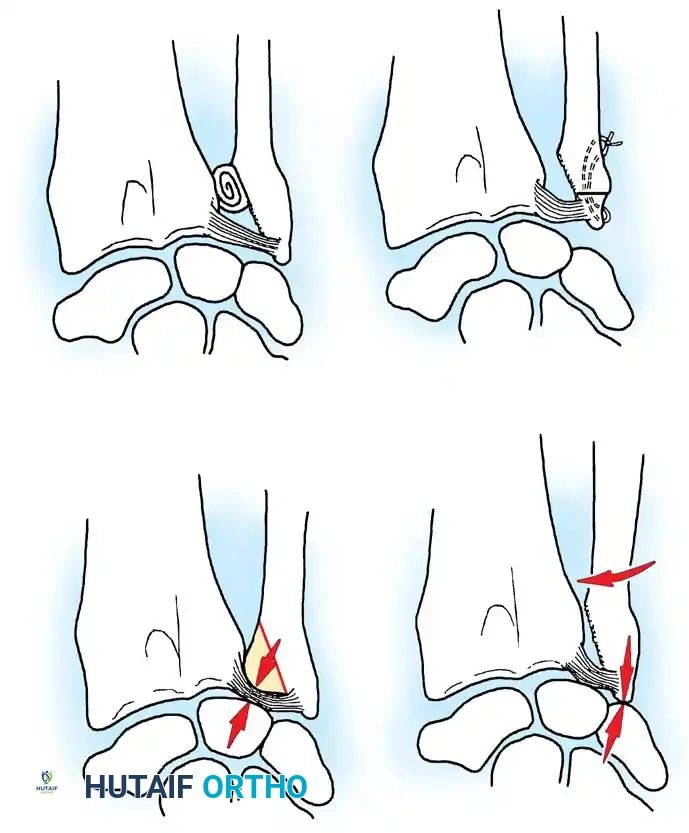
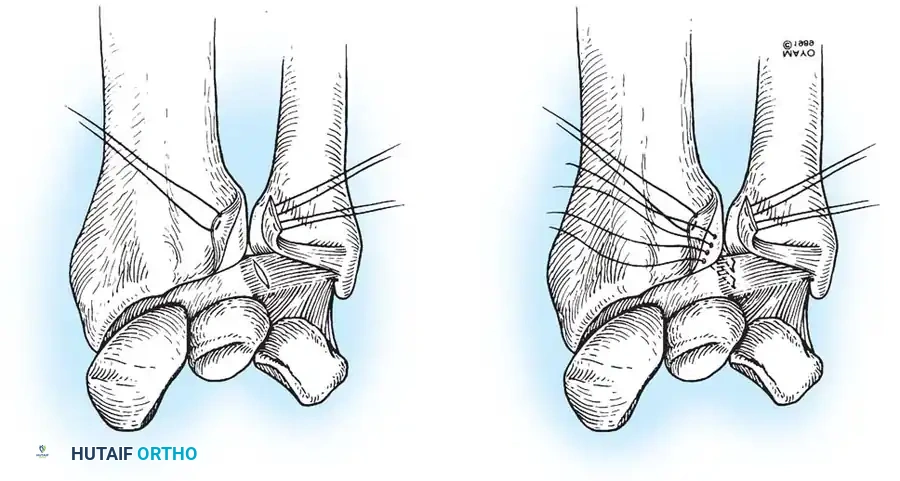
Class 1: Traumatic Lesions
These typically result from forced forearm rotation or axial loading, often associated with distal radius fractures.
* 1A: Central perforation of the articular disc (avascular zone).
* 1B: Ulnar avulsion (with or without ulnar styloid fracture). Involves the highly vascularized periphery.
* 1C: Distal avulsion (involving ulnocarpal ligaments), leading to volar ulnar carpal "sag."
* 1D: Radial avulsion (with or without sigmoid notch fracture).
Illustration of various TFCC tear patterns and their respective biomechanical implications for DRUJ stability.
Class 2: Degenerative Lesions (Ulnocarpal Abutment Syndrome)
These lesions represent a continuum of wear, typically seen in ulnar-positive wrists.
* 2A: TFCC wear (thinning without perforation).
* 2B: TFCC wear + lunate/ulnar chondromalacia.
* 2C: TFCC perforation + lunate/ulnar chondromalacia.
* 2D: TFCC perforation + chondromalacia + lunotriquetral ligament perforation.
* 2E: All of the above + ulnocarpal arthritis.
Management of Traumatic TFCC Lesions (Palmer Class 1)
Non-Operative Management
Initial management for stable Class 1 lesions involves immobilization in a Muenster or long-arm cast for 4 to 6 weeks to control forearm rotation, followed by structured rehabilitation. If symptoms persist, surgical intervention is warranted.
Surgical Technique: Arthroscopic Debridement of TFCC Tears (Class 1A)
Class 1A lesions occur in the avascular central portion of the disc. Because they lack healing potential, the treatment of choice for symptomatic tears is arthroscopic debridement.
Surgical Warning: When debriding a central TFCC tear, never excise more than two-thirds of the central disc. A minimum of 2 mm of the peripheral rim must be preserved to maintain the integrity of the radioulnar ligaments and prevent iatrogenic DRUJ instability.
Step-by-Step Procedure:
1. Setup and Portals: Suspend the wrist with 10 to 15 lbs of traction. Establish the 3-4 portal for the arthroscope and the 6R portal for instrumentation.
2. Diagnostic Tour: Evaluate the radiocarpal joint. Clear synovitis using a 2.0 mm or 2.9 mm full-radius shaver.
3. Assessment: Probe the central TFCC tear. Assess the trampoline effect; a loss of tension indicates a peripheral tear.
4. Debridement: Introduce a punch or shaver through the 6R portal. Carefully resect the unstable flap of the central perforation. Smooth the edges to prevent mechanical catching.
5. Closure: Close portals with non-absorbable sutures and apply a volar splint.
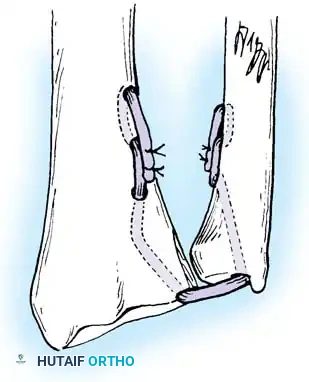
Surgical Technique: Repair of Ulnar Avulsions (Class 1B)
Class 1B lesions involve the vascularized peripheral attachment at the ulnar fovea. These lesions are amenable to repair and are a primary cause of DRUJ instability if left untreated.
Arthroscopic and Open Repair Principles:
If the ulnar styloid is fractured at its base, open reduction and internal fixation (ORIF) of the styloid often restores TFCC tension. If the styloid is intact but the foveal attachment is avulsed, an arthroscopic or open transosseous repair is indicated.
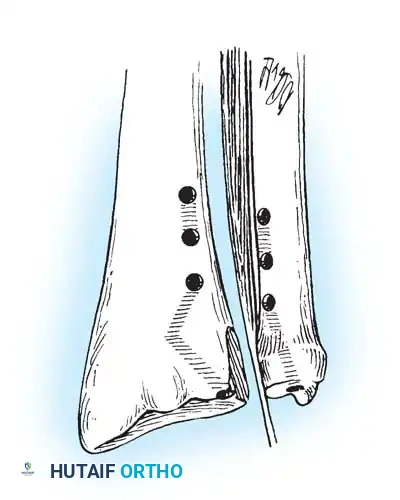
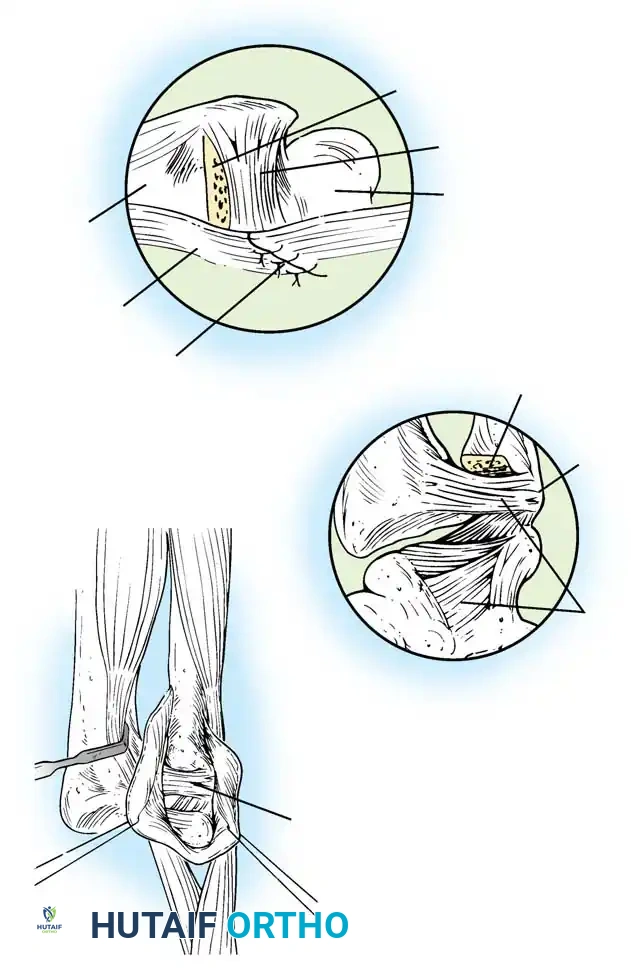
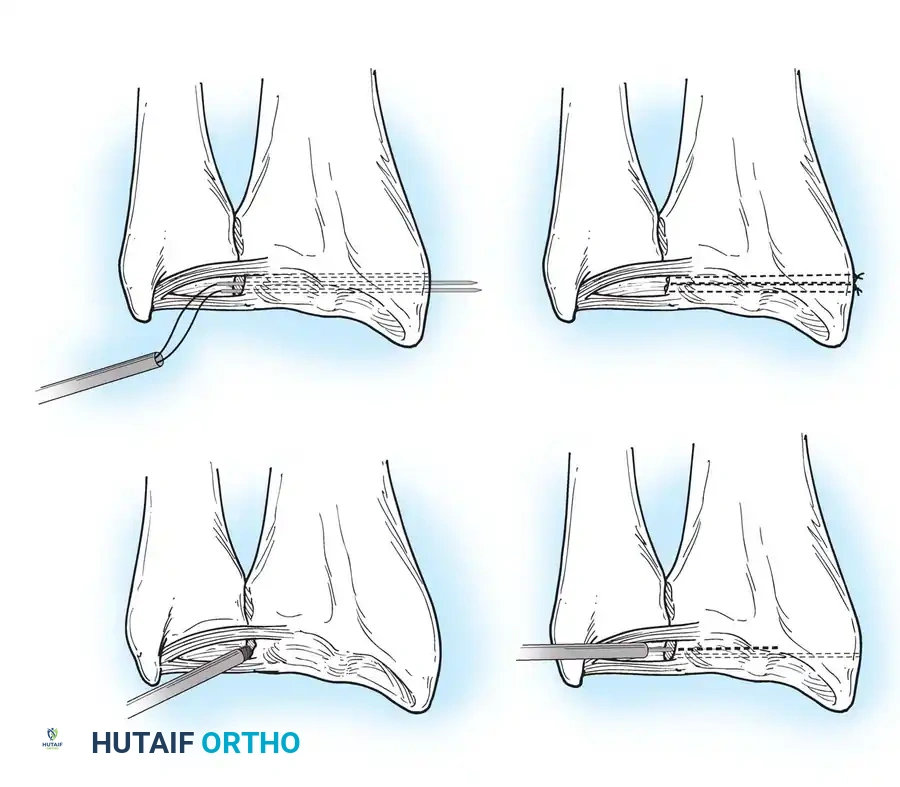
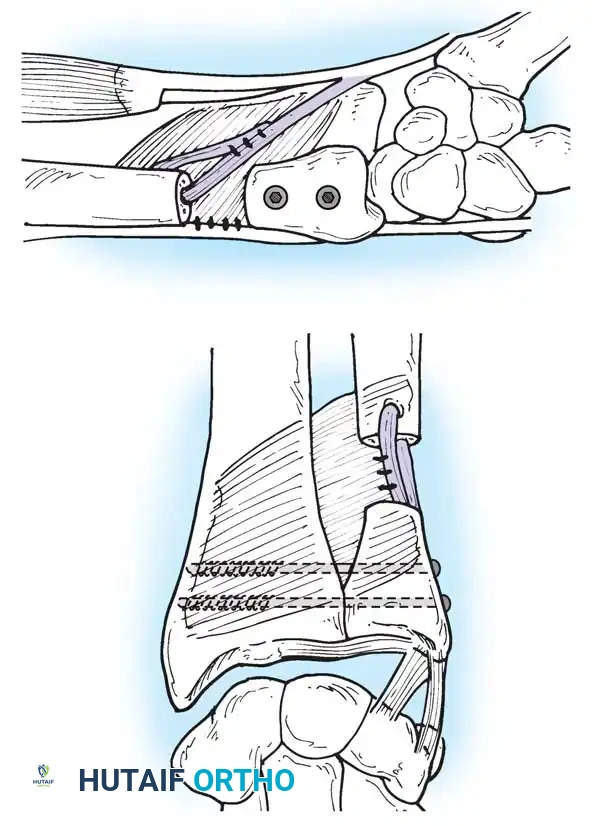
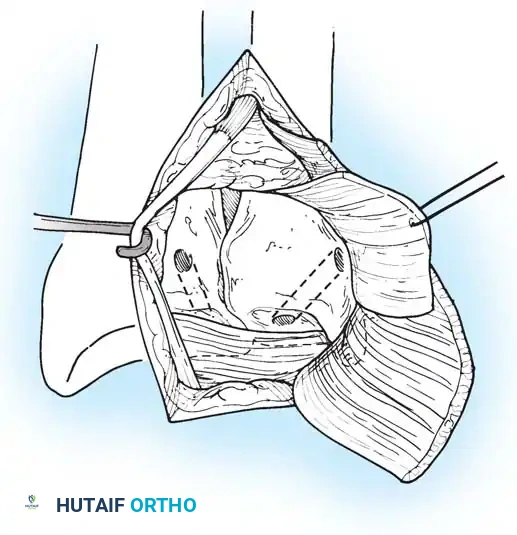
Preparation of the distal ulna: Drill holes are created at the fovea to facilitate transosseous suture passage for anatomic TFCC reattachment.
Transosseous Repair Technique:
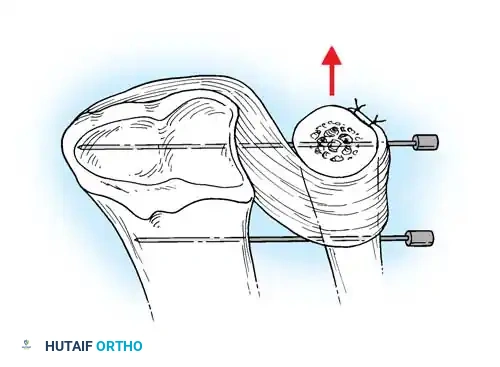
1. Identify the foveal detachment arthroscopically or via an open dorsal ulnar approach.
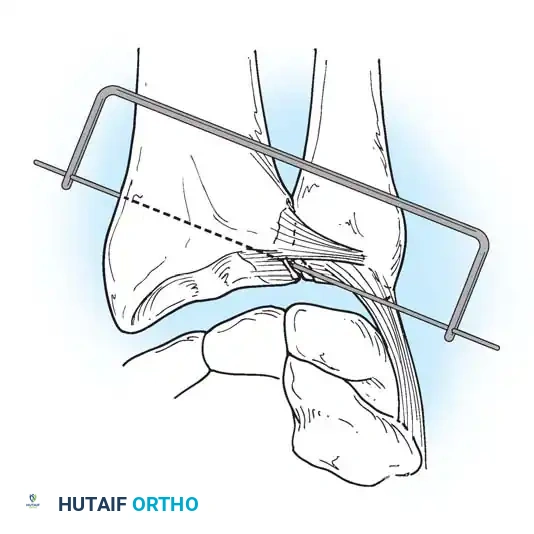
2. Prepare the ulnar fovea down to bleeding bone using a burr or curette to stimulate a healing response.
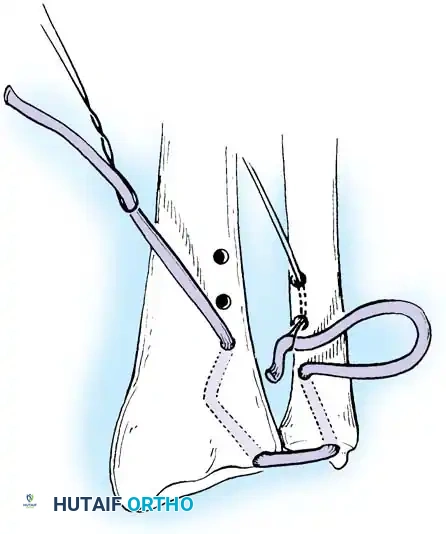
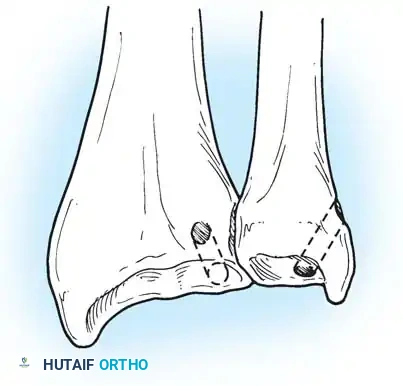
3. Utilize a targeting guide to drill two converging osseous tunnels from the ulnar neck into the fovea.
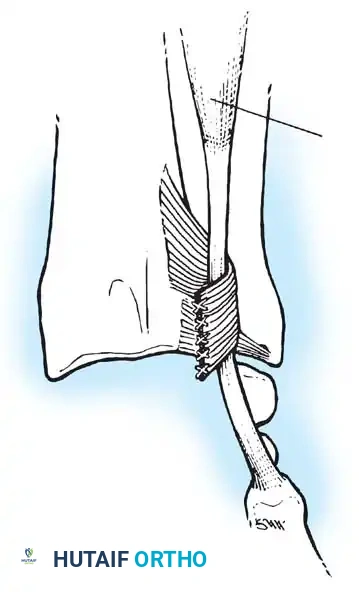
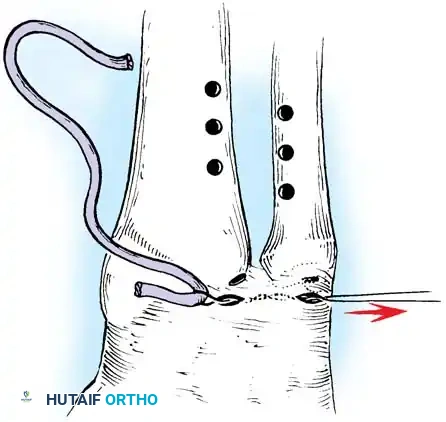
Passing non-absorbable sutures through the osseous tunnels in the ulna to capture the peripheral edge of the TFCC.
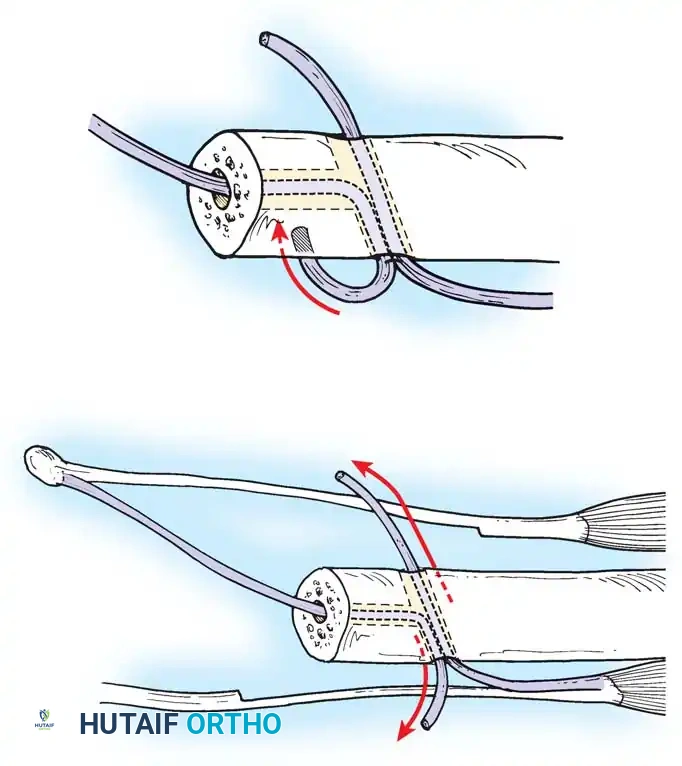
- Pass strong, non-absorbable sutures (e.g., 2-0 FiberWire) through the TFCC using an outside-in or inside-out technique, then shuttle the suture limbs down the osseous tunnels.
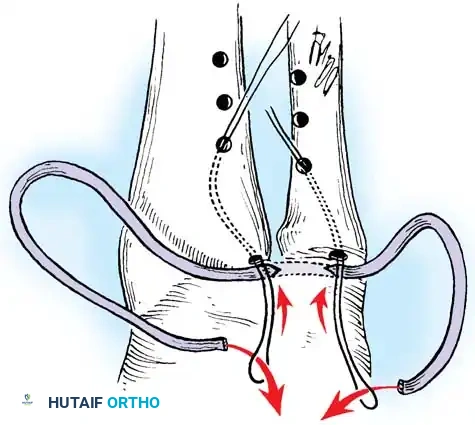
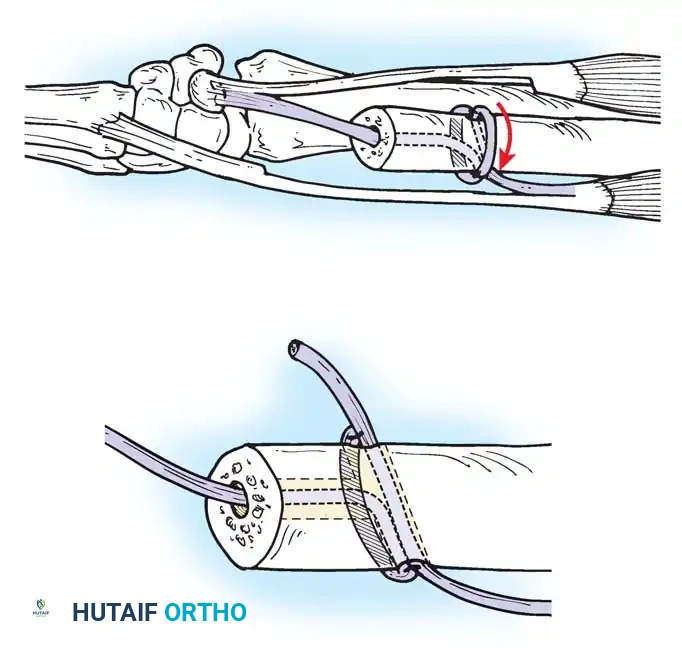
The sutures are tied securely over the cortical bone bridge of the ulnar neck, restoring tension to the radioulnar ligaments.
- Tie the sutures over the ulnar cortical bridge with the forearm in neutral rotation to restore anatomic tension.
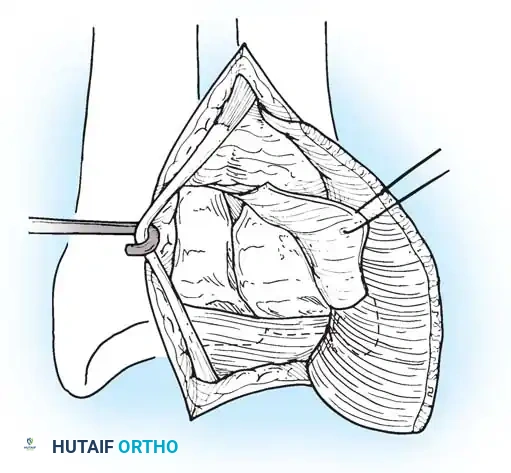
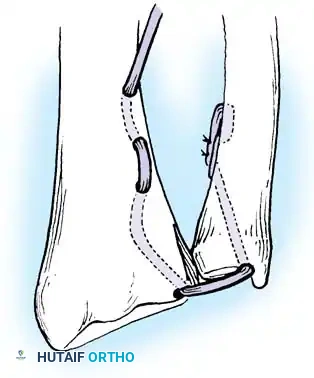
In cases of severe instability or concomitant ECU subsheath disruption, open capsular repair and ECU stabilization are required.
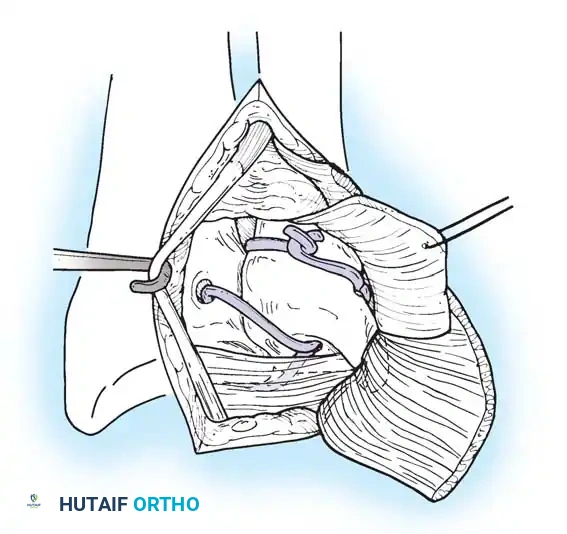
Open repair of the dorsal capsule and TFCC, ensuring robust closure and stabilization of the ulnar-sided structures.
Stabilization of the ECU tendon and subsheath, a critical step in addressing complex ulnar-sided wrist trauma.
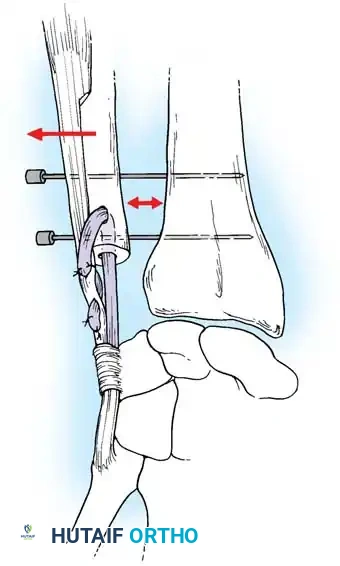
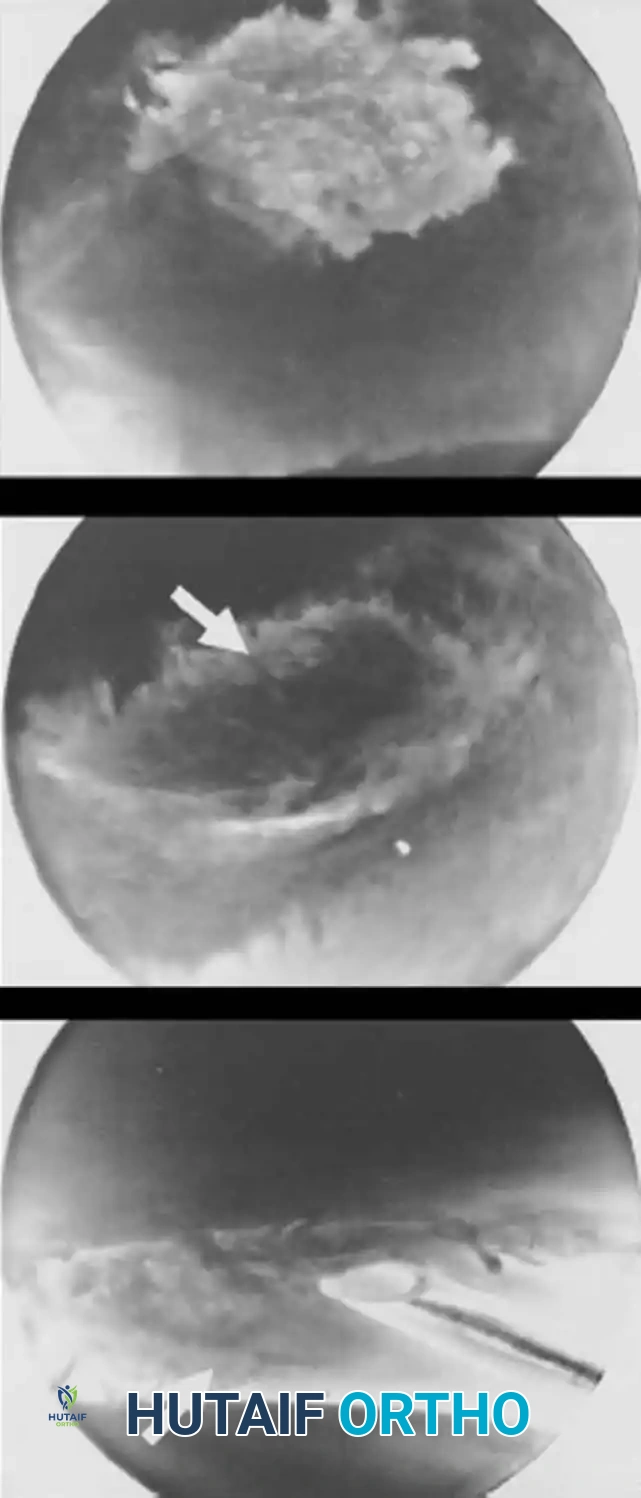
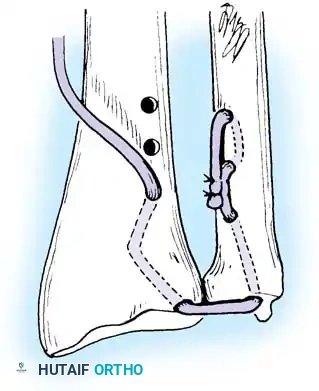
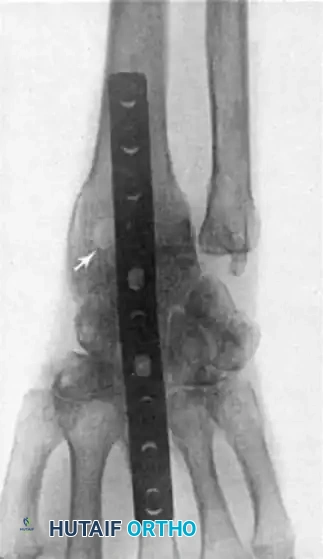
If the DRUJ remains unstable after soft tissue repair, temporary transarticular K-wire fixation may be necessary to protect the repair during the initial healing phase.

Radiographic confirmation of temporary transarticular K-wire fixation stabilizing the DRUJ following complex TFCC repair.
Chronic Instability and TFCC Reconstruction
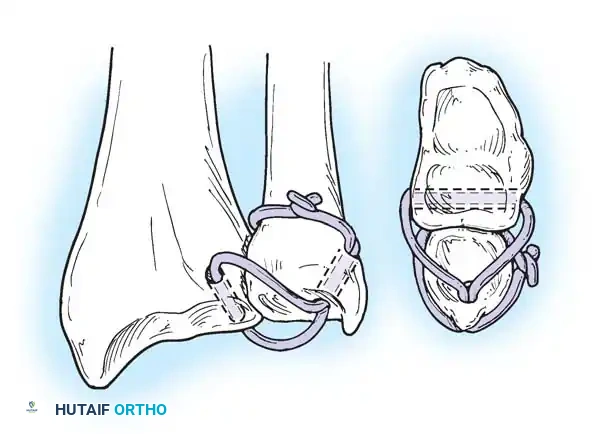
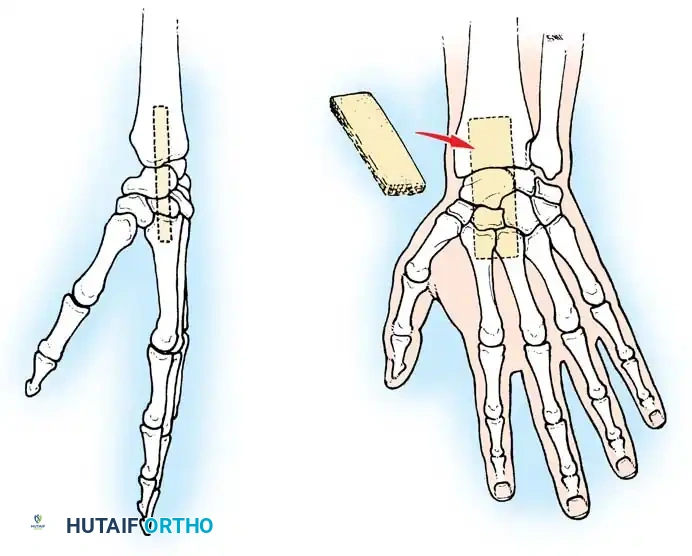
In chronic settings where the TFCC is irreparable, anatomic ligament reconstruction using a tendon autograft (e.g., palmaris longus) is indicated. The graft is routed through the distal radius and ulnar fovea to recreate the dorsal and volar radioulnar ligaments.
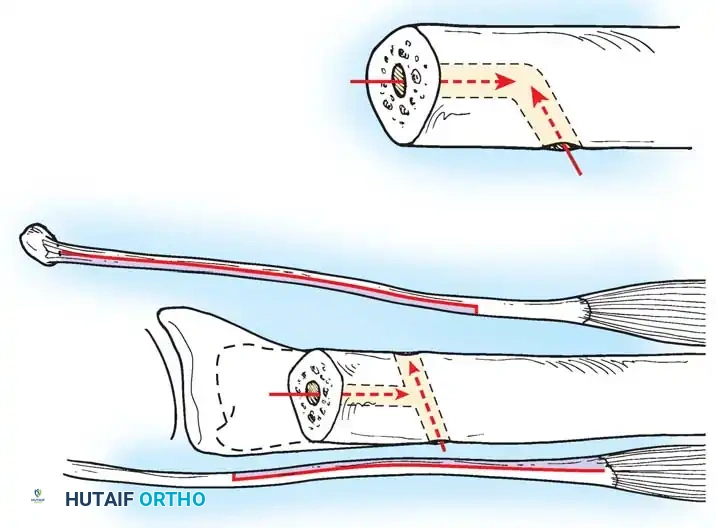
Tendon graft routing through osseous tunnels in the radius and ulna for anatomic reconstruction of the DRUJ ligaments.
Management of Degenerative Lesions (Palmer Class 2) and Ulnocarpal Impaction
Ulnocarpal impaction syndrome is characterized by chronic, load-bearing abutment of the ulnar head against the TFCC and ulnar carpus (lunate and triquetrum). It is predominantly seen in patients with positive ulnar variance, either congenital or acquired (e.g., malunited distal radius fracture, Essex-Lopresti injury).
Symptoms include insidious ulnar-sided wrist pain, exacerbated by forceful grip, pronation, and ulnar deviation. Radiographs typically reveal positive ulnar variance and subchondral sclerosis or cystic changes in the ulnar head and proximal ulnar aspect of the lunate.
Surgical Intervention: Ulnar Shortening Osteotomy
When conservative measures (NSAIDs, splinting, corticosteroid injections) fail, surgical unloading of the ulnocarpal joint is required. Ulnar shortening osteotomy is the gold standard extra-articular procedure. It not only decompresses the ulnocarpal joint but also tightens the ulnocarpal ligaments and the TFCC, thereby stabilizing the DRUJ.
Clinical Pearl: Ulnar shortening osteotomy is contraindicated in the presence of advanced DRUJ arthritis. In such cases, salvage procedures like the Darrach procedure (distal ulnar excision) or the Sauvé-Kapandji procedure (DRUJ arthrodesis with ulnar pseudarthrosis) are indicated.
Surgical Technique for Ulnar Shortening Osteotomy:
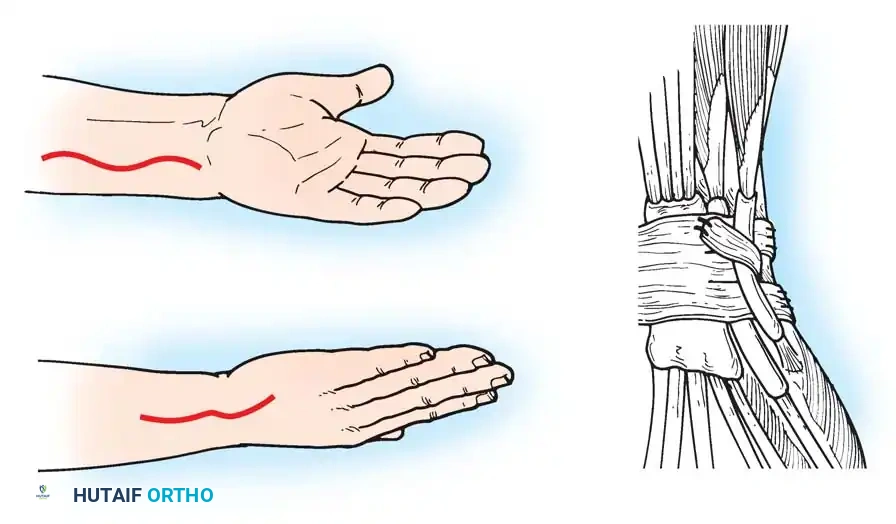
1. Approach: A longitudinal incision is made over the subcutaneous border of the distal ulna. The interval between the ECU and flexor carpi ulnaris (FCU) is utilized.
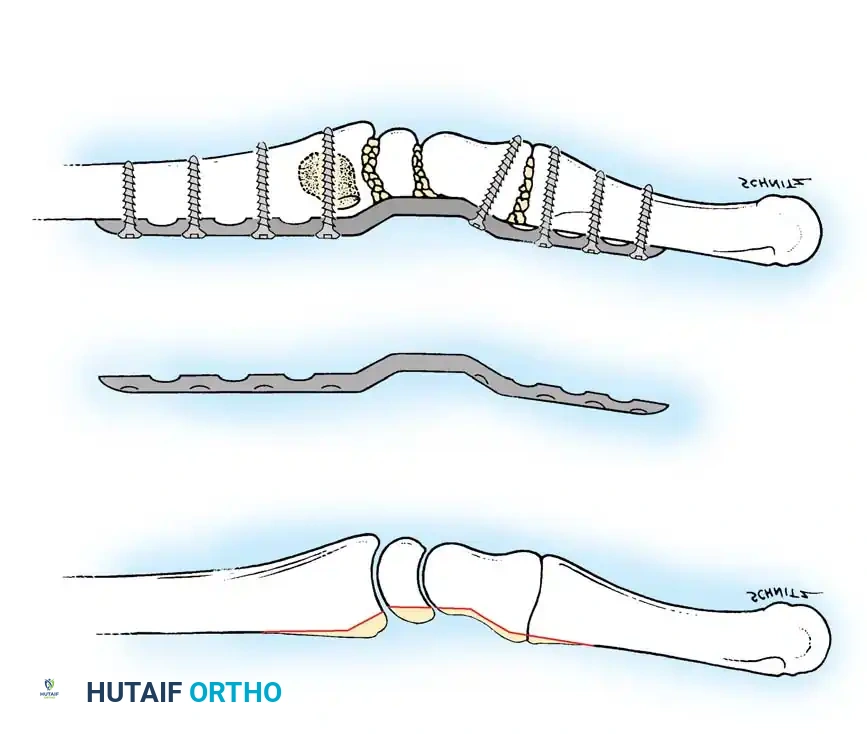
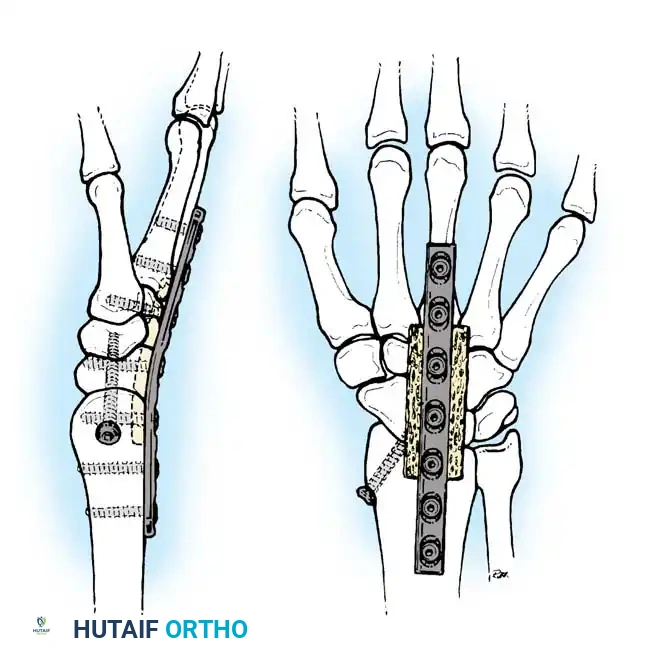
2. Plate Application: A specialized ulnar shortening osteotomy plate is applied to the volar or tension surface of the ulna.
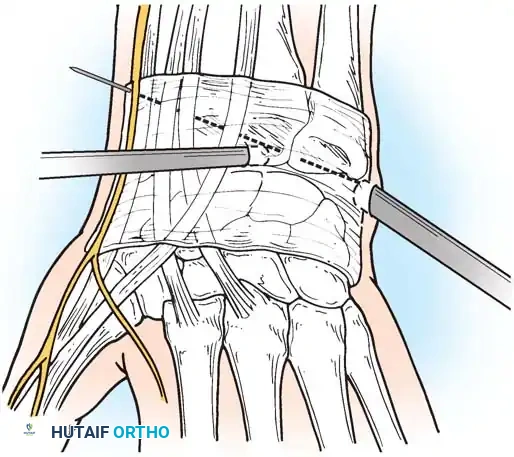
3. Osteotomy: A precise oblique or step-cut osteotomy is performed using a cutting guide. The amount of bone resected (typically 2 to 4 mm) is calculated preoperatively based on the degree of positive variance.
Application of a specialized cutting guide to perform a precise, parallel oblique osteotomy of the ulnar diaphysis.
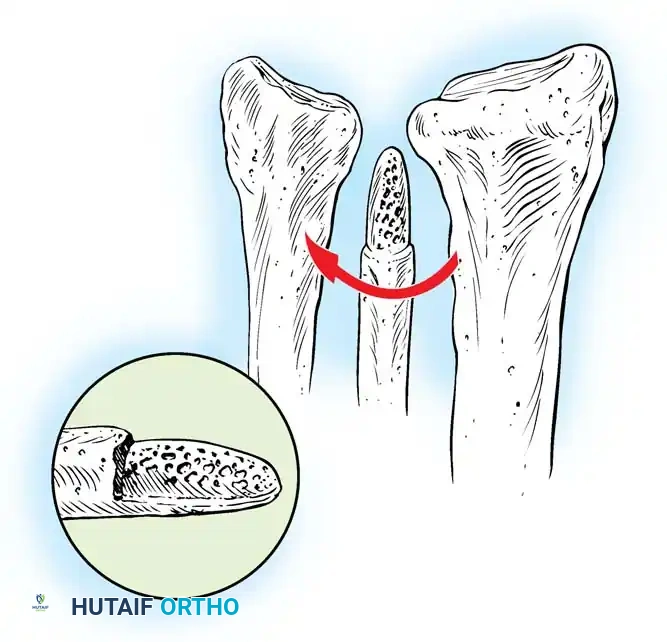
- Compression and Fixation: The osteotomy site is reduced and dynamically compressed using the plate's compression device or an articulated tension device.
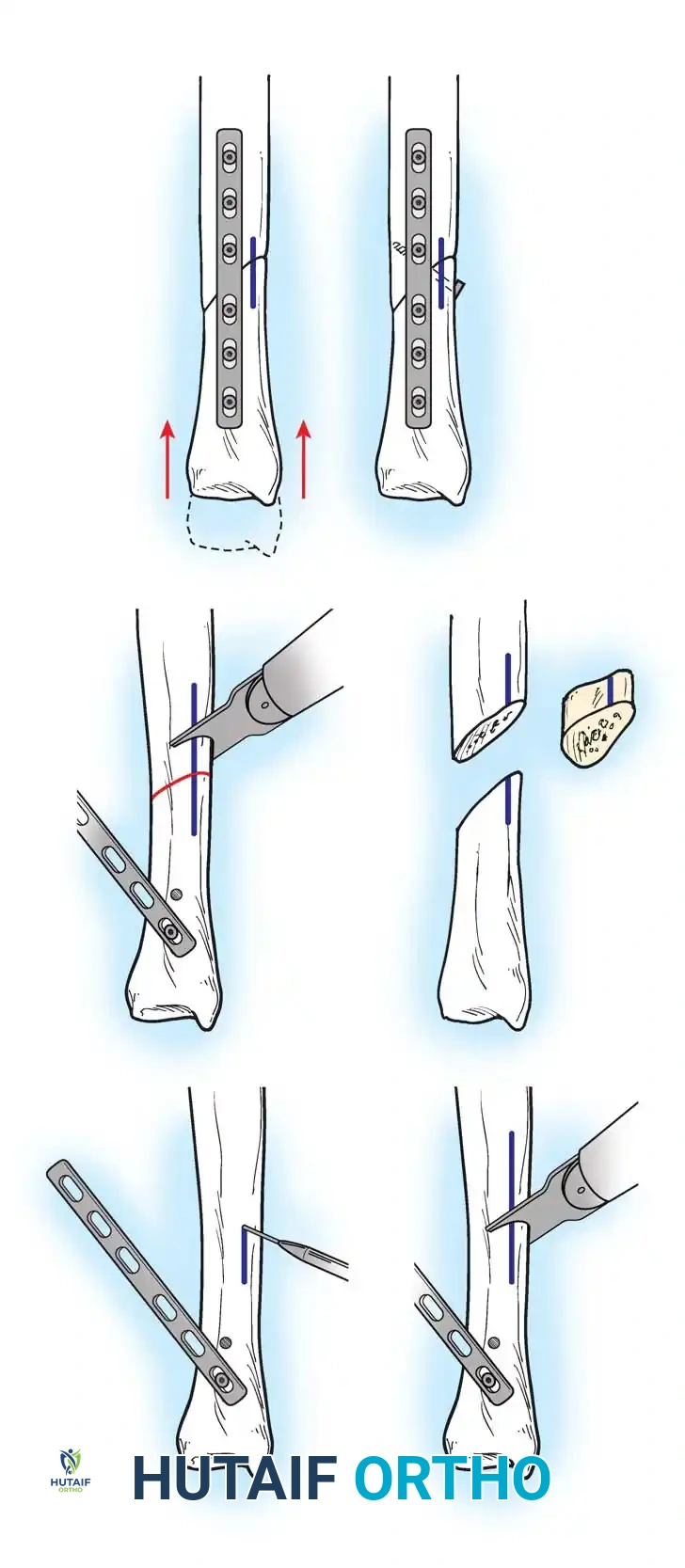
The osteotomy is closed and rigidly compressed using a dynamic compression plate, ensuring primary bone healing and immediate structural stability.
- Closure: The periosteum and soft tissues are meticulously closed over the plate to minimize tendon irritation.
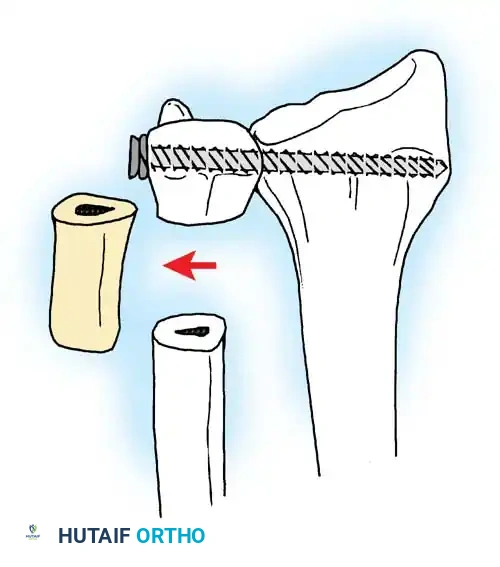
Arthroscopic Wafer Procedure
For patients with mild positive ulnar variance (less than 2 mm) and an intact DRUJ, an arthroscopic wafer procedure (partial resection of the distal ulnar head) is an alternative. This intra-articular procedure removes the central 2 to 3 mm of the ulnar head through the central TFCC perforation, decompressing the joint without the need for an osteotomy or hardware.
Postoperative Rehabilitation Protocols
The success of DRUJ and TFCC surgery relies heavily on strict adherence to postoperative rehabilitation.
- Arthroscopic Debridement (Class 1A) / Wafer Procedure:
- Immobilization in a volar splint for 1 to 2 weeks.
- Early active range of motion (ROM) is initiated.
- Strengthening begins at 4 weeks. Full activity is typically resumed by 6 to 8 weeks.
- TFCC Repair (Class 1B/1C):
- Immobilization in a Muenster or long-arm cast/splint for 4 to 6 weeks to restrict pronation and supination.
- At 6 weeks, transition to a removable wrist splint and begin active-assisted forearm rotation.
- Progressive strengthening begins at 8 to 10 weeks. Return to heavy loading or sports is restricted until 3 to 4 months postoperatively.
- Ulnar Shortening Osteotomy:
- Immediate postoperative splinting.
- Gentle active ROM of the wrist and forearm is initiated within the first 2 weeks, provided rigid fixation was achieved.
- Lifting and forceful rotation are restricted until radiographic evidence of osseous union is observed (typically 8 to 12 weeks). Hardware removal may be considered after 12 to 18 months if the plate causes soft-tissue irritation.
By meticulously evaluating the biomechanical derangements of the DRUJ and applying stage-appropriate surgical interventions—ranging from arthroscopic debridement to complex osseous realignments—the orthopedic surgeon can reliably restore function and alleviate debilitating ulnar-sided wrist pain.
Associated Surgical & Radiographic Imaging



You Might Also Like