Mastering Hand Revascularization: A Comprehensive Intraoperative Guide to Sympathectomy, Microvascular Reconstruction, and Embolectomy

Key Takeaway
This intraoperative masterclass provides a comprehensive guide to surgical management of hand vasospastic and vaso-occlusive diseases. Fellows will learn precise techniques for digital sympathectomy, microvascular revascularization, and embolectomy. We cover detailed anatomy, meticulous surgical steps, critical pearls and pitfalls, and essential postoperative care, ensuring optimal outcomes for patients with compromised hand perfusion.
Comprehensive Introduction and Patho-Epidemiology
The management of ischemic conditions of the upper extremity represents one of the most formidable challenges in modern orthopedic and plastic hand surgery. Patients presenting with advanced vasospastic and vaso-occlusive diseases—ranging from severe, refractory Raynaud's phenomenon to acute embolic events and chronic microvascular thrombosis—stand at the precipice of catastrophic tissue loss. These pathologies, if not managed with aggressive, precise, and biologically sound surgical interventions, inexorably lead to chronic, excruciating ulcerations, profound functional debilitation, and ultimately, digital amputation. The overarching objective of surgical intervention in this domain transcends mere procedural execution; it is fundamentally about the restoration of vital nutritional blood flow, the modulation of aberrant sympathetic tone, and the preservation of the intricate biomechanical function of the hand.
To master hand revascularization, the operating surgeon must possess a nuanced understanding of the underlying patho-epidemiology distinguishing vasospastic from vaso-occlusive diatheses. Vasospastic disorders, quintessentialized by Raynaud's syndrome, are characterized by episodic, profound constriction of the digital microvasculature. This is driven by a pathological amplification of sympathetic nervous system tone, frequently compounded by structural narrowing secondary to intimal hyperplasia and smooth muscle hypertrophy. Triggers such as cold exposure, vibratory trauma, and emotional stress precipitate these ischemic cascades. Primary Raynaud's disease is often benign, but secondary Raynaud's phenomenon—frequently associated with systemic connective tissue disorders like scleroderma, systemic lupus erythematosus (SLE), and rheumatoid arthritis—portends a much higher risk of irreversible tissue necrosis.
Conversely, vaso-occlusive disorders manifest as a critical reduction in the cross-sectional area of the vessel lumen. This mechanical obstruction can be the sequela of acute thrombosis, distal embolization originating from proximal cardiac or atherosclerotic sources, or focal stenotic lesions inherent to conditions like Buerger’s disease (thromboangiitis obliterans) and hypothenar hammer syndrome. In the latter, repetitive blunt trauma to the hypothenar eminence induces intimal damage, aneurysm formation, and subsequent thrombosis of the ulnar artery, frequently showering microemboli into the digital circulation. Understanding these distinct yet occasionally overlapping pathophysiological mechanisms is absolute prerequisite for selecting the appropriate surgical armamentarium, be it adventitial sympathectomy to relieve spasm, or microvascular bypass and embolectomy to restore luminal patency.
Detailed Surgical Anatomy and Biomechanics
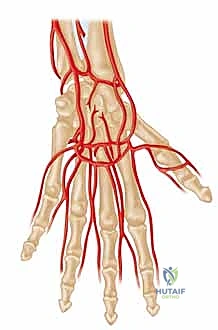
Arterial Architecture and the Palmar Arches
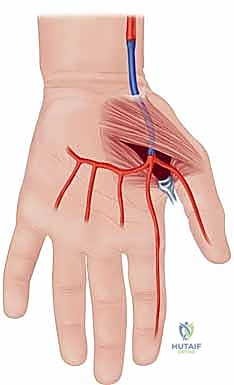
Before a single incision is conceptualized, an exhaustive mastery of the hand's vascular architecture is paramount; in this anatomical theater, precision is synonymous with prevention. The primary arterial inflow to the hand is derived from the radial and ulnar arteries, which originate from the bifurcation of the brachial artery at the antecubital fossa. The ulnar artery, typically the dominant vessel, courses distally to form the superficial palmar arch, located superficially within the mid-palm, deep only to the palmar aponeurosis. This arch serves as the major arterial conduit supplying the ulnar aspect of the digits, giving rise to the common digital arteries.
The radial artery, after traversing the anatomical snuffbox and piercing the first dorsal interosseous muscle, primarily forms the deep palmar arch. This structure lies more proximally and deeply within the palm, resting directly upon the metacarpal bases and interosseous muscles, and predominantly supplies the radial aspect of the hand, including the thumb and index finger. In approximately 80% of the patient population, these two arches are in continuous communication, forming a complete palmar arch system that provides robust, redundant collateral circulation. However, the presence of an incomplete arch significantly amplifies the risk of catastrophic ischemia should one primary inflow vessel become compromised. Furthermore, anatomical variants such as a persistent median artery—which accompanies the median nerve through the carpal tunnel—can contribute significantly to digital perfusion and must be identified during preoperative mapping.
Neurovascular Relationships and Sympathetic Innervation
The regulation of vascular tone in the upper extremity is dictated by sympathetic nerve fibers that originate in the spinal cord, typically exiting via the second and third thoracic nerve roots. These preganglionic fibers synapse in the sympathetic chain, and postganglionic fibers traverse the brachial plexus, ultimately distributing along the major arterial trunks. Critically for the hand surgeon, these sympathetic fibers do not travel as distinct, isolated nerves in the distal extremity; rather, they are intricately embedded within the adventitial layer of the arteries themselves.
As the common digital arteries bifurcate into the proper digital arteries, they are intimately accompanied by the proper digital nerves, forming the neurovascular bundles of the digits. This relationship is of profound surgical significance. During a digital sympathectomy, the primary objective is the meticulous excision of this adventitial layer to disrupt sympathetic signaling. Because the adventitia is physically contiguous with the surrounding connective tissue and lies mere millimeters from the digital nerve, extreme microsurgical dexterity is required to achieve complete adventitial stripping without inflicting iatrogenic neuropraxia or structural damage to the arterial media.
Muscular Intervals and Osteology
While the primary focus of revascularization is the neurovascular bundle, safe and efficient access necessitates a thorough understanding of the surrounding muscular intervals and osteology. Proximal control, when required, involves navigating the medial bicipital groove to isolate the brachial artery. In the forearm, the radial artery is accessed via the interval between the brachioradialis and the flexor carpi radialis, whereas the ulnar artery is approached deep to the flexor carpi ulnaris.
Within the complex topography of the palm, dissection proceeds through the intricate layers of the intrinsic musculature and fascial septa. The carpal bones form the rigid floor of the carpal tunnel and Guyon’s canal, housing structures that must be rigorously protected during proximal palmar dissection. Surgical incisions, particularly the classic Bruner zig-zag approach, are meticulously designed to respect these underlying structures, crossing flexion creases at oblique angles to mitigate the risk of postoperative scar contracture, thereby preserving the delicate biomechanical balance of digital flexion and extension.
Exhaustive Indications and Contraindications
Diagnostic Criteria and Decision Making
The decision to proceed with surgical revascularization or sympathectomy is complex and must be predicated on a rigorous evaluation of the patient's clinical trajectory and objective hemodynamic data. Surgery is rarely the first line of defense; it is reserved for patients who have demonstrated recalcitrance to maximal medical therapy. This includes failed trials of calcium channel blockers, phosphodiesterase inhibitors (e.g., pentoxifylline, sildenafil), topical or systemic nitrates, prostacyclin analogs, and sometimes botulinum toxin A injections.
The primary clinical indications include progressive, unrelenting pain at rest, the development of ischemic digital ulcerations, or impending gangrene. In the context of vasospastic disease, a periarterial digital sympathectomy is indicated when symptoms are severe and progressive, provided there is no major proximal occlusion of the radial or ulnar arteries, and adequate distal target vessels (at least three patent common digital arteries) can be visualized angiographically. Conversely, in vaso-occlusive disease—such as an acute embolus or hypothenar hammer syndrome—direct arterial reconstruction, embolectomy, or vein graft bypass is mandated to bridge the occluded segment and restore inline pulsatile flow.
Indications and Contraindications Matrix
| Clinical Scenario | Primary Indications for Surgery | Absolute Contraindications | Relative Contraindications |
|---|---|---|---|
| Severe Raynaud's Syndrome | Intractable pain, non-healing digital ulcers, failure of maximal medical therapy (CCBs, PDE5 inhibitors, Botox). | Active, profound systemic sepsis; inability to tolerate anesthesia. | Active smoking (patient refusal to quit); severe, uncorrected coagulopathy. |
| Hypothenar Hammer Syndrome | Ulnar artery aneurysm, distal microembolization, digital ischemia, claudication of the hand. | Lack of viable distal run-off vessels for bypass; asymptomatic incidental finding. | Extensive proximal atherosclerotic disease precluding adequate inflow. |
| Acute Embolic Event | Sudden onset pallor, pulselessness, pain, paresthesia, paralysis (the 5 Ps) indicating acute limb/digit threat. | Irreversible tissue necrosis/gangrene (requires amputation instead). | Delayed presentation where ischemic time exceeds viability threshold. |
| Buerger's Disease (TAO) | Severe ischemic rest pain, ulceration despite absolute smoking cessation. | Active tobacco use (surgery will almost universally fail). | Extensive distal microvascular obliteration (no bypass targets). |
Pre-Operative Planning, Templating, and Patient Positioning
Clinical and Hemodynamic Evaluation
Every successful microvascular intervention is architected long before the patient enters the operating theater. Preoperative planning must be exhaustive. The clinical examination focuses heavily on assessing the adequacy of perfusion and the patency of collateral networks. The modified Allen's test is a critical bedside maneuver; by sequentially occluding and releasing the radial and ulnar arteries, the surgeon can ascertain the dominance of the palmar arch and determine which vessel, if any, can be safely sacrificed or utilized as an inflow source for a bypass graft.
Beyond palpation, non-invasive hemodynamic testing provides objective quantification of ischemia. Doppler ultrasonography is utilized to map arterial signals, while digital photoplethysmography (PPG) waveform analysis helps differentiate between fixed occlusive disease (blunted waveforms) and vasospastic disease (waveforms that normalize with warming). Segmental arterial pressure measurements and the calculation of digital-brachial indices (DBI) are essential; a DBI of less than 0.7 suggests significant occlusive disease, and absolute digital pressures below 30 mm Hg correlate strongly with an inability to heal ischemic ulcerations.
Advanced Imaging Modalities
While non-invasive tests provide physiological data, high-resolution imaging is the definitive roadmap for surgical navigation. Conventional digital subtraction angiography (DSA) remains the gold standard for evaluating the intricate microvasculature of the hand. It provides unparalleled spatial resolution, allowing the surgeon to pinpoint the exact anatomical location of stenoses, occlusions, aneurysms, and collateral networks. We meticulously study these angiograms to identify optimal, disease-free proximal inflow vessels and viable distal outflow targets for potential interposition vein grafting.
In modern practice, CT angiography (CTA) and MR angiography (MRA) are increasingly utilized as less invasive alternatives, particularly for evaluating proximal upper extremity vasculature. However, their utility in visualizing the distal digital arteries is often limited by spatial resolution and artifact. If a systemic or cardiac etiology is suspected, particularly in cases of acute embolic phenomena, an echocardiogram and a comprehensive hypercoagulable workup (including screening for antiphospholipid syndrome, Factor V Leiden, and connective tissue serologies) are mandatory to prevent recurrent postoperative occlusion.
Operating Room Setup and Patient Positioning
The choreography of the operating room is critical for minimizing ischemic time and optimizing microsurgical precision. The patient is positioned supine with the affected extremity extended onto an appropriately padded, radiolucent hand table. The arm is abducted to approximately 90 degrees, the elbow slightly flexed, and the wrist supported in mild extension to splay the palmar structures. A proximal upper arm pneumatic tourniquet is applied over generous padding. A completely bloodless field is an absolute prerequisite for the delicate micro-dissection and anastomoses required; the tourniquet time and inflation pressure must be rigorously monitored.
Anticipating the potential need for an autologous vein graft—a frequent necessity in reconstructive revascularization—a secondary surgical site must be prepared. Typically, the ipsilateral or contralateral lower extremity is prepped and draped to allow access to the greater saphenous vein. Alternatively, the cephalic vein of the contralateral arm may be utilized. The operating microscope, equipped with dual-head observation for the primary surgeon and assistant, is brought into the field. High-quality microsurgical instruments, including jeweler's forceps, adventitial scissors, and micro-vessel dilators, are arranged, and the room temperature is elevated to mitigate environmentally induced vasospasm during the procedure.
Step-by-Step Surgical Approach and Fixation Technique
Incisional Strategy and Initial Exposure
The surgical approach for hand revascularization and sympathectomy demands meticulous soft tissue handling. For access to the palmar arch and digital arteries, we employ classic Bruner zig-zag incisions. These incisions begin in the distal palm and extend proximally from the proximal phalanges, carefully designed so that the apices of the flaps fall at the mid-axial lines and the limbs cross the flexion creases obliquely. This geometric configuration is critical; linear incisions across flexion zones inevitably lead to hypertrophic scarring and debilitating flexion contractures.
The skin is incised utilizing a #15 blade, proceeding through the epidermis and dermis. Fine dissecting scissors are then employed to elevate the full-thickness skin flaps, preserving the subdermal vascular plexus to ensure flap viability. As the subcutaneous fat is parted, the palmar aponeurosis is encountered and longitudinally incised. Retraction is achieved using self-retaining lead hands or fine skin hooks, minimizing crush injury to the delicate tissues. At this juncture, the operating microscope is draped and brought into the field, providing 10x to 20x magnification for the critical neurovascular dissection.
Flatt Digital Sympathectomy Technique
The Flatt Digital Sympathectomy is the cornerstone procedure for medically refractory Raynaud's phenomenon with patent inflow. The objective is the precise mechanical ablation of the sympathetic nerve fibers traveling within the arterial adventitia. Under high magnification, the common digital arteries and their proper digital branches are identified as they emerge from beneath the superficial palmar arch.
The first critical step is the isolation of the digital artery from the adjacent proper digital nerve. These structures are intimately bound by delicate fascial bands. Using fine micro-forceps and micro-scissors, the surgeon meticulously separates the artery from the nerve over a distance of 1.0 to 2.0 cm. Extreme vigilance is maintained to avoid any traction or direct trauma to the nerve, which could precipitate a painful postoperative neuroma.
Once the artery is isolated, the adventitial stripping commences. The surgeon stabilizes the arterial wall with one set of non-toothed jeweler's forceps. With a second set of forceps, the thin, translucent outer adventitial layer is grasped. Using a highly controlled, peeling motion—akin to removing the thin skin from a grape—the adventitia is stripped circumferentially from the underlying muscularis media.

As the adventitia is removed, the visual appearance of the artery changes dramatically; it transitions from a slightly opaque, tethered vessel to a smooth, highly translucent, and often visibly dilated conduit. This visual cue is the hallmark of a successful sympathectomy.
Concurrently, the surgeon must identify and sharply divide any microscopic tethering branches or fine neural connections bridging the proper digital nerve and the arterial wall, as these frequently carry aberrant sympathetic fibers.
Radical Digital Sympathectomy and Microvascular Considerations
In patients presenting with profound, widespread vasospasm or severe ischemic ulcerations involving multiple digits, a localized Flatt sympathectomy may be insufficient. In these severe cohorts, a radical or extensive digital sympathectomy is indicated. This highly aggressive approach involves skeletonizing the arterial tree from the distal forearm down to the proper digital arteries.
The dissection begins proximally, stripping the adventitia from the distal radial and ulnar arteries as they enter the wrist. The superficial palmar arch is entirely exposed and denuded of its adventitial layer.
This extensive dissection requires navigating the complex neural anatomy of the palm, particularly the branches of the median and ulnar nerves, ensuring they are gently retracted and protected.
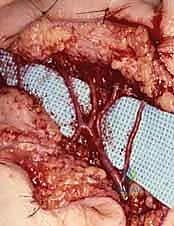
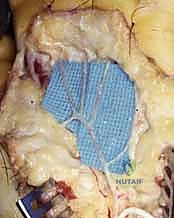
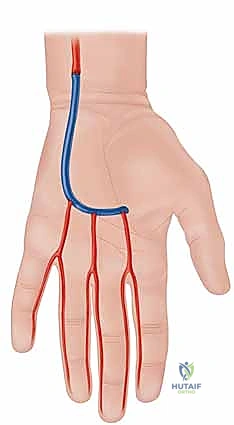
If, during the exploration, an area of fixed occlusion or a thrombosed aneurysm (such as in hypothenar hammer syndrome) is encountered, the procedure transitions from sympathectomy to microvascular reconstruction. The diseased arterial segment is resected until healthy, pulsatile intima is visualized proximally and distally. An autologous reversed saphenous vein graft is harvested, prepared, and interposed into the defect. End-to-end microvascular anastomoses are performed using 8-0 or 9-0 non-absorbable monofilament sutures under the microscope, ensuring precise intimal coaptation to prevent turbulent flow and re-thrombosis.
Upon completion of either sympathectomy or bypass, the tourniquet is deflated. The surgeon observes the extremity for the return of brisk capillary refill and the resolution of pallor. Topical vasodilators, such as papaverine or lidocaine, may be applied directly to the vessels to counteract any mechanically induced vasospasm. Meticulous hemostasis is achieved using bipolar electrocautery before the skin flaps are loosely approximated to accommodate postoperative edema.
Complications, Incidence Rates, and Salvage Management
Intraoperative and Early Postoperative Complications
Despite meticulous technique, hand revascularization and sympathectomy carry inherent risks. Intraoperative complications are primarily technical. Arterial perforation or intimal tearing during adventitial stripping is a catastrophic event that can immediately convert a vasospastic digit into an ischemic one. If this occurs, primary microvascular repair or interposition vein grafting must be performed immediately. The incidence of iatrogenic arterial injury in experienced hands is less than 1%.
Nerve injury is another significant concern. The intimate relationship between the digital arteries and nerves makes the nerves highly susceptible to traction injury or inadvertent transection. Postoperative dysesthesias, numbness, or the development of a painful neuroma occur in approximately 2% to 5% of cases. Early postoperative complications include hematoma formation, which can compress the newly sympathectomized vessels and induce secondary ischemia. Therefore, rigorous hemostasis prior to closure is non-negotiable. Wound dehiscence or superficial infection can also occur, particularly in patients with underlying connective tissue diseases or those on chronic immunosuppressive therapy.
Complications and Salvage Strategies
| Complication | Estimated Incidence | Pathophysiology & Clinical Presentation | Salvage Strategy & Management |
|---|---|---|---|
| Arterial Perforation / Thrombosis | < 1% | Intimal damage during stripping leads to acute platelet aggregation and thrombosis. Presents as an acutely white, pulseless digit post-tourniquet deflation. | Immediate re-exploration. Resection of the damaged arterial segment and microvascular reconstruction with a reversed vein graft. |
| Digital Nerve Injury / Neuroma | 2% - 5% | Traction neuropraxia or inadvertent sharp transection during dissection. Presents as persistent numbness or exquisite, localized pain along the nerve tract. | For suspected transection, immediate primary epineural repair. For delayed neuroma, surgical excision and nerve capping or burying into muscle/bone. |
| Postoperative Hematoma | 1% - 3% | Inadequate hemostasis prior to closure. Presents as excessive swelling, pain, and potentially compromised distal perfusion due to mass effect. | Bedside evacuation if small; return to the OR for formal exploration, evacuation, and bipolar cauterization of the bleeding vessel if expanding. |
| Recurrence of Ischemic Symptoms | 15% - 30% (Long-term) | Incomplete adventitial stripping, regeneration of sympathetic pathways, or progression of the underlying systemic disease (e.g., severe scleroderma). | Optimization of medical therapy (prostacyclins, PDE5 inhibitors). In severe cases, consideration of chemical sympathectomy (Botox) or revision surgery/amputation. |
Phased Post-Operative Rehabilitation Protocols
Acute Phase and Wound Healing
The postoperative rehabilitation protocol is as critical to the ultimate functional outcome as the surgical intervention itself. In the immediate acute phase (Days 0 to 14), the primary goals are the optimization of perfusion, the prevention of hematoma, and the promotion of primary wound healing. The hand is placed in a bulky, non-compressive soft dressing, augmented with a volar orthosis resting the wrist in slight extension and the metacarpophalangeal joints in 70 degrees of flexion, while allowing the interphalangeal joints to remain free.
Strict elevation of the extremity above the level of the heart is enforced to minimize interstitial edema, which can compress the microvasculature. The patient is placed in a warm environment, and cold exposure is strictly prohibited. If a microvascular anastomosis was performed, the patient may be maintained on a regimen of low-molecular-weight heparin or aspirin to mitigate the risk of early microvascular thrombosis. Active and passive range of motion of the uninvolved joints (shoulder, elbow) is encouraged immediately. Gentle, protected active range of motion of the digits may begin within the first few days, depending on the stability of the wound and the surgeon's preference, to prevent flexor tendon adhesions.
Subacute Phase and Functional Restoration
As the incisions heal and sutures are removed (typically around two weeks postoperatively), the patient transitions into the subacute phase of rehabilitation (Weeks 2 to 6). The bulky dressings are discontinued, and scar management techniques are initiated. This includes gentle scar massage, the application of silicone elastomer sheets, and potentially the use of compression garments (such as Isotoner gloves), provided they do not compromise digital perfusion.
Supervised hand therapy becomes intensive during this phase. The focus shifts towards restoring full active and passive range of motion of the digits. Tendon gliding exercises and intrinsic muscle stretching are emphasized to counteract the tendency for scar contracture along the Bruner incisions. If the digital nerves were manipulated extensively during the sympathectomy, sensory re-education protocols are implemented to help the brain interpret altered sensory signals and minimize hypersensitivity. Strengthening exercises are generally delayed until 6 to 8 weeks postoperatively, ensuring that the vascular reconstruction is fully mature and capable of withstanding the increased metabolic demands of exercising muscle. Absolute cessation of tobacco use remains a lifelong mandate, as continued smoking is the single greatest predictor of late surgical failure and recurrent ischemia.
Summary of Landmark Literature and Clinical Guidelines
Historical Context and Modern Paradigm Shifts
The evolution of surgical intervention for hand ischemia is deeply rooted in the pioneering work of early hand surgeons. The concept of peripheral digital sympathectomy was popularized by Adrian Flatt in the late 20th century. Flatt recognized that proximal sympathectomies (e.g., cervical or stellate ganglionectomies) often yielded transient results due to the rapid regeneration of sympathetic pathways and failed to address the localized hyperreactivity of the distal digital vessels. His technique of localized adventitial stripping revolutionized the management of refractory Raynaud's, demonstrating significant improvements in ulcer healing and pain reduction.
Subsequent landmark studies by Koman and colleagues further elucidated the pathophysiology of digital ischemia, differentiating between nutritional capillary blood flow (essential for tissue viability) and thermoregulatory arteriovenous shunt flow. Their research underscored that the primary benefit of sympathectomy is the restoration of nutritional blood flow, which is critical for healing ischemic ulcers, even if cold intolerance is not completely eradicated.
Evidence-Based Guidelines for Revascularization
Modern clinical guidelines, supported by the American Society for Surgery of the Hand (ASSH), emphasize a multidisciplinary, stepwise approach to upper extremity ischemia. Surgery is firmly positioned as a salvage therapy following the exhaustion of advanced pharmacological interventions. For vaso-occlusive diseases, the literature clearly supports aggressive microvascular reconstruction. Studies evaluating the outcomes of vein grafting for hypothenar hammer syndrome demonstrate patency rates exceeding 80% at five years, provided the patient adheres to strict smoking cessation.
In the realm of vasospastic disease, a systematic review of digital sympathectomy outcomes reveals that while it is highly effective for healing existing ulcers (success rates often exceeding 85%), it is not a definitive cure for the underlying systemic disease. Patients with secondary Raynaud's phenomenon, particularly those with scleroderma, have a higher risk of symptom recurrence and subsequent ulcer formation compared to those with primary Raynaud's or idiopathic vasospasm. Therefore, the contemporary surgical paradigm dictates that revascularization and sympathectomy must be viewed not as isolated mechanical fixes, but as critical components of a comprehensive, lifelong management strategy for the ischemic hand.
