Extremity Replantation: Principles, Surgical Techniques, and Functional Outcomes
Key Takeaway
Extremity replantation requires meticulous microvascular expertise and precise patient selection. This guide details the critical steps of replantation, from initial ischemia management and bone shortening to complex neurovascular anastomoses. By adhering to strict biomechanical principles and evidence-based postoperative protocols, orthopedic surgeons can maximize both limb survival and functional recovery, ensuring outcomes that surpass those of amputation and prosthetic fitting.
Comprehensive Introduction and Patho-Epidemiology
The advent of extremity replantation represents one of the most profound advancements in modern orthopedic, plastic, and reconstructive microsurgery. In 1962, Ronald Malt and Charles McKhann at the Massachusetts General Hospital in Boston successfully reattached a completely amputated human limb for the first time, forever altering the landscape of trauma surgery. This monumental achievement was not an isolated event but rather the culmination of excellent experimental and clinical foundations laid by pioneers such as Harry Buncke and Schulz. Concurrently, the persistent clinical innovations of Harold Kleinert and colleagues demonstrated that amputated digits could be replanted with reliable success, challenging the prevailing dogma that such small-caliber vessels were beyond the realm of surgical salvage.
Subsequent landmark reports by Komatsu and Tamai in Japan, and by Ch’en et al. at the Sixth People’s Hospital in Shanghai, provided the earliest accounts of completely amputated digits replanted via direct anastomoses of digital vessels. Since these pioneering efforts, digits, hands, feet, and major limbs have been successfully replanted globally. American centers led by Buncke and Schulz in California, Kleinert et al. in Kentucky, and Urbaniak in North Carolina established the institutional blueprints for replantation centers across the United States. Equally significant were the international contributions from O’Brien in Australia, Ch’en in Shanghai, Biemer in Germany, Meyer in Switzerland, and Millesi in Austria, all of whom refined the microvascular techniques that define the current standard of care.
Atroshi and Rosberg’s extensive review of international epidemiologic data reveals that 85% to 95% of replantations occur in young men, with a mean age of 25 to 30 years. This demographic distribution underscores the occupational and industrial nature of these devastating injuries. Pediatric cases account for 3% to 10% of patients in series that include children, often resulting from home accidents, door crushes, or agricultural machinery. The economic impact of these injuries is staggering, given the loss of productivity in a predominantly young, working-age population, combined with the immense costs of the initial microsurgical intervention, prolonged hospitalization, and extensive outpatient rehabilitation.
The mechanism of injury is a critical determinant of both graft survival and ultimate functional outcome. The primary mechanisms reported in major replantation series dictate the pathophysiological zone of injury. Guillotine or sharp amputations (comprising 14% to 53% of cases) yield the highest survival rates due to highly localized tissue damage and clean vascular transections, allowing for primary end-to-end anastomoses. Crush injuries (11% to 62%) present significant challenges due to broad zones of injury, requiring extensive debridement of devitalized endothelium and often necessitating interpositional vein grafts to bridge the resulting vascular gaps. Avulsion injuries (16% to 29%) carry the poorest prognosis; the intimal damage stretches far beyond the visible level of amputation, leading to a high risk of postoperative thrombosis, the "no-reflow" phenomenon, and severe traction neurapraxia or axonotmesis.

Detailed Surgical Anatomy and Biomechanics
A profound understanding of the microvascular and neural topography of the extremity is the absolute prerequisite for successful replantation. In the upper extremity, arterial inflow dynamics are dictated by the superficial and deep palmar arches, which arborize into the common and proper digital arteries. The proper digital arteries typically measure between 0.8 mm and 1.5 mm in external diameter at the base of the proximal phalanx, tapering distally. Successful microvascular repair hinges on the meticulous handling of the tunica intima and tunica media; even microscopic intimal flaps or subintimal hematomas can act as a nidus for platelet aggregation, initiating a thrombotic cascade that will inevitably doom the replant.
Venous outflow is arguably more critical and technically demanding than arterial inflow. The venous drainage of the digits and hand is highly asymmetric, relying predominantly on the dorsal venous network. These thin-walled, valved structures are highly susceptible to desiccation, mechanical trauma, and torsion. To prevent venous congestion—the most common cause of replant failure—the surgeon must strive to achieve a vein-to-artery anastomosis ratio of at least 2:1, and ideally 3:1. When interpositional vein grafts are harvested (commonly from the volar forearm or dorsal foot), the surgeon must meticulously orient the graft to account for venous valves, ensuring that the valves do not impede antegrade flow when used in the arterial system, or retrograde flow when bridging venous defects.
The neuroanatomy of the extremity dictates the ultimate functional utility of the replanted part. The fascicular topography of the median, ulnar, and radial nerves undergoes complex spatial rotations as the nerves course distally. In the context of replantation, primary epineurial or group fascicular repair must be executed with zero tension. Tension across the neurorrhaphy site induces intraneural ischemia, exacerbating Wallerian degeneration and severely compromising axonal sprouting. If the zone of injury precludes tension-free coaptation after adequate bone shortening, the use of autologous nerve grafts (such as the medial antebrachial cutaneous nerve or the sural nerve) is unequivocally indicated to bridge the defect.
From a biomechanical standpoint, the management of the skeletal framework is the foundation upon which all subsequent soft tissue repairs rest. Bone shortening is not merely an option; it is a biomechanical imperative. Attempting to maintain the original bone length in the face of a crush or avulsion injury will invariably place excessive tension on the microvascular anastomoses and nerve repairs. The osseous structures must be shortened until healthy, uninjured intimal tissue can be coapted without tension. Furthermore, the chosen method of osteosynthesis (whether longitudinal K-wires, crossed K-wires, 90-90 intraosseous wiring, or mini-fragment plates) must provide sufficient absolute or relative stability to withstand the deforming forces of the flexor and extensor tendons, thereby permitting early protective mobilization protocols without risking fixation failure.

Exhaustive Indications and Contraindications
The fundamental philosophical prerequisite for extremity replantation is that the anticipated functional outcome must surpass that of a well-fitted prosthesis or a revised amputation stump. The surgeon must carefully weigh the potential for useful motion, protective sensibility, and cosmetic acceptability against the immense surgical risk, the psychological toll of prolonged rehabilitation, and the substantial economic burden placed upon the patient and the healthcare system. Replantation is a limb-salvage procedure, but it must never devolve into the salvage of a useless, painful, or insensate appendage that ultimately hinders the patient's overall function.
Ischemia time is a paramount physiological variable guiding patient selection. Muscle tissue, due to its high metabolic demand, undergoes irreversible necrosis and subsequent fibrosis after approximately 6 hours of warm ischemia. Replantation of macro-amputations (proximal to the radiocarpal joint) after this window invites devastating systemic complications, including ischemia-reperfusion injury, myoglobinuria, and acute renal failure. Conversely, amputated digits—which lack a muscular belly and consist primarily of bone, tendon, and skin—exhibit remarkable tolerance to ischemia. Digits can routinely tolerate up to 12 hours of warm ischemia and, if properly cooled to 4°C, up to 24 hours of cold ischemia without compromising survival.
Age-specific indications require nuanced clinical judgment. There are no absolute upper or lower chronological age limits for replantation; physiological age and baseline functional status are the true determinants. Pediatric patients possess extraordinary neuroplasticity and regenerative capacity, making replantation highly indicated even in severe injuries. Conversely, geriatric patients often exhibit poor nerve regeneration, baseline joint arthropathy, and a higher propensity for profound postoperative joint stiffness. However, replantation above the elbow in an elderly patient may still be indicated strictly to preserve joint length in anticipation of a subsequent below-elbow amputation, thereby allowing for a vastly superior prosthetic fitting.
The thumb, contributing to approximately 40% to 50% of overall hand function, represents a mandatory indication for replantation whenever technically feasible, regardless of the level or mechanism of injury. Multiple digit amputations, amputations in children, and single digit amputations distal to the flexor digitorum superficialis (FDS) insertion (Zone I) are also strong indications. Conversely, absolute contraindications include concomitant life-threatening injuries (the "life over limb" principle), severe multilevel segmental crush injuries, and extreme physiological instability.
| Parameter | Strong Indications for Replantation | Relative/Absolute Contraindications |
|---|---|---|
| Patient Factors | Pediatric age, highly motivated adult | Hemodynamic instability, severe comorbidities, severe psychiatric illness |
| Amputation Level | Thumb, multiple digits, partial hand, wrist level | Single digit proximal to FDS insertion (Zone II) in adults (relative) |
| Mechanism | Sharp/Guillotine amputation | Severe multilevel crush, extreme avulsion with diffuse intimal damage |
| Ischemia Time | Digits: <12h warm, <24h cold | Proximal limb: >6h warm ischemia |
| Systemic Injury | Isolated extremity trauma | Concomitant life-threatening head, chest, or abdominal trauma |

Pre-Operative Planning, Templating, and Patient Positioning
The pre-operative phase of extremity replantation begins at the point of injury and extends through the trauma bay into the microsurgical suite. Proper handling of the amputated part is critical to preserving cellular viability. The amputated segment must be wrapped in saline-moistened sterile gauze, placed inside a sealed, watertight plastic bag, and then immersed in a slurry of ice and water (ice slush). Direct contact with ice or the use of dry ice is strictly contraindicated, as it induces irreversible cellular frostbite and microvascular thrombosis. Concurrently, the patient must be evaluated utilizing standard Advanced Trauma Life Support (ATLS) protocols to rule out life-threatening injuries that would preclude prolonged microsurgical intervention.
Radiographic evaluation is mandatory for both the amputation stump and the amputated part. High-quality orthogonal radiographs allow the surgeon to template the required bone shortening, identify occult fractures within the amputated segment, and select the appropriate hardware for osteosynthesis. In cases of proximal extremity amputations or severe crush injuries, pre-operative angiography may occasionally be indicated to delineate the proximal vascular tree, though it should never significantly delay the transfer to the operating room. The surgical plan must explicitly detail the sequence of repair, the anticipated need for vein or nerve grafts, and the strategy for soft tissue coverage.
The operating room setup for replantation demands a highly specialized infrastructure. A two-team approach is vastly superior to a single-surgeon effort. Team A assumes responsibility for the meticulous preparation, debridement, and tagging of neurovascular structures on the amputated part at a back table, utilizing loupe magnification and the operating microscope. Team B simultaneously prepares the amputation stump on the patient. This concurrent workflow dramatically reduces total ischemia time and mitigates surgeon fatigue during procedures that routinely exceed 10 to 12 hours. The room must be equipped with a high-resolution, dual-head operating microscope, specialized micro-instruments (jeweler's forceps, adventitial scissors, micro-vessel clamps), and a temperature-controlled environment to prevent patient hypothermia and subsequent peripheral vasospasm.
Patient positioning and anesthesia are optimized for prolonged microvascular surgery. The patient is placed supine with the affected extremity extended on a radiolucent hand table. Regional anesthesia, specifically an axillary or supraclavicular brachial plexus block utilizing a continuous indwelling catheter, is the anesthetic modality of choice. This not only provides excellent intraoperative and postoperative analgesia but also induces a profound sympathectomy, resulting in sustained peripheral vasodilation that maximizes flow across the microvascular anastomoses. A Foley catheter is placed to monitor urine output (especially critical for detecting myoglobinuria in proximal amputations), and forced-air warming blankets are applied to maintain core body temperature above 37°C.
Step-by-Step Surgical Approach and Fixation Technique
The sequence of replantation generally follows a highly standardized progression, although minor variations exist based on the level of amputation and surgeon preference. The classic sequence is: Preparation and Debridement, Bone Fixation, Extensor Tendon Repair, Arterial Anastomosis, Nerve Repair, Flexor Tendon Repair, Venous Anastomosis, and Skin Closure. Some surgeons prefer to repair the flexor tendons before the neurovascular structures to minimize manipulation of the anastomoses, while others prioritize immediate arterial repair in cases of prolonged ischemia.
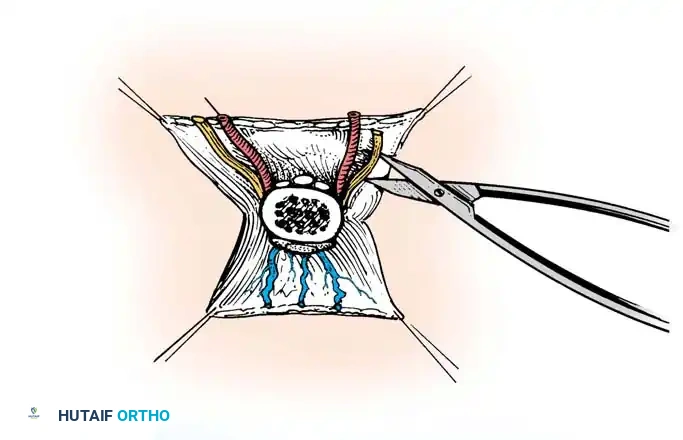
Meticulous debridement under tourniquet control is the most critical initial step. The zone of injury is often deceivingly broad. All devitalized tissue, including contaminated bone, crushed muscle, and avulsed skin, must be radically excised until punctate bleeding is observed from the soft tissues and Haversian canals of the bone. The neurovascular bundles are systematically identified, dissected free from surrounding scar tissue, and tagged with high-visibility sutures under loupe or microscopic magnification. The adventitia of the vessels is stripped back 2 to 3 millimeters to expose the tunica media, preparing the vessels for eventual anastomosis.
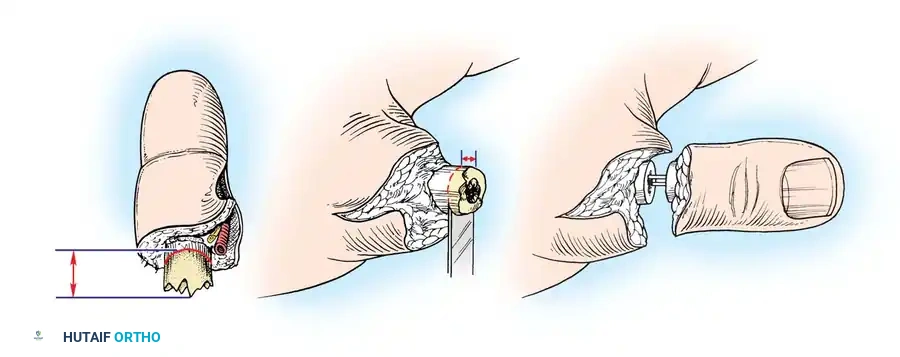
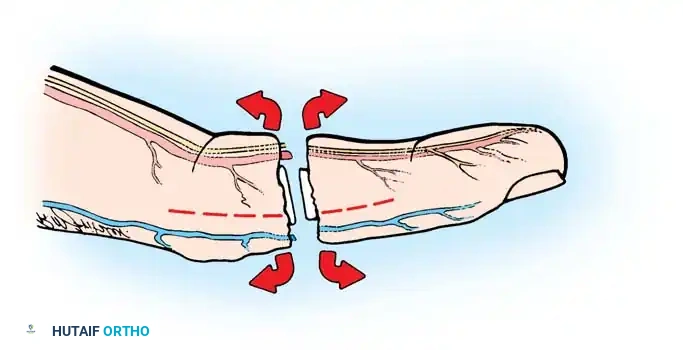
Bone shortening is mandatory and must be executed with precision. Attempting to maintain original bone length will result in excessive tension on the microvascular anastomoses and nerve repairs, leading to inevitable failure. The bone is shortened using an oscillating saw, ensuring perpendicular cuts to maximize cortical contact. The degree of shortening is dictated by the extent of the vascular and neural gaps; the bone must be shortened until healthy, uninjured intima can be coapted without tension. Inadequate bone shortening is a primary, yet entirely preventable, cause of vascular thrombosis.
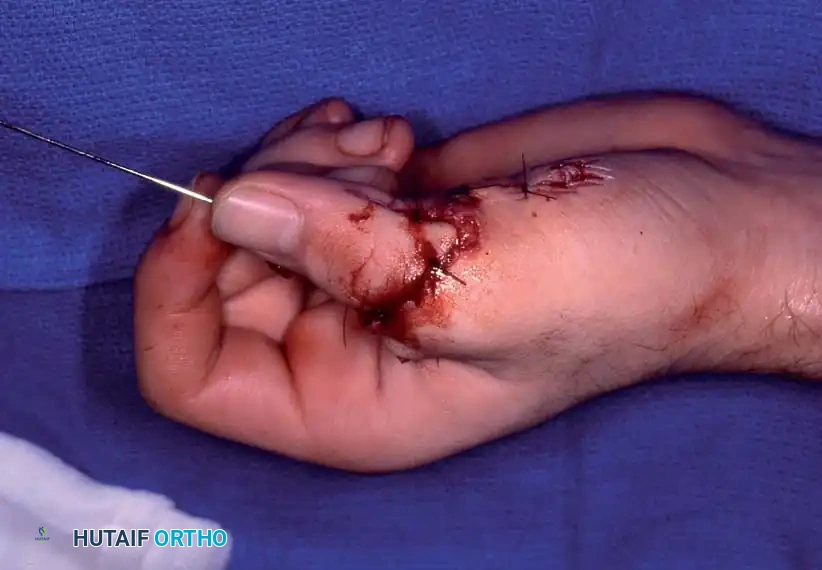
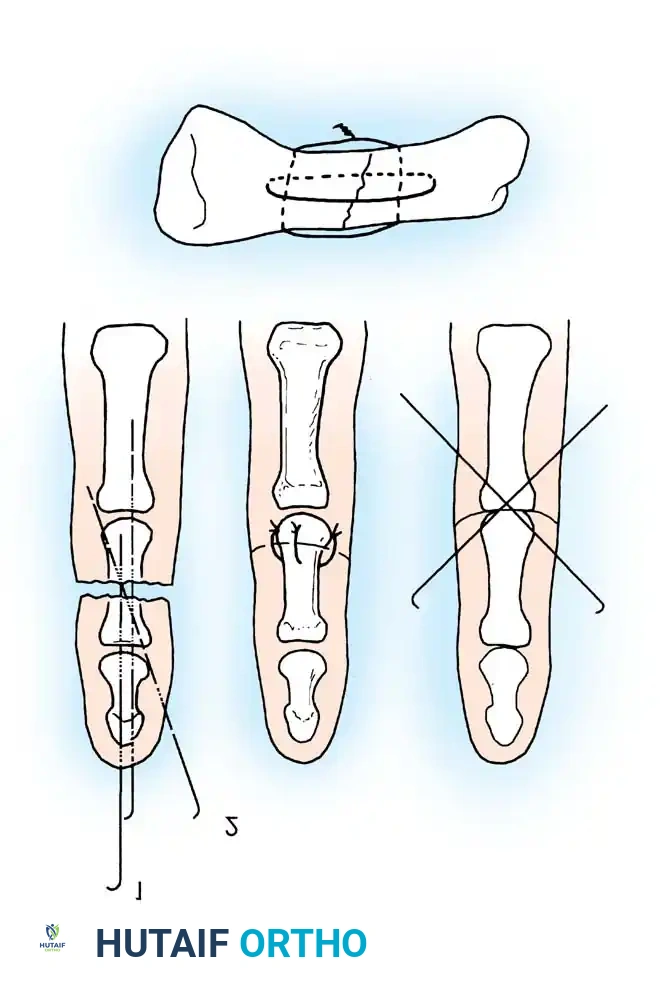
Rigid or semi-rigid osteosynthesis is required to allow early mobilization and prevent shearing forces across the microvascular repairs. Techniques include longitudinal K-wires, crossed K-wires, 90-90 intraosseous wiring, or mini-fragment plates. Intraosseous wiring (often combined with a single oblique K-wire for rotational stability) provides excellent biomechanical stability while maintaining a low profile, minimizing interference with the overlying extensor mechanism. Following skeletal stabilization, the extensor tendons are repaired using strong core sutures (e.g., figure-of-eight or modified Kessler techniques) to restore the dorsal stabilizing forces of the digit.
The operating microscope is then brought into the surgical field for the microvascular and microneural phases. Arteries are typically repaired first to minimize ischemia time and flush out toxic metabolites. The intima must be rigorously inspected under high magnification; any "ribbon sign," intimal separation, or contusion dictates further resection. End-to-end anastomoses are performed using 9-0 or 10-0 nylon interrupted sutures. If a tension-free repair is impossible, interpositional vein grafts must be utilized. Following arterial reperfusion, primary epineurial or group fascicular nerve repair is performed. Finally, the venous anastomoses are completed, aiming for a 2:1 or 3:1 vein-to-artery ratio. The skin must be closed loosely; if closure is tight, fasciotomies or local skin grafts must be employed to prevent compartment syndrome and vascular compression.


Complications, Incidence Rates, and Salvage Management
Despite flawless surgical technique, extremity replantation is fraught with profound postoperative complications. The most immediate and devastating complication is microvascular thrombosis, which typically occurs within the first 48 to 72 hours. Arterial thrombosis presents with a pale, cool, and empty digit lacking capillary refill. Venous thrombosis, which is statistically more common, presents with a blue, engorged, and tense digit with excessively rapid capillary refill that bleeds dark blood when pricked. The distinction is critical, as the salvage pathways differ significantly.
Salvage of a failing replant requires immediate intervention. If conservative measures (lowering the limb for arterial insufficiency, elevating for venous congestion, adjusting room temperature, or administering systemic boluses of heparin) fail to improve perfusion within 30 minutes, emergent surgical re-exploration is mandatory. In cases of venous congestion where no anastomotic salvage is possible, the application of medicinal leeches (Hirudo medicinalis) can provide temporary venous outflow. The leech saliva contains hirudin, a potent local anticoagulant, which allows the bite wound to ooze continuously, decompressing the digit until neovascularization occurs (typically 5 to 7 days).
Late complications are nearly universal and significantly impact the patient's ultimate quality of life. Cold intolerance is experienced by almost all replantation patients. Studies by Povlsen et al. have demonstrated that this cold-induced vasospasm does not physiologically improve over time; rather, patients perceive improvement because they adapt their behavioral habits to avoid cold exposure. Nonunion or malunion of the osseous structures occurs in 10% to 15% of cases, necessitating secondary bone grafting or corrective osteotomies. Tendon adhesions and severe joint stiffness are ubiquitous, particularly in Zone II flexor tendon injuries, frequently requiring secondary tenolyses, capsulotomies, or staged tendon reconstructions months after the initial replantation.
Systemic complications are a grave concern in major limb replantations (proximal to the wrist). Ischemia-reperfusion injury releases a cascade of toxic metabolites, including potassium, lactic acid, and myoglobin, into the systemic circulation. This can precipitate life-threatening hyperkalemia, metabolic acidosis, and acute renal failure secondary to myoglobinuric cast nephropathy. Aggressive intravenous hydration, urine alkalinization, and vigilant monitoring in an intensive care setting are absolute requirements. In severe cases, prophylactic fasciotomies of the replanted limb are mandatory to prevent compartment syndrome secondary to reperfusion edema.
| Complication | Estimated Incidence | Pathophysiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Arterial Thrombosis | 10% - 15% | Intimal damage, tension, vasospasm | Emergent re-exploration, vein grafting, systemic vasodilators |
| Venous Congestion | 15% - 25% | Inadequate vein repair, tight skin closure | Suture release, medicinal leeches (Hirudo medicinalis), Heparin |
| Cold Intolerance | 80% - 100% | Loss of sympathetic autoregulation | Behavioral adaptation, biofeedback, calcium channel blockers |
| Tendon Adhesions | 40% - 60% | Scar formation in Zone II, prolonged immobilization | Aggressive hand therapy, secondary surgical tenolysis |
| Nonunion/Malunion | 10% - 15% | Inadequate fixation, infection, avascular necrosis | Revision osteosynthesis, autologous bone grafting |

Phased Post-Operative Rehabilitation Protocols
The functional success of an extremity replantation is inextricably linked to the rigor and precision of the postoperative rehabilitation protocol. Surgery merely sets the stage; therapy dictates the outcome. The immediate postoperative phase (Days 0 to 14) prioritizes vascular survival over all other concerns. The extremity must be immobilized in a well-padded, non-constrictive plaster splint in the exact position of function that was maintained throughout the microvascular procedure. Elevation of the limb is critical to promote venous drainage, but the surgeon must be cautious: excessive elevation above the level of the heart can compromise arterial inflow in a marginally perfused digit.
During this initial phase, postoperative monitoring is intensive. Clinical observation of color, capillary refill, tissue turgor, and temperature is supplemented by objective monitoring modalities such as surface temperature probes, pulse oximetry, or laser Doppler flowmetry. A drop in surface temperature of more than 2°C or an absolute temperature below 30°C is highly indicative of impending vascular compromise. Anticoagulation protocols vary widely by institution but frequently include a combination of aspirin, low-molecular-weight dextran, or intravenous heparin, particularly in crush injuries or when extensive vein grafts have been utilized. The patient's room must be kept exceptionally warm to prevent sympathetically mediated peripheral vasospasm.
The early protective motion phase (Weeks 2 to 6) marks the transition from strict immobilization to controlled tendon gliding. The goal is to prevent dense peritendinous adhesions while strictly protecting the fragile microvascular anastomoses, nerve repairs, and healing osteosyntheses. Protocols such as the modified Kleinert or Duran techniques are frequently employed for flexor tendon repairs. These involve dynamic extension splinting with controlled, passive flexion exercises. The therapist must possess a deep understanding of the exact surgical sequence and the tensile strength of the repairs to avoid catastrophic rupture of the reconstructed tissues.
The intermediate and late phases (Weeks 6 through 12 and beyond) focus on aggressive active range of motion, progressive strengthening, and sensory re-education. Once radiographic evidence of bone healing is confirmed, dynamic splinting is gradually weaned. Strengthening exercises utilizing putty, hand dynamometers, and functional tasks are initiated. Sensory re-education is a critical component of the late phase; as regenerating axons reach the distal mechanoreceptors, the patient must be retrained to interpret altered sensory afferents. Desensitization techniques (using various textures, vibration, and fluidotherapy) are employed to manage hyperesthesia. The ultimate goal is to return the patient to their previous employment, which may require specialized work hardening programs and functional capacity evaluations.

Summary of Landmark Literature and Clinical Guidelines
The evolution of extremity replantation is thoroughly documented in the orthopedic and microsurgical literature, providing a robust evidence base for current clinical guidelines. Overall survival rates reported by major U.S. and international centers consistently range from 50% to 92% for replanted and revascularized parts. Major limb replantations (proximal to the radiocarpal joint) demonstrate a slightly lower survival rate of 40% to 80%, reflecting the devastating systemic impact of large muscle mass ischemia. The level of amputation significantly impacts survival statistics: below-elbow replantations generally fare better than above-elbow injuries. Historical data from the Beijing Trauma Hospital reported 61% survival for above-elbow and 37% for below-elbow, whereas Ikuta’s series reported 88% and 80%, respectively. Replantations at or just proximal to the wrist show uniformly optimistic survival rates in the 80% to 90% range.
However, modern clinical guidelines emphasize that success cannot be measured by tissue survival alone; it is ultimately dictated by the return of useful, integrated function. Graham et al. conducted a landmark retrospective evaluation of 22 patients with successful upper extremity replantations at or proximal to the wrist against 22 matched amputees fitted with advanced upper-extremity prosthetics. In closely matched adult below-elbow injuries, the replantation group demonstrated 50% good to excellent functional outcomes, whereas the prosthetic group had none, unequivocally validating the functional superiority of biological replantation over prosthetic substitution in appropriately selected patients.
To standardize the evaluation of these complex, multisystem injuries, Ch’en et al. developed a comprehensive functional grading system that remains the gold standard in academic literature. The Ch’en Criteria classify outcomes into four grades. Grade I
Clinical & Radiographic Imaging Archive


